Bacterial conjunctivitis is an inflammatory disease of the conjunctiva caused by bacterial infection. The conjunctiva is a mucous membrane that extends from the inner surface of the eyelids (palpebral conjunctiva) through the fornix to the surface of the eyeball (bulbar conjunctiva), where it meets the cornea at the limbus.
This condition is one of the most common infectious diseases encountered in ophthalmology. In the United States, acute infectious conjunctivitis accounts for approximately 1% of primary care visits, with an estimated 4 million cases per year1). While it can affect individuals of all ages, it is more common in children and the elderly.
Most cases are acute and self-limiting, and serious complications are rare. However, due to its high prevalence, the social impact in terms of school and work absenteeism is substantial. Direct and indirect medical costs are estimated to exceed $500 million per year in the United States alone1).
Clinically, it is classified into acute type (common bacterial), hyperacute type (mainly gonococcal), and chronic type (mainly chlamydial). This article primarily focuses on acute bacterial conjunctivitis.
Azari AA, Barney NP. Conjunctivitis: A Systematic Review. J Ophthalmic Vis Res. 2020 Jul 29;15(3):372-395. Figure 4. PMCID: PMC7431717. License: CC BY.
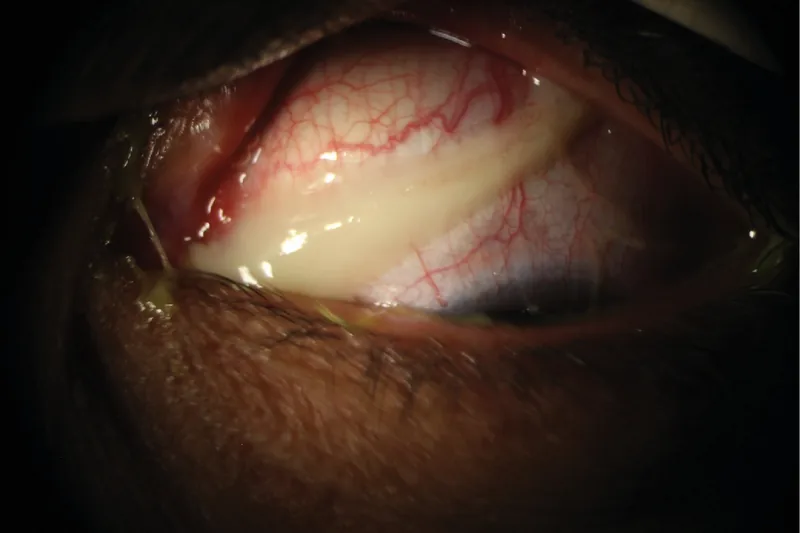
Thick, stringy purulent discharge from the eyelid margin is observed, demonstrating the typical amount of secretion in acute bacterial conjunctivitis. This image easily illustrates the clinical difference from viral or allergic conjunctivitis at a glance.
Bulbar conjunctival injection: Diffuse dilation of conjunctival vessels is observed.
Palpebral conjunctival injection and edema: Papillary reaction is present, but without significant follicular formation.
Mucopurulent discharge: Moderate in amount, but the character varies depending on the causative organism.
Conjunctival edema (chemosis): In severe cases, the bulbar conjunctiva becomes swollen.
Eyelid erythema and swelling: In hyperacute cases (gonococcal), marked eyelid swelling is observed.
Hyperacute (gonococcal conjunctivitis) develops with an incubation period of half a day to 3 days. It is characterized by a large amount of white-yellow, creamy purulent discharge and is also called “blennorrhea.” Corneal ulcers may form early in the disease course and can progress to corneal perforation.
Among bacterial conjunctivitis, there are clinically important subtypes that are not common but significant. Gonococcal conjunctivitis and chlamydial conjunctivitis differ from typical acute bacterial conjunctivitis in their course, testing, and treatment approach.
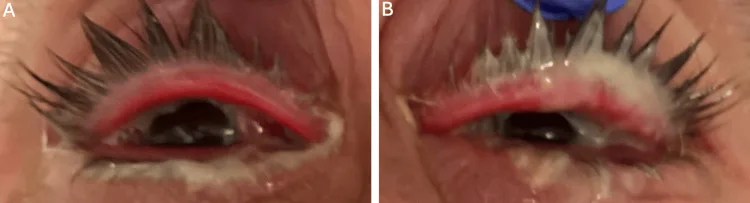
Albear S, LoBue S, Cooley A, Brandenburg T, Friedes R, Park J. Povidone-Iodine as an Adjuvant Therapy for Refractory Gonorrhea Keratoconjunctivitis: A Case Report. Cureus. 2025;17(5):e83676. Figure 1. PMCID: PMC12143893. License: CC BY.
A) Right eye and B) left eye show profuse purulent discharge, mild swelling, and eyelid margin hyperemia. This corresponds to the purulent discharge described in section “2. Main Symptoms and Clinical Findings” for gonococcal conjunctivitis.
Gonococcal conjunctivitis has an acute onset. Suspect it when the following findings overlap.
Acute onset: Worsens within days
Profuse discharge: Reaccumulates quickly even after wiping
Severe conjunctival chemosis: Bulbar conjunctiva is elevated
Corneal involvement: Accompanied by pain, photophobia, and decreased vision
Preauricular lymphadenopathy: More prominent than in acute bacterial conjunctivitis
In adults, infection occurs via finger contact from genital secretions. This is not a disease limited to neonates. If diagnosis is delayed, it can progress to corneal ulcer or corneal perforation7). Obtain conjunctival cultures before starting treatment. When gonococcal infection is suspected, initiate systemic treatment without waiting for culture results8).
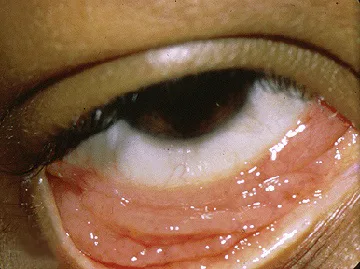
Trobe J. Chlamydial-conjunctivitis.jpg. The Eyes Have It, University of Michigan Kellogg Eye Center. 2011. Source ID: Wikimedia Commons File:Chlamydial-conjunctivitis.jpg. License: CC BY 3.0.
This is a clinical photograph of chlamydial conjunctivitis with the lower palpebral conjunctiva everted. It corresponds to chlamydial follicular conjunctivitis discussed in the “2. Main symptoms and clinical findings” section.
Chlamydial conjunctivitis tends to follow a subacute to chronic course. In adult inclusion conjunctivitis, Chlamydia trachomatis serotypes D–K are involved9).
Often unilateral: may later become bilateral
Persists for 2 weeks or longer: difficult to improve with standard antibacterial eye drops
Prominent follicular formation: large follicles in the lower fornix
Mucopurulent discharge: more purulent than viral conjunctivitis
Preauricular lymphadenopathy: may be tender
Corneal involvement: superficial keratitis and superior limbal infiltration
In adults, genital chlamydial infection may coexist. A systematic review reports that chlamydial conjunctivitis accounts for 1.8–5.6% of acute conjunctivitis cases10). Coexisting genital infection has been reported in 54% of men and 74% of women10). It should be treated as a systemic infection that does not remain confined to the eye.
QIs bacterial conjunctivitis contagious?
A
Bacterial conjunctivitis spreads through contact transmission. Hand-to-eye contact and sharing towels or pillowcases are common routes of infection. Frequent handwashing and avoiding shared personal items are important for preventing further spread.
Toddlers to school-age children: Streptococcus pneumoniae is the most common. It occurs more frequently in winter, often presenting bilaterally alongside upper respiratory tract infections. Small outbreaks may occur.
Children overall: Haemophilus influenzae accounts for 29–42% and Streptococcus pneumoniae accounts for 13–30%1).
Adults
Staphylococcus aureus: A representative causative bacterium of conjunctivitis in adults. It presents as acute to subacute catarrhal conjunctivitis.
Blepharoconjunctivitis type: Often accompanied by inflammation of the eyelid margin, presenting as chronic blepharoconjunctivitis. May also involve superficial keratitis in the lower one-third of the cornea.
Elderly
Staphylococcus species: Most common. Frequently complicated by blepharitis.
Streptococcus pneumoniae and Haemophilus influenzae: Present as acute catarrhal conjunctivitis.
Corynebacterium species: In recent years, has become a concern as a cause of refractory chronic conjunctivitis.
Gonococcus (Neisseria gonorrhoeae): The cause of hyperacute conjunctivitis. It is the only bacterium that can infect healthy corneal epithelium and can cause corneal perforation. In adults, it presents as a sexually transmitted infection.
Chlamydia trachomatis: Causes chronic follicular conjunctivitis. Suspect this bacterium in prolonged follicular conjunctivitis that does not respond to antibiotics.
In recent years, with the widespread adoption of preventive measures against gonococcus and chlamydia in neonates, reports of neonatal conjunctivitis caused by Escherichia coli have been increasing4). Neonatal conjunctivitis caused by E. coli develops within 3 days after birth and presents with purulent discharge and eyelid edema4).
In recent years, drug-resistant bacteria such as methicillin-resistant Staphylococcus aureus (MRSA), penicillin-resistant Streptococcus pneumoniae (PRSP), and drug-resistant Haemophilus influenzae (BLNAR) have been increasing. Fluoroquinolone resistance is also progressing in Neisseria gonorrhoeae. When drug-resistant bacteria are involved, conjunctivitis can become refractory to treatment.
Poor hygiene habits: Insufficient hand washing, improper contact lens care
Crowded environments: Schools, daycare facilities, military barracks, etc.
Ocular surface abnormalities: Dry eye, blepharitis, anatomical abnormalities of the ocular surface
Immunodeficiency: Systemic immunosuppression
After ophthalmic surgery: Increased risk of postoperative infection
QWhy do causative bacteria differ by age?
A
This is because the normal conjunctival flora and immune function differ with age. Children have a lower ability to produce antibodies against the capsular antigen of Haemophilus influenzae, making them more susceptible to infection by this bacterium. In older adults, the defense mechanisms of the ocular surface decline, leading to an increase in infections caused by Staphylococcus species.
Most cases can be diagnosed based on clinical findings, and laboratory testing is not mandatory. Suspect bacterial conjunctivitis when bulbar conjunctival injection, mucopurulent discharge, and papillary reaction of the palpebral conjunctiva are present without marked follicular formation or preauricular lymphadenopathy.
Differentiating between bacterial and viral conjunctivitis is clinically important.
Smear test: Useful for rapid diagnosis. Observe bacteria phagocytized by neutrophils using Gram stain and Giemsa stain to estimate the causative organism. Simple staining kits (Diff-Quick, Faber G, etc.) are also available.
Isolation culture test: Identifies the causative bacteria and performs drug sensitivity testing. However, culture can detect the causative organism in only about half of cases.
Indications for culture: Culture is not performed in all cases. It is performed for neonates, treatment-resistant or recurrent cases, and when gonococcal infection is suspected.
Specimens When Gonococcal or Chlamydial Infection Is Suspected
When gonococcal infection is suspected, submit a conjunctival swab for culture. Since gonococci are susceptible to drying, specify the suspected organism when collecting the specimen. Culture is important not only for diagnosis but also for confirming drug sensitivity. Even if nucleic acid amplification testing is also performed, sensitivity cannot be evaluated8).
When chlamydial infection is suspected, a specimen containing not only eye discharge but also conjunctival epithelial cells is necessary. In cases of persistent follicular conjunctivitis, consider chlamydia antigen testing or nucleic acid amplification testing of conjunctival swabs. Evaluation of concurrent infections of the genital tract, pharynx, rectum, etc., is also important8).
The Infectious Keratitis Clinical Practice Guidelines (3rd Edition) strongly recommend combining smear microscopy and culture testing for the diagnosis of bacterial keratitis6). Culture positivity rates are reported to be 37.6–74.3%, and smear microscopy positivity rates are 58.1–73.7%6). In cases where no antibiotics have been administered before testing, the culture positivity rate is 77.3%; however, after administration, it drops to 37.8%. Therefore, specimens should be collected before antibiotic administration whenever possible6).
Viral conjunctivitis: characterized by follicular conjunctivitis, serous discharge, and preauricular lymphadenopathy. Adenovirus rapid testing is useful
Allergic conjunctivitis: primarily presents with ocular itching. Eosinophil infiltration is characteristic
Differentiation from gonococcal conjunctivitis: Since Moraxella species are also Gram-negative diplococci, differentiation from gonococci is difficult by smear alone. Always combine with culture testing
Non-infectious diseases: In cases of conjunctivitis that does not respond to antibiotics, vascular lesions such as carotid-cavernous fistula (CCF) should also be considered in the differential diagnosis5). If conjunctival injection, chemosis, ocular movement disorders, and elevated intraocular pressure are present and the condition does not respond to antibiotics, suspect carotid-cavernous fistula and perform imaging studies5)
The mainstay of treatment for bacterial conjunctivitis is topical administration of antibiotics. Initial therapy is given empirically, and the regimen should be adjusted based on smear and culture results.
Approximately 60% of cases resolve spontaneously, but antibiotic administration can shorten the duration of illness. The antibiotic-treated group heals approximately 1.9 days faster than the untreated group (3.8 days vs 5.7 days)2). Artificial tears (carboxymethylcellulose sodium) alone have also been reported to reduce local pathogen load and promote healing2).
Among fluoroquinolone antibiotics, tosufloxacin (Ozex, Tosuflo) is approved for use in children. In adults, choose a fluoroquinolone or cephem antibiotic, keeping Staphylococcus species in mind.
Staphylococcus, Streptococcus, Streptococcus pneumoniae: Beta-lactams (Bestron) are first-line. Fluoroquinolones are also effective.
PRSP: May show resistance to aminoglycosides. Choose a cephem (Bestron) or fourth-generation fluoroquinolone (Gatiflo, Vegamox).
Aminoglycosides: Ineffective against Streptococcus and Streptococcus pneumoniae.
Gram-Negative Bacteria
Haemophilus influenzae: Penicillins and cephalosporins are first-line. Fluoroquinolones may also be used. In recent years, β-lactam-resistant strains (BLNAR) have emerged.
Neisseria gonorrhoeae: Fluoroquinolone resistance is progressing, and cephalosporins are first-line. For multidrug-resistant gonococci, intravenous ceftriaxone (Rocephin) is also used.
MRSA: Chloramphenicol eye drops (Ophthalon) are attempted first. Staphylococci are less likely to develop resistance to chloramphenicol. If the effect is insufficient, vancomycin ophthalmic ointment is used (requires case registration). Self-prepared arbekacin eye drops are also reported to be useful.
Gonococcal conjunctivitis: Systemic administration of ceftriaxone is required in addition to topical antibiotic eye drops. Because of the risk of corneal perforation, follow-up every 1–2 days is necessary.
Azithromycin (Azimicin) eye drops: Launched in 2019. They serve as a countermeasure against fluoroquinolone-resistant bacteria. For conjunctivitis, use 2 times daily for 2 days, then once daily for 5 days.
Key Points in the Treatment of Sexually Transmitted Infection-Related Conjunctivitis
Topical antibiotics alone are insufficient for gonococcal conjunctivitis; systemic treatment is essential. For adults and adolescents, a single intramuscular dose of ceftriaxone 1 g is a treatment option8). A single saline irrigation of the eye may also be considered8). Cases with corneal epithelial defects or corneal thinning require hospitalization and frequent examinations11).
For chlamydial conjunctivitis, evaluation of systemic infection is necessary in addition to topical eye treatment. Doxycycline 100 mg twice daily for 7 days is the standard oral regimen8). A single oral dose of azithromycin 1 g is an alternative, but the decision should consider coinfected sites and the possibility of pregnancy8).
Partner management is important for both gonococcal and chlamydial infections. Treating only the patient may lead to reinfection. Concurrent testing for HIV, syphilis, and other sexually transmitted infections should also be considered8).
QCan it heal without antibiotics?
A
About 60% of acute bacterial conjunctivitis resolves spontaneously. However, antibiotic treatment shortens the duration of illness by approximately 2 days and promotes microbial elimination2), so it is generally prescribed at the time of consultation. Contact lens users are at risk of severe disease, and aggressive treatment is recommended.
The normal conjunctiva harbors normal flora such as Staphylococcus and Corynebacterium. Staphylococcus aureus is isolated from 5–10% of healthy conjunctival sacs. Tear washing, the barrier function of the conjunctival epithelium, and immune factors in tears such as lysozyme and IgA normally prevent infection. Infection occurs when these defense mechanisms are compromised.
Staphylococcus aureus: Causes direct tissue damage through exotoxins and also triggers allergic reactions via sensitization. It is also a causative organism of marginal corneal ulcers and corneal phlyctenules.
Coagulase-negative staphylococci (CNS): Some strains produce biofilms and exhibit resistance to antimicrobial agents.
Streptococcus pneumoniae: Possesses a capsule and shows resistance to aminoglycosides. It is classified into more than 80 serotypes based on capsular soluble substances, with type III being the most virulent.
Haemophilus influenzae: A commensal bacterium of the upper respiratory tract. Children are susceptible to infection due to their low ability to produce antibodies against the capsular antigen of this bacterium. It preferentially infects squamous epithelium, causing intense bulbar conjunctival hyperemia, known as pink eye.
Neisseria gonorrhoeae: Adheres to mucosal epithelial cells via pili and outer membrane proteins, and can invade healthy corneal epithelium. It is fragile and loses infectivity within hours once detached from the mucosa.
Bacterial conjunctivitis triggers a neutrophil-predominant inflammatory response. The predominance of neutrophilic infiltration in conjunctival smear specimens is a key differentiating feature from viral conjunctivitis, where lymphocytic infiltration predominates. Observing bacteria phagocytosed by neutrophils can help identify the causative organism.
Howard & de St. Maurice reviewed a study showing that the introduction of PCV13 (13-valent pneumococcal conjugate vaccine) led to a 93% reduction in conjunctivitis caused by PCV13 serotypes and a reduction of more than one-third in total conjunctivitis cases1). Notably, the incidence of conjunctivitis caused by nontypeable Haemophilus influenzae (NTHi) also significantly decreased after PCV13 introduction1). This finding suggests the presence of complex bacterial interactions between Streptococcus pneumoniae and Haemophilus influenzae in the respiratory tract.
Therapeutic Effects of Antibiotics and Artificial Tears
Liu & Kuo describe a randomized controlled trial comparing three groups for pediatric acute infectious conjunctivitis: moxifloxacin, artificial tears (carboxymethylcellulose sodium), and no treatment2). The moxifloxacin group showed a reduction of 1.9 days to cure compared with the no-treatment group (3.8 days vs 5.7 days). Additionally, the artificial tears (placebo) group also significantly shortened the duration of healing compared with the no-treatment group2). A meta-analysis confirmed that antibiotics reduce symptoms on days 3–6 (odds ratio 0.59)2).
Commiskey et al. reported a case of bilateral chronic refractory conjunctivitis in a 98-year-old woman3). Age-related atrophy of the orbital tissues and dehiscence of the levator aponeurosis led to enlargement of the superior fornix, forming a reservoir of infection. Staphylococcus aureus was the most common causative organism, and the mainstays of treatment are fornix irrigation, topical and systemic antibiotics, and povidone-iodine irrigation3). GFS should be considered in the differential diagnosis of refractory chronic conjunctivitis in elderly patients.
Changes in the Pathogens of Neonatal Conjunctivitis
Saadeh-Jackson et al. reported a case of neonatal conjunctivitis caused by Escherichia coli, arguing that as preventive measures against gonococcal and chlamydial infections become widespread, E. coli is emerging as a notable pathogen4). Clinical features included onset within 3 days of birth, normal body temperature, purulent discharge, and eyelid edema4). Levofloxacin eye drops based on culture results were effective.
QCan vaccines prevent bacterial conjunctivitis?
A
Reports indicate that the introduction of the pneumococcal conjugate vaccine (PCV13) has led to a 93% reduction in conjunctivitis caused by vaccine serotypes1). However, there is no vaccine that directly prevents all bacterial conjunctivitis. Regular handwashing and hygiene management remain the most important preventive measures.
Howard LM, de St Maurice A. Unraveling the Impact of Pneumococcal Conjugate Vaccines on Bacterial Conjunctivitis in Children. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2021;72(7):1208-1210. doi:10.1093/cid/ciaa202. PMID:32140700; PMCID:PMC11004944.
Liu SH, Kuo IC. Topical antibiotics and artificial tears associated with reduced infective-conjunctivitis symptoms. The Journal of pediatrics. 2023;261:113320. doi:10.1016/j.jpeds.2022.12.021. PMID:37741681; PMCID:PMC11249201.
Commiskey P, Bowers E, Dmitriev A, Mammen A. Bilateral, chronic, bacterial conjunctivitis in giant fornix syndrome. BMJ case reports. 2022;15(1). doi:10.1136/bcr-2021-245460. PMID:35027379; PMCID:PMC8762122.
Saadeh-Jackson S, Rodriguez L, Leffler CT, Freymiller C, Wolf E, Wijesooriya N, et al. Ophthalmia neonatorum due to Escherichia coli: A rare cause or an emerging bacterial etiology of neonatal conjunctivitis?. Clinical case reports. 2022;10(8):e6201. doi:10.1002/ccr3.6201. PMID:35949413; PMCID:PMC9354094.
Campos AL, Gonçalves FMF, Cardoso R, et al. A Rare and Surprising Case of Spontaneous Type B Carotid-Cavernous Fistula in an Internal Medicine Ward. Cureus. 2022;14(11):e31456. doi:10.7759/cureus.31456.
McAnena L, Knowles SJ, Curry A, Cassidy L. Prevalence of gonococcal conjunctivitis in adults and neonates. Eye (Lond). 2015;29(7):875-880. doi:10.1038/eye.2015.57. PMID:25907207; PMCID:PMC4506339.
Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187.
Abedifar Z, Fallah F, Asadiamoli F, Bourrie B, Doustdar F. Chlamydia trachomatis Serovar Distribution in Patients with Follicular Conjunctivitis in Iran. Turkish journal of ophthalmology. 2023;53(4):218-221. doi:10.4274/tjo.galenos.2022.12080. PMID:37602552; PMCID:PMC10442745.
Azari AA, Arabi A.. Conjunctivitis: A Systematic Review. J Ophthalmic Vis Res. 2020;15(3):372-395. doi:10.18502/jovr.v15i3.7456. PMID:32864068; PMCID:PMC7431717.
Albear S, LoBue S, Cooley A, Brandenburg T, Friedes R, Park J. Povidone-Iodine as an Adjuvant Therapy for Refractory Gonorrhea Keratoconjunctivitis: A Case Report. Cureus. 2025;17(5):e83676. doi:10.7759/cureus.83676.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.