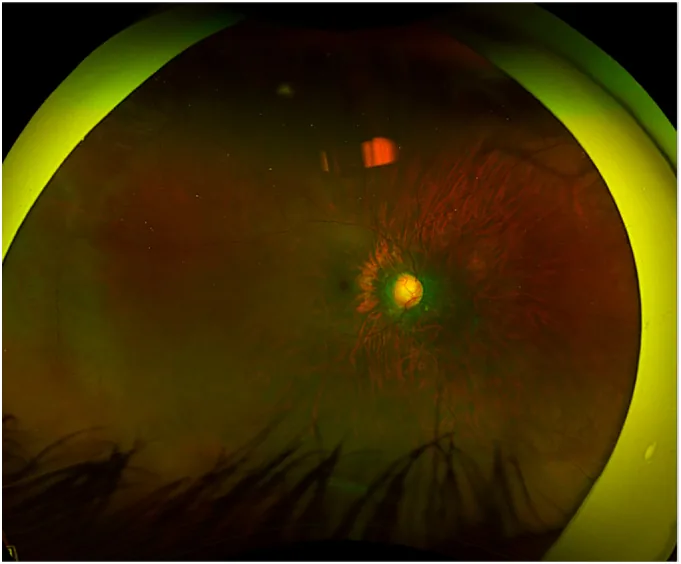
Bamefleh DA, et al. Bleb morphology following mitomycin-C sponge versus subconjunctival injection in deep sclerectomy for pediatric congenital glaucoma: A case report. Int J Surg Case Rep. 2025. Figure 1. PMCID: PMC12510068. License: CC BY.
Wide-angle fundus photograph of the right eye showing optic disc cupping enlargement consistent with glaucoma progression before reoperation. Corresponds to optic disc cupping discussed in section “1. Overview of Glaucoma Eye Drops.”
Glaucoma is a progressive optic neuropathy, and the only modifiable risk factor is intraocular pressure1)4). Current pharmacotherapy aims to lower IOP. IOP is determined by aqueous humor production, conventional outflow through the trabecular meshwork, uveoscleral outflow, and episcleral venous pressure.
Glaucoma eye drops lower IOP by either suppressing aqueous humor production or promoting aqueous humor outflow1)4)5).
Mechanism of Action
Drug Class
Suppression of aqueous humor production
Beta-blockers, alpha-agonists, CAIs
Outflow enhancement
Prostaglandin analogs, ROCK inhibitors, miotics
Prostaglandin (PG) analogs, which have strong intraocular pressure-lowering effects and few systemic side effects, are often the first-line choice 4)5). If the effect is insufficient, it is common to add beta-blockers, then alpha-agonists or CAIs in order.
QWhat is the first-line treatment for glaucoma eye drops?
A
PG analogs are the most frequently prescribed first-line drugs 4)5). This is because they have the greatest intraocular pressure-lowering effect (25–33%), are administered once daily, and have good tolerability. If PG analogs cannot be used due to contraindications, side effects, cost, or patient preference, treatment is started with beta-blockers or alpha-agonists.
PG analogs lower intraocular pressure mainly by enhancing uveoscleral outflow2)4)5). Through modulation of matrix metalloproteinases, they cause remodeling of the extracellular matrix and increased outflow pathway permeability.
Representative drugs include latanoprost, travoprost, bimatoprost, and tafluprost 2)4)5). They lower intraocular pressure by 25–33% and the effect lasts 24 hours with once-daily administration.
Side Effects of PG Analogs
Iris pigmentation: Permanent color change due to increased number of melanosomes 4)5)
Periorbital pigmentation: Pigmentation of the eyelid skin
Conjunctival hyperemia: One of the most common side effects
Eyelash changes: Hypertrichosis and elongation
Periorbital changes (PAPA/DUUS): Deepening of the upper eyelid sulcus
Beta-blockers suppress sympathetic nerve endings in the ciliary epithelium, reducing aqueous humor production and lowering intraocular pressure by 20–25% 4)5).
There are non-selective beta-blockers (timolol, levobunolol, metipranolol, carteolol) and cardioselective beta-blockers (betaxolol) 4)5). Timolol is the most widely used. Nighttime dosing has limited efficacy and may contribute to visual field progression through nocturnal blood pressure reduction 4)5).
Major systemic side effects include bronchospasm, bradycardia, and hypotension 4)5). They should be avoided in patients with asthma, COPD, bradycardia, or atrioventricular block 4)5).
Alpha-2 adrenergic receptor agonists include brimonidine and apraclonidine 4)5).
Brimonidine lowers intraocular pressure by 20–25% through dual action: suppressing aqueous humor production and enhancing uveoscleral outflow4)5). It has similar efficacy to timolol. Allergic conjunctivitis is relatively common; it should be avoided in infants and children due to CNS depression 4)5).
Apraclonidine is mainly used to prevent transient intraocular pressure spikes in the perioperative period. Tachyphylaxis is a problem with long-term use.
They inhibit carbonic anhydrase in the ciliary epithelium, reducing aqueous humor production 4)5).
Topical CAIs (dorzolamide, brinzolamide) lower intraocular pressure by 15–20%. They have fewer systemic side effects than oral CAIs. Dosing is 2–3 times daily. Main side effects are taste disturbance and stinging. They are more effective than other drugs on nighttime intraocular pressure.
Oral CAIs (acetazolamide) are used for short-term management of acute intraocular pressure elevation, but long-term use is limited due to systemic side effects such as metabolic acidosis, paresthesia, and fatigue 1).
Contraction of the ciliary muscle widens the trabecular meshwork and increases aqueous humor outflow 4)5). It lowers intraocular pressure by 15–25%.
Pilocarpine is a representative drug, requiring administration 3–4 times daily. It is particularly useful for pigmentary glaucoma, aphakic glaucoma, and plateau iris syndrome. It is also used as a pretreatment before laser iridotomy.
Main side effects include myopia, decreased vision in dim light due to miosis, and brow ache. Attention should also be paid to the risk of retinal detachment and cataract4)5).
ROCK Inhibitors
Mechanism of action: Relaxes the cytoskeleton of the trabecular meshwork and Schlemm’s canal, facilitating conventional outflow. It also contributes to decreased aqueous humor production and reduced episcleral venous pressure.
Ripasudil: First approved in the world in Japan in 2014. Administered twice daily.
Netarsudil: Approved in the United States in 2017. Administered once daily. Shows similar intraocular pressure reduction to timolol but is inferior to latanoprost.
Main side effects: Conjunctival hyperemia (mild, short-term), corneal verticillata.
Fixed Combinations
Dorzolamide/Timolol: The most widely used fixed combination. Administered twice daily.
Brimonidine/Timolol: Provides greater intraocular pressure reduction than each monotherapy. Administered twice daily.
Brinzolamide/Brimonidine: A fixed combination without timolol. Administered twice daily.
Netarsudil/Latanoprost: ROCK inhibitor + PG combination. Administered once daily. Provides superior intraocular pressure reduction compared to each monotherapy.
QWhat is the role of ROCK inhibitors?
A
ROCK inhibitors are a new class of glaucoma medications that enhance outflow through the conventional pathway via the trabecular meshwork and Schlemm’s canal. In Japan, ripasudil was first approved worldwide in 2014. A fixed combination of netarsudil/latanoprost is also under development. Currently, they are not first-line agents and are often used as add-on therapy. Neuroprotective effects and inhibition of scarring after filtration surgery have been shown in animal models, and future applications are expected.
QWhat are the advantages of fixed combinations?
A
The greatest advantage of fixed combinations is improved adherence. Reducing the number of instillations and medications decreases patient burden. Additionally, the “washout effect” from sequential instillation is eliminated, which may result in better intraocular pressure control than separate administration. Disadvantages include higher cost and difficulty in adjusting individual drug doses.
Intraocular pressure is determined by the balance between aqueous humor production and outflow1)2)3). Aqueous humor is produced by the non-pigmented epithelium of the ciliary body and exits via two main pathways.
In the conventional pathway (trabecular outflow), aqueous humor drains through the trabecular meshwork → Schlemm’s canal → collector channels → episcleral veins1)2)3). In the uveoscleral pathway, aqueous humor flows through the spaces between ciliary muscle fibers into the suprachoroidal space.
Each drug class acts on these outflow pathways or aqueous production. Prostaglandin analogs primarily enhance the uveoscleral pathway, while ROCK inhibitors enhance the conventional pathway. Beta-blockers, alpha-agonists, and CAIs suppress aqueous production2)3)4)5). Miotics contract the ciliary muscle, mechanically widening the trabecular meshwork and enhancing conventional outflow.
ROCK inhibitors are the newest drug class introduced clinically since 2014. In addition to intraocular pressure lowering, neuroprotective effects via increased optic nerve head blood flow have been shown in animal models. They also inhibit fibroblast proliferation and differentiation into myofibroblasts through suppression of TGF-β, potentially reducing scarring after glaucomafiltration surgery. Applications for corneal endothelial diseases are also being studied.
The netarsudil/latanoprost fixed combination acts on both the conventional and uveoscleral pathways, showing superior intraocular pressure reduction compared to each monotherapy.
Emergence of Laser Trabeculoplasty as First-Line Treatment
Based on the results of the LiGHT trial, laser trabeculoplasty (selective laser trabeculoplasty) has been confirmed to have an intraocular pressure-lowering effect equivalent to eye drops and to be cost-effective 2). The EGS and AAO guidelines recommend laser trabeculoplasty as first-line treatment 2)3)4). For patients with adherence issues to medication, laser trabeculoplasty is an ideal option.
Reduction of ocular surface damage through widespread use of preservative-free formulations
Development of sustained-release drug delivery systems
Establishment of optimal drug selection strategies based on personalized treatment
Clinical validation of the neuroprotective effects of ROCK inhibitors
QWhat are the benefits of preservative-free eye drops?
A
Preservatives in glaucoma eye drops (especially benzalkonium chloride) can cause ocular surface inflammation, corneal epithelial damage, and dry eye with long-term use 1). Preservative-free formulations reduce these side effects and are particularly useful for maintaining ocular surface health in patients using multiple eye drops long-term. Maintaining the ocular surface is also important because it affects the success rate of future glaucoma surgery.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021 Jun;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Gedde SJ, Lind JT, Wright MM, Chen PP, Muir KW, Vinod K, Li T, Mansberger SL; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P151-P192. doi:10.1016/j.ophtha.2020.10.023. PMID:33189698.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.