Red eye (hyperemia) is one of the most common complaints in ophthalmology outpatient clinics. It is caused by dilation or bleeding of blood vessels on the ocular surface, and its causes range widely from mild allergic conjunctivitis and dry eye to sight-threatening serious diseases such as acute angle-closure glaucoma attack, corneal ulcer, and endophthalmitis1).
According to reviews in general internal medicine and ophthalmology in Western countries, the most common cause of redness is infectious or allergic conjunctivitis, followed by dry eye, trauma, and contact lens-related diseases 1). On the other hand, diseases with ciliary injection (iridocyclitis, acute glaucoma attack, keratitis) are a minority among all red eye patients, but their visual prognosis is severe if missed, making differential diagnosis of urgency particularly important.
By systematically checking the pattern of redness and accompanying symptoms (eye pain, visual changes, discharge characteristics, contact lens use), high-urgency diseases can be efficiently narrowed down. This article focuses on differential diagnosis based on anatomical classification of redness and assessment of consultation urgency.
Redness is classified into four patterns based on the site and depth of occurrence. This classification is the most important first step in differentiating the underlying disease.
① Conjunctival Injection
Mechanism: Dilation of superficial conjunctival vessels (conjunctival arteries and veins)
Characteristics: Diffuse red hyperemia that is strongest in the fornix (inner side of the eyelid) and becomes thinner toward the limbus. When the eye moves outward, the hyperemic area also moves.
Mechanism: Dilation of the anterior ciliary arteries (deep vessels)
Characteristics: Intense bluish-purple hyperemia around the limbus (corneal edge). The hyperemic area does not move with eye movement. Reflects deep inflammation.
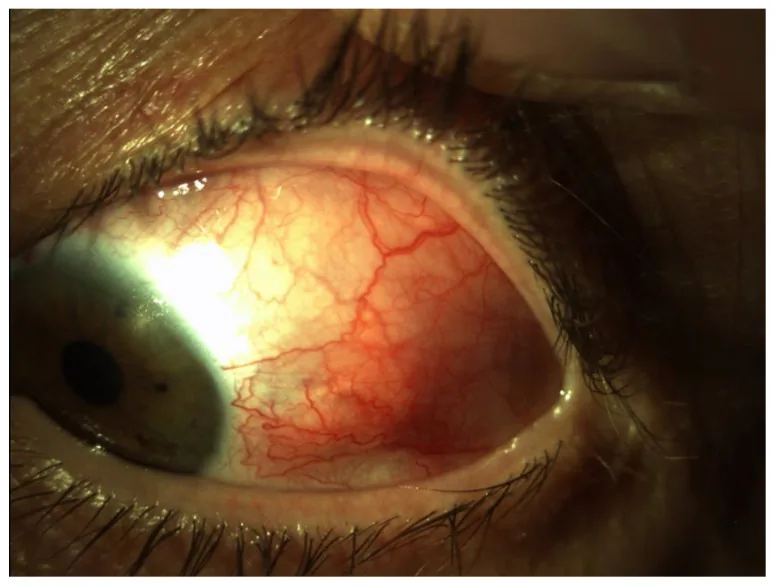
Smeller L, Toth-Molnar E, Sohar N. Optical Coherence Tomography: Focus on the Pathology of Macula in Scleritis Patients. J Clin Med. 2023;12(14):4825. Figure 1. PMID: 37510941; PMCID: PMC10381547; DOI: 10.3390/jcm12144825. License: CC BY.
Anterior segment photograph of diffuse anterior scleritis on the temporal side of the left eye, showing localized dark red hyperemia and vascular dilation. This corresponds to scleral hyperemia (dark red localized redness due to deep vessel congestion) discussed in the section “2. Types of hyperemia (anatomical classification)”.
Mechanism: Congestion of intrascleral vessels (often autoimmune mechanism)
Characteristics: Localized deep dark red hyperemia. Does not disappear with ocular compression. Scleritis is associated with severe eye pain. Episcleritis has mild pain.
Indicated diseases: Anterior scleritis/episcleritis. Often associated with systemic diseases such as rheumatoid arthritis, psoriasis, and inflammatory bowel disease.
Epinephrine eye drop test: Conjunctival hyperemia resolves, but scleritis does not.
④ Subconjunctival Hemorrhage
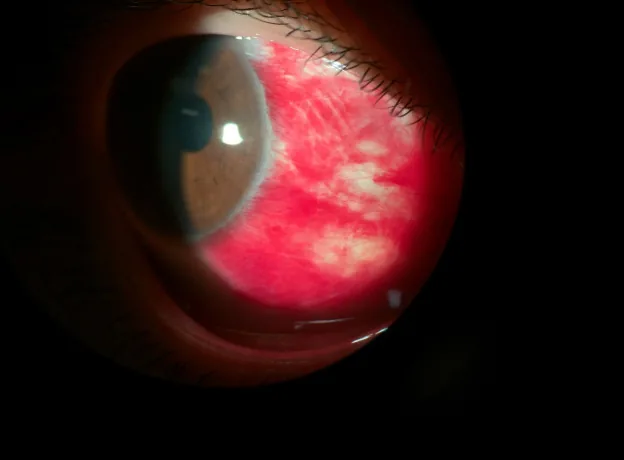
Celebi ARC, Aygun EG. A rare cause of recurrent subconjunctival hemorrhage: ocular vicarious menstruation. GMS ophthalmology cases. 2023;13:Doc05. doi:10.3205/oc000213. PMID:36875630; PMCID:PMC9979076. Figure 1. PMID: 36875630; PMCID: PMC9979076; DOI: 10.3205/oc000213. License: CC BY.
Slit lamp image of the patient’s right eye at the start of menstruation, showing a well-demarcated bright red subconjunctival hemorrhage on the nasal side. This corresponds to subconjunctival hemorrhage (localized bleeding due to vascular rupture) discussed in the section “2. Types of Hyperemia (Anatomical Classification).”
Mechanism: Rupture of subconjunctival blood vessels (blood accumulates between the conjunctiva and sclera)
Features: Localized bright red, well-demarcated hemorrhage. It is not diffuse but rather a “solid” redness. Often not accompanied by vision loss or eye pain.
Indicated diseases/triggers: Hypertension, anticoagulant use, coughing, sneezing, trauma. Usually resolves spontaneously within 1–2 weeks6).
Note: If accompanied by pain or vision loss, rule out trauma or globe perforation.
QWhat is the difference between subconjunctival hemorrhage and conjunctival injection?
A
Conjunctival injection is a condition where the blood vessels of the conjunctiva dilate, causing a diffuse redness. In contrast, subconjunctival hemorrhage is a condition where blood vessels under the conjunctiva rupture and blood accumulates locally, characterized by a well-defined, bright red, patchy hemorrhage. Subconjunctival hemorrhage without pain or vision loss is naturally absorbed within 1 to 2 weeks, and treatment is generally unnecessary6). Hypertension and use of anticoagulants (warfarin, direct oral anticoagulants) are common triggers. If it recurs or is accompanied by pain or vision changes, an ophthalmology consultation is recommended.
3. Main causes of conjunctival injection (differential diagnosis)
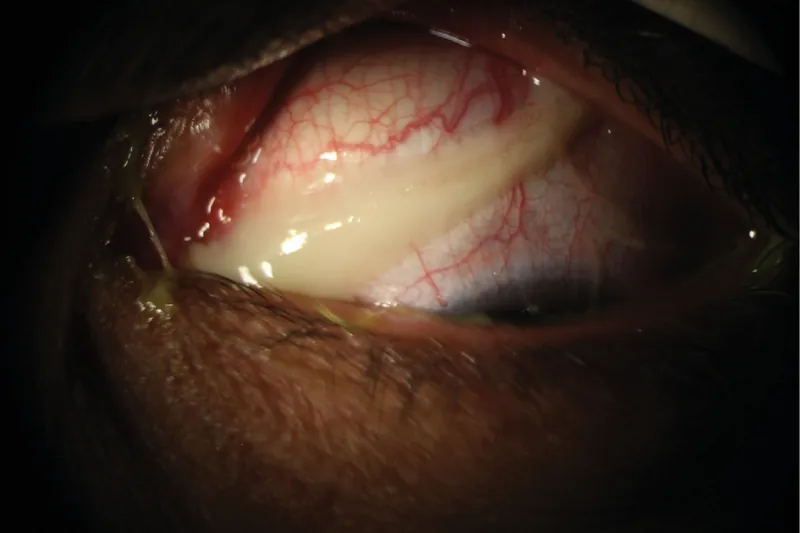
Azari AA, Arabi A. Conjunctivitis: a systematic review. J Ophthalmic Vis Res. 2020 Jul 29;15(3):372-395. Figure 4. PMCID: PMC7431717. License: CC BY.
Clinical image of thick purulent discharge in a patient with acute bacterial conjunctivitis. This corresponds to bacterial conjunctivitis (infectious conjunctivitis characterized by purulent discharge) discussed in section “3. Main causes of hyperemia (differential diagnosis).”
The nature of the discharge is useful for differential diagnosis.
Watery discharge: Suggests viral (adenovirus, herpes). Epidemic keratoconjunctivitis (EKC) is a highly contagious disease caused by adenovirus, and prevention of nosocomial infection is important2). Patients should be advised to avoid school or work for two weeks after onset.
Purulent discharge: Suggests bacterial (Staphylococcus aureus, Streptococcus pneumoniae, Neisseria gonorrhoeae, etc.). Treat with antibacterial eye drops such as levofloxacin 0.5% ophthalmic solution or tobramycin eye drops. Gonococcal conjunctivitis progresses rapidly and carries a risk of corneal perforation.
Mucoid or stringy discharge: Suggests allergic (including vernal catarrh). Use anti-allergic eye drops or antihistamine eye drops.
Hyperemia in contact lens (CL) wearers carries a higher risk of bacterial keratitis, Pseudomonas corneal ulcer, and Acanthamoeba keratitis compared to non-wearers3). A large epidemiological study in Australia reported an annual incidence of microbial keratitis due to CL of approximately 25 per 100,000 soft CL wearers3). Extended wear increases the risk more than 10-fold compared to daily disposable CL3).
The RPS Adeno Detector (adenovirus antigen rapid test) has a sensitivity of 89% and specificity of 94%, enabling rapid diagnosis and aiding in the prevention of nosocomial infection2). If EKC is suspected, isolate the patient and disinfect all instruments used.
4. Key Points for History Taking and Differential Diagnosis
Long-term use of steroids: risk of infectious eye disease and glaucoma
HLA-B27-related diseases (e.g., ankylosing spondylitis): strong association with anterior uveitis (iridocyclitis)
QWhat should be done if the eye becomes red while wearing contact lenses?
A
Remove the contact lenses immediately. If eye pain, decreased vision, or corneal whitening persists after lens removal, see an ophthalmologist on the same day. Redness while wearing contact lenses may indicate bacterial or Pseudomonas corneal infection, which can lead to corneal perforation if left untreated3). Prolonged wear of soft contact lenses or continuous wear of disposable lenses further increases the risk. Using over-the-counter eye drops until seeing an ophthalmologist is not recommended, as it delays appropriate antibiotic treatment.
If a chemical substance enters the eye, irrigate with copious tap water for at least 15 minutes before seeking medical attention 5). Alkaline substances (mold remover, cement, lime, bleach) are particularly severe because they penetrate deep into tissues through saponification of fats, reaching the corneal stroma and anterior chamber. Seek emergency care while irrigating. At the ophthalmology visit, check pH (target pH 7.0–7.4) 5).
Superficial conjunctival vessels (arteries, veins, capillaries) dilate due to inflammatory mediators (histamine, prostaglandins, cytokines) or allergens. In allergic conjunctivitis, IgE-mediated mast cell degranulation releases large amounts of histamine, causing immediate vasodilation and ocular itching. In dry eye, friction and drying stimulation due to tear film instability cause persistent mild inflammation, leading to chronic conjunctival injection. The TFOS DEWS II pathophysiology report states that tear hyperosmolarity induces inflammatory cytokines in corneal and conjunctival epithelium, creating a vicious cycle of chronic redness and foreign body sensation 9).
Ciliary flush results from dilation of the anterior ciliary arteries (deep vessels that penetrate the sclera to supply the ciliary body, iris, and cornea). It directly reflects inflammation or irritation of the iris, ciliary body, and cornea, making it an objective indicator of serious anterior segment disease. In acute glaucoma attack, a rapid rise in intraocular pressure (60–80 mmHg) causes corneal edema and ischemia of the iris root, leading to intense ciliary flush and corneal epithelial edema (causing blurred vision).
Most cases of scleritis are caused by autoimmune mechanisms (especially necrotizing scleritis associated with rheumatoid arthritis). Inflammation causes dilation and congestion of blood vessels within the sclera, and due to poor anastomosis with adjacent vessels, localized dark red congestion occurs. Episcleritis is limited to the episcleral tissue on the scleral surface and has a better prognosis than scleritis, but tends to recur. In the epinephrine (adrenaline) instillation test, conjunctival and episcleral congestion subsides due to vasoconstriction, but deep scleritis does not. This characteristic is sometimes used for differentiation.
Small blood vessels under the conjunctiva rupture due to physical or pressure load (coughing, sneezing, straining, heavy lifting), hypertension, or the effects of anticoagulants, leading to blood accumulation in the subconjunctival space. Because clot formation occurs rapidly via the extrinsic pathway of coagulation factors, massive bleeding is rare. Natural absorption usually takes 1–2 weeks 6). It may be a sign of hypertension, so repeated episodes warrant medical evaluation 6).
Rapid adenovirus antigen tests, such as the RPS Adeno Detector, are effective in preventing nosocomial infections of EKC, and next-generation diagnostic tools aimed at improving false-negative rates are under development 2). Rapid differentiation between infectious and non-infectious conjunctivitis is becoming increasingly important from the perspective of reducing unnecessary antibiotic prescriptions.
AI Application for Differentiating Hyperemia and Dry Eye
Studies have reported automatic classification of the type and severity of hyperemia using machine learning (deep learning) analysis of ocular surface images 7). Non-invasive ocular surface assessment tools using smartphone cameras are also being developed, and their use in primary care and telemedicine is expected.
For severe allergic conjunctival diseases such as vernal keratoconjunctivitis and atopic keratoconjunctivitis, where existing antihistamines and anti-allergic drugs are insufficient, expansion of insurance coverage for tacrolimus ophthalmic solution and ophthalmic application of biologics including omalizumab are being considered 8). The Guidelines for the Diagnosis and Treatment of Allergic Conjunctival Diseases (3rd edition) have organized the positioning of cyclosporine and tacrolimus eye drops for severe cases 8).
Findings from TFOS DEWS III and Dry Eye-Related Hyperemia
The TFOS DEWS II Pathophysiology Report indicates that tear hyperosmolarity and tear film instability drive the inflammatory cascade in the cornea and conjunctiva, and that chronicity of neurosensitization and ocular surface damage leads to persistent hyperemia and discomfort 9). Evidence is accumulating on the efficacy of novel therapeutic targets for dry eye-related hyperemia, such as MUC5AC mucin secretagogues (3% diquafosol sodium ophthalmic solution) and anti-inflammatory eye drops (cyclosporine ophthalmic solution).
Cronau H, Kankanala RR, Mauger T. Diagnosis and management of red eye in primary care. Am Fam Physician. 2010;81(2):137-144.
Sambursky R, Tauber S, Schirra F, et al. The RPS adeno detector for diagnosing adenoviral conjunctivitis. Ophthalmology. 2006;113(10):1758-1764.
Stapleton F, Keay L, Edwards K, Naduvilath T, Dart JK, Brian G, et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology. 2008;115(10):1655-62. doi:10.1016/j.ophtha.2008.04.002. PMID:18538404.
Austin A, Lietman T, Rose-Nussbaumer J. Update on the Management of Infectious Keratitis. Ophthalmology. 2017;124(11):1678-1689. doi:10.1016/j.ophtha.2017.05.012. PMID:28942073; PMCID:PMC5710829.
Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol. 1997;41(4):275-313.
Tarlan B, Kiratli H. Subconjunctival hemorrhage: risk factors and potential indicators. Clinical ophthalmology (Auckland, N.Z.). 2013;7:1163-70. doi:10.2147/OPTH.S35062. PMID:23843690; PMCID:PMC3702240.
Gulshan V, Peng L, Coram M, Stumpe MC, Wu D, Narayanaswamy A, et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA. 2016;316(22):2402-2410. doi:10.1001/jama.2016.17216. PMID:27898976.