Seasonal/perennial AC

Allergic Conjunctivitis (Including Hay Fever)
Key points at a glance
Section titled “Key points at a glance”1. What is allergic conjunctivitis?
Section titled “1. What is allergic conjunctivitis?”Allergic conjunctival disease (ACD) is defined as “an inflammatory disease of the conjunctiva primarily involving a type I allergic reaction, accompanied by subjective symptoms and objective findings triggered by an antigen”1). A diagnosis of ACD is not made based solely on an allergic predisposition; it requires the presence of subjective symptoms such as itching, foreign body sensation, discharge, and tearing, along with inflammatory changes of the conjunctiva.
The Japanese Society of Ophthalmic Allergy’s “Allergic Conjunctival Disease Clinical Practice Guidelines, 3rd Edition” classifies disease types based on the presence or absence of proliferative changes of the conjunctiva (papillary hypertrophy, giant papillae, limbal swelling or gelatinous elevation), the presence of atopic dermatitis, and the presence of mechanical irritation from foreign bodies1).
- Allergic conjunctivitis (AC): A type without proliferative changes of the conjunctiva. When symptoms occur seasonally, it is called seasonal allergic conjunctivitis (SAC); when perennial, it is called perennial allergic conjunctivitis (PAC). Among SAC, cases caused by pollen are also called “pollen conjunctivitis,” with major regional pollens such as Japanese cedar pollen being representative antigens1).
- Atopic keratoconjunctivitis (AKC): Chronic ACD associated with facial atopic dermatitis. Often accompanied by conjunctival fibrosis and corneal neovascularization or opacity1). First reported by Hogan et al. in 1952, describing five cases of atopic eczema with bilateral keratoconjunctivitis2).
- Vernal keratoconjunctivitis (VKC): A severe type with proliferative changes in the conjunctiva. May involve various corneal lesions such as corneal epithelial damage, persistent epithelial defects, shield ulcers, and corneal plaques1).
- Giant papillary conjunctivitis (GPC): Caused by mechanical irritation from contact lenses, ocular prostheses, or surgical sutures, with proliferative changes in the upper tarsal conjunctiva. Corresponds to the most severe form of contact lens-related papillary conjunctivitis, with papillae 1 mm or larger in diameter1).
Epidemiology in Japan
Section titled “Epidemiology in Japan”Nationwide surveys led by ophthalmologists include the Japan Ophthalmologists Association Allergic Eye Disease Survey (1993–1995), the Ministry of Health and Welfare Field Survey (1993), and the Japan Ocular Allergy Research Society Prevalence Survey (2017)1, 4). The 2017 prevalence survey reported the following data on prevalence, distribution by type, and age distribution.
| Indicator | Survey results |
|---|---|
| Overall prevalence of ACD | 48.7% (marked increase from 15–20% in 1993) |
| SAC due to Japanese cedar and cypress | 37.4% |
| Perennial allergic conjunctivitis (PAC) | 14.0% |
| SAC due to allergens other than Japanese cedar and cypress | 8.0% |
| Atopic keratoconjunctivitis (AKC) | 5.3% |
| Vernal keratoconjunctivitis (VKC) | 1.2% |
| Giant papillary conjunctivitis (GPC) | 0.6% |
| Age distribution of all ACD | Peak in 40s, small peak in teens |
| SAC regional variation | Higher in Tokyo metropolitan area and Chubu region |
Source: Japanese Ophthalmological Allergy Society Clinical Guideline Committee “Clinical Guidelines for Allergic Conjunctival Diseases, 3rd Edition” 1) and Okamoto et al. “2017 Japanese Ophthalmological Allergy Society Survey on Allergic Conjunctival Diseases” 4).
PAC has a bimodal peak in the teens and 40s, while SAC prevalence increases with age from childhood. SAC is associated with allergic rhinitis in 65-70% of cases 1). AKC is estimated to occur in 25-40% of patients with atopic dermatitis 5).
Q
How do the four types of allergic conjunctival disease differ?
A
According to the 3rd edition of the Japanese Ophthalmological Allergy Society clinical guidelines, the four types are classified based on the presence or absence of conjunctival proliferative changes, association with atopic dermatitis, and presence of mechanical irritation. Cases without proliferative changes are allergic conjunctivitis (subdivided into seasonal SAC and perennial PAC), those with facial atopic dermatitis are atopic keratoconjunctivitis (AKC), those with proliferative changes and severe corneal lesions are vernal keratoconjunctivitis (VKC), and those caused by mechanical irritation from contact lenses or artificial eyes are giant papillary conjunctivitis (GPC).
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”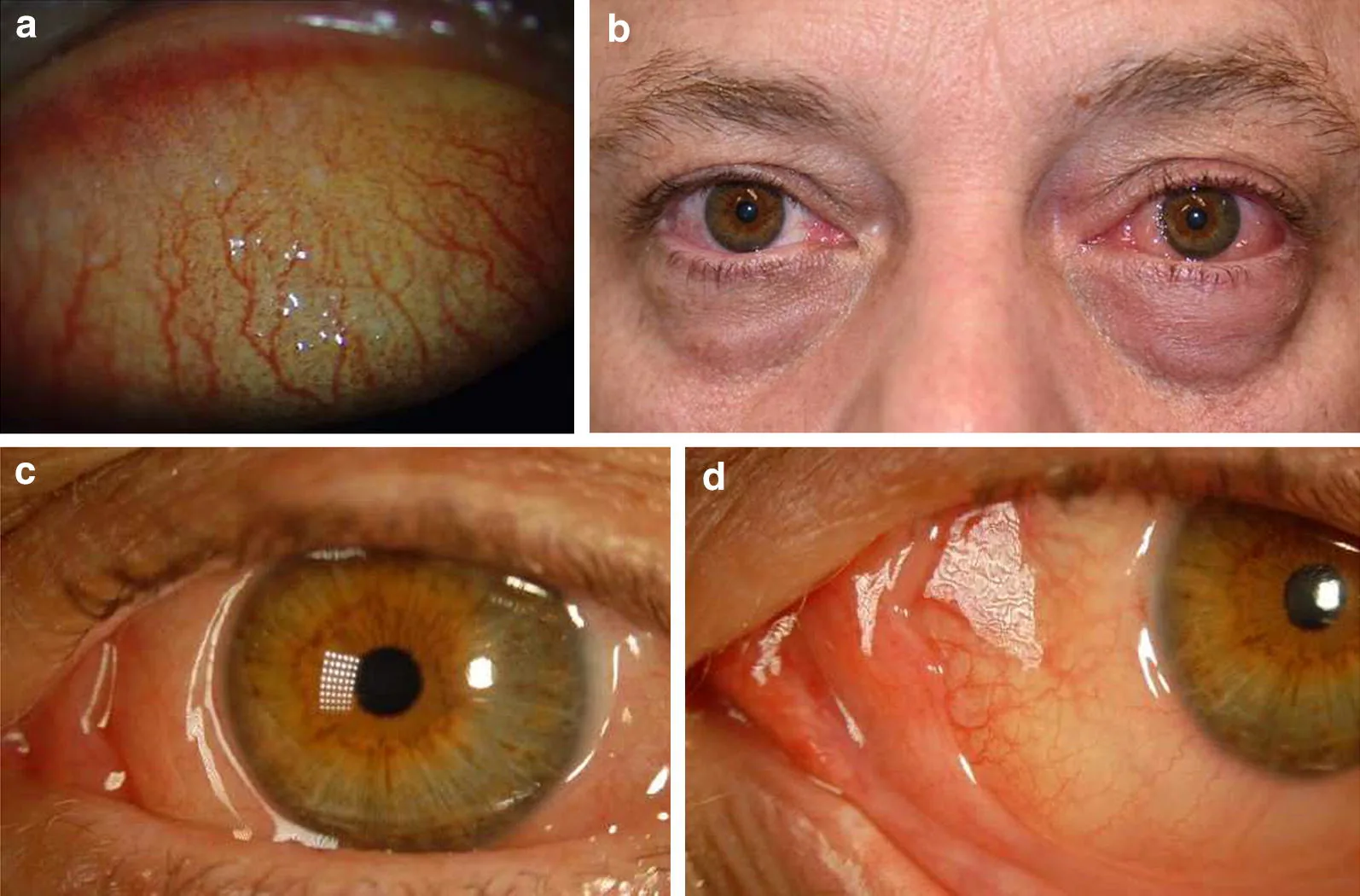
Dupuis P, et al. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020. Figure 3. PMCID: PMC6975089. License: CC BY.
Clinical photograph of allergic conjunctivitis showing conjunctival hyperemia, conjunctival edema, and eyelid edema. Inflammatory findings of the ocular surface and eyelids are directly observable, corresponding to the description of main symptoms and clinical findings.
Subjective Symptoms
Section titled “Subjective Symptoms”The typical subjective symptoms of ACD are itching, foreign body sensation, and discharge, among which ocular itching is the most specific symptom1).
- Ocular itching: The most characteristic symptom of ACD. It occurs when histamine released from mast cells stimulates sensory nerve endings. In children and the elderly, it may not be reported as itching but rather as foreign body sensation or discomfort1).
- Foreign body sensation: A complaint of “grittiness.” It often occurs when numerous conjunctival papillae come into contact with the cornea during blinking1).
- Discharge: Mainly serous or mucous, characterized by white or translucent stringy, viscous discharge. Its nature differs from neutrophil-dominant bacterial discharge1). In VKC, yellow viscous discharge may be observed.
- Tearing and hyperemia: Frequent but low specificity.
- Eye pain, photophobia, and decreased vision: Seen when corneal lesions are present, correlating with severity1).
- GPC-specific complaints: Often begin with mild foreign body sensation during contact lens use, followed by lens displacement, lens soiling, increased discharge, and blurred vision in that order.
Clinical Findings and Evaluation Criteria
Section titled “Clinical Findings and Evaluation Criteria”Severity assessment involves separate observation of the palpebral conjunctiva, bulbar conjunctiva, limbus, and cornea1). Representative items are shown below.
| Site | Item | Severity Indicator |
|---|---|---|
| Palpebral conjunctiva | Hyperemia | Mild: a few vessels; moderate: many vessels; severe: vessels indistinguishable |
| Palpebral conjunctiva | Papillae | Mild: 0.1–0.2 mm; moderate: 0.3–0.5 mm; severe: ≥0.6 mm |
| Palpebral conjunctiva | Giant papillae | Diameter ≥1 mm. Moderate if covering less than half of the upper palpebral conjunctiva; severe if half or more |
| Bulbar conjunctiva | Edema | Partial = mild; diffuse = moderate; vesicular = severe |
| Limbus | Trantas dots | 1–4 = mild; 5–8 = moderate; ≥9 = severe |
| Cornea | Epithelial damage | Punctate keratitis → desquamative punctate keratitis → shield ulcer |
Source: Created based on the severity assessment of the Japanese Society of Ocular Allergology’s “Guidelines for the Diagnosis and Treatment of Allergic Conjunctival Diseases, 3rd Edition” 1).
Characteristic findings by disease type
Section titled “Characteristic findings by disease type”Vernal keratoconjunctivitis, palpebral type
Cobblestone giant papillae: Hard cobblestone-like papillae lined up on the upper tarsal conjunctiva 1).
Mucoid discharge: Accompanied by a large amount of stringy, mucoid discharge.
Corneal complications: Punctate keratitis, desquamative punctate keratitis, shield ulcer, and corneal plaque may occur 1, 14).
Vernal keratoconjunctivitis, limbal type
Limbal gelatinous elevations: Gelatinous elevations form at the corneal limbus.
Trantas dots: Small white elevations caused by aggregates of degenerated conjunctival epithelium and eosinophils1).
Pseudo-arcus senilis: Arcus senilis-like opacity remaining after severe limbal inflammation1).
Atopic keratoconjunctivitis
Eczematous blepharitis: Continuous with facial atopic dermatitis. Accompanied by eyelid thickening, trichiasis, and madarosis.
Conjunctival pigmentation and symblepharon: Long-term course leads to conjunctival sac shortening and symblepharon1, 12).
Corneal complications: May progress from punctate keratitis to persistent epithelial defects and corneal ulcers.
Giant papillary conjunctivitis
Characteristic papillae: Round, well-defined, smooth surface, non-fused, and low elevation. Morphologically different from the giant papillae of vernal keratoconjunctivitis1).
Corneal complications are rare: Mainly caused by mechanical irritation, inflammation is often mild.
Low IgE positivity rate: The involvement of type I allergy is not always clear1).
3. Causes and risk factors
Section titled “3. Causes and risk factors”Causative antigens
Section titled “Causative antigens”The distribution of causative antigens varies greatly by disease type. Serum antigen-specific IgE antibody testing uses the “PAC set” (including mites, house dust, alder, cedar, cypress, timothy grass, orchard grass, mugwort, ragweed, Candida, Alternaria, cat epithelium, dog epithelium, etc.) as a covered item under insurance1).
| Disease type | Main causative antigens | Seasonality |
|---|---|---|
| Seasonal Allergic Conjunctivitis (SAC) | Japanese cedar/cypress (spring), grasses such as orchard grass/timothy (early summer), ragweed/mugwort (autumn) | Yes |
| Perennial Allergic Conjunctivitis (PAC) | Dust mites/house dust, mold, pet dander | No |
| Atopic Keratoconjunctivitis (AKC) | Multiple sensitizations (dust mites/house dust, pollen, food, etc.), atopic predisposition | Chronic |
| Vernal Keratoconjunctivitis (VKC) | House dust/dust mites are common, but also reacts to multiple antigens such as pollen and animal dander | Exacerbations present |
| Giant Papillary Conjunctivitis (GPC) | Contact lens materials/lens deposits, ocular prosthesis, exposed sutures | No |
Risk Factors and Background
Section titled “Risk Factors and Background”- Atopic predisposition/family history: A family history of bronchial asthma, allergic rhinitis, or atopic dermatitis increases the risk. In AKC, skin barrier dysfunction, including filaggrin gene abnormalities, is involved5).
- Urban living/environmental factors: Air pollution, smoking, and dry environments can exacerbate ACD6).
- Dupilumab: Dupilumab, an IL-4 receptor alpha chain antibody used to treat severe atopic dermatitis, has been reported to have a risk ratio of 2.64 for developing conjunctivitis, requiring caution during AKC treatment1).
- Eye rubbing habit: Chronic eye rubbing due to itching is a risk factor for keratoconus and atopic cataract5, 12). In AKC, chronic mechanical stimulation promotes weakening of corneal structure and has been linked to early-onset keratoconus5).
Q
What measures can be taken at home during pollen season?
A
For pollen measures, wearing goggles or regular glasses, discontinuing contact lenses and switching to glasses if possible, rinsing with preservative-free artificial tears (tap water is not allowed as it damages the cornea), wearing a smooth-textured coat when going out and removing it at the entrance, and washing the face and gargling after returning home are useful. Additionally, starting anti-allergic eye drops about two weeks before the predicted pollen dispersal date (“initial therapy”) is effective.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Diagnostic Approach
Section titled “Diagnostic Approach”Diagnosis is performed in three stages based on three elements: clinical symptoms, type I allergic predisposition, and local type I allergic reaction in the eye 1).
- Clinical diagnosis (A only): Presence of clinical symptoms characteristic of ACD.
- Clinical definitive diagnosis (A+B): In addition to clinical symptoms, positive total IgE antibodies in tears, positive serum antigen-specific IgE antibodies, or a positive skin reaction consistent with the suspected antigen.
- Definitive diagnosis (A+B+C, or A+C): In addition to the above, eosinophils in conjunctival scrapings are positive.
A: Presence of clinical symptoms / B: Presence of type I allergic predisposition / C: Presence of type I allergic reaction in the conjunctiva.
Among subjective symptoms and objective findings, severe ocular itching, giant papillae, limbal proliferation, and shield ulcers are considered particularly specific findings 1).
Local Ocular Examination
Section titled “Local Ocular Examination”- Eosinophil test in conjunctival scrapings: After topical anesthesia, evert the upper eyelid, gently massage the tarsal conjunctiva with a glass rod, collect mucus with a spatula, and smear it on a slide. Perform Hansel or Giemsa staining, and if even one eosinophil is observed under a light microscope, it is considered positive 1, 3).
- Total IgE antibody test in tears (Allerwatch®): A rapid diagnostic kit by Wakamoto Pharmaceutical / Minaris Medical, using immunochromatography to test tear samples. Reported sensitivity for ACD is 73.6%, specificity 100% 1). Positive rates by disease type: SAC 61.9%, PAC 65.4%, AKC 80.5%, VKC 94.7%, GPC 75.0%, overall 72.2% 3).
- Topical provocation test: A method to confirm induction of conjunctivitis symptoms by instilling a known antigen solution, but it is not covered by insurance in Japan and is not standardized 1).
Systemic Allergic Predisposition Testing
Section titled “Systemic Allergic Predisposition Testing”- Serum antigen-specific IgE antibody test: Select items mainly from the PAC set, such as mites, house dust, Japanese cedar, cypress, orchard grass, ragweed, mugwort, dog and cat epithelium. Up to 13 items are covered by insurance 1, 3). For screening, View Allergy 39 (Thermo Fisher Diagnostics) or Masto Immunosystems V (Minaris Medical), which allow simultaneous measurement of multiple items, can also be used under insurance coverage 3).
- Skin reaction (prick test/scratch test): Positive if wheal diameter is 3 mm or more, or at least half the size of the positive control wheal. Use positive control (to check for false negatives) and negative control (to check for dermographism). Histamine H₁ receptor antagonists and tricyclic antidepressants may cause false negatives, so attention to the washout period before testing is necessary 3). Exercise caution in patients with severe bronchial asthma, history of anaphylaxis, or significant cardiovascular disease.
Diagnostic Flow
Section titled “Diagnostic Flow”In clinical diagnosis, cases presenting with ocular itching and hyperemia are first stratified based on the presence or absence of conjunctival proliferative changes. If no proliferative changes are present, SAC/PAC is determined based on seasonality; if proliferative changes are present, GPC, AKC, and VKC are differentiated based on contact lens use and the presence or absence of atopic dermatitis1).
Differential Diagnosis
Section titled “Differential Diagnosis”In differential diagnosis, the following diseases should be particularly considered1).
- Viral conjunctivitis: Adenovirus (epidemic keratoconjunctivitis, pharyngoconjunctival fever), herpes simplex virus, varicella-zoster virus, enterovirus, SARS-CoV-2, etc. Acute onset, unilateral involvement, and preauricular lymphadenopathy are suggestive; adenovirus antigen can be detected using a rapid diagnostic kit.
- Bacterial conjunctivitis: Causative organisms include Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae. It is differentiated by mucopurulent yellow to yellow-green discharge and polymorphonuclear leukocytes in conjunctival scrapings.
- Chlamydial conjunctivitis: In adults, it presents as acute unilateral follicular conjunctivitis, characterized by large follicles in the lower palpebral conjunctival fornix.
- Conjunctival folliculosis: Miliary follicles seen in the lower palpebral conjunctival fornix of children, asymptomatic and of no pathological significance.
- Dry eye: Accompanied by shortened tear break-up time (BUT) and often coexists with allergic conjunctival disease (ACD)1).
Q
How can viral conjunctivitis and allergic conjunctivitis be distinguished?
A
If ocular itching is severe, both eyes are affected, discharge is predominantly serous or mucoid white, and there is an allergic predisposition (concomitant allergic rhinitis or dermatitis, family history), allergic conjunctivitis is suspected. Conversely, if onset is acute, starting in one eye, with mucopurulent or yellow discharge, preauricular lymphadenopathy, fever, or sore throat, infectious conjunctivitis is considered, and adenovirus rapid testing or conjunctival scraping examination is performed. The diagnostic criteria for both are detailed in the third edition of the Japanese Society of Ocular Allergology guidelines.
5. Standard Treatment
Section titled “5. Standard Treatment”The first-line treatment for all disease types is anti-allergic eye drops, with steroid eye drops and immunosuppressive eye drops added depending on severity1). For refractory severe cases, oral steroids, subconjunctival steroid injections, and surgical treatments such as conjunctival papillae resection are also options.
Anti-Allergic Eye Drops
Section titled “Anti-Allergic Eye Drops”Anti-allergic eye drops are broadly classified into two categories based on their mechanism of action1, 13).
- Mediator release inhibitors: They inhibit mast cell degranulation, suppressing the release of histamine, leukotrienes, thromboxane A₂, etc., thereby reducing the immediate phase reaction of type I allergy. By inhibiting local conjunctival infiltration of inflammatory cells, they also act on the late phase.
- Histamine H₁ receptor antagonists: These competitively inhibit the binding of histamine released from mast cells to H₁ receptors, suppressing redness and eye itching. They are reported to have a faster onset of action for itching than mediator release inhibitors.
Representative drugs are summarized in the table below.
| Classification | Generic name | Representative brand name | Concentration and dosage |
|---|---|---|---|
| Mediator release inhibitors | Pemirolast potassium | Alegysal ophthalmic solution | 0.1% twice daily |
| Mediator release inhibitors | Tranilast | Rizaben ophthalmic solution | 0.5% four times daily |
| Mediator release inhibitors | Ibudilast | Ketas ophthalmic solution | 0.01% four times daily |
| Mediator release inhibitors | Acitazanolast hydrate | Zepelin ophthalmic solution | 0.1% 4 times daily |
| H₁ receptor antagonists | Ketotifen fumarate | Zaditen ophthalmic solution | 0.05% 4 times daily |
| H₁ receptor antagonists | Levocabastine hydrochloride | Livostin ophthalmic solution | 0.025% 4 times daily |
| H₁ receptor antagonists | Olopatadine hydrochloride | Patanol ophthalmic solution | 0.1% 4 times daily |
| H₁ receptor antagonist | Epinastine hydrochloride | Alesion ophthalmic solution / Alesion LX ophthalmic solution | 0.05% 4 times daily / 0.1% 2 times daily |
Source: Created based on the list of anti-allergic eye drops from the Japanese Society of Ophthalmic Allergy’s “Clinical Practice Guidelines for Allergic Conjunctival Diseases, 3rd Edition” 1).
Ketotifen, olopatadine, and epinastine have been shown to have histamine H₁ receptor antagonistic effects as well as mediator release inhibitory effects in vitro. Alesion LX does not contain preservatives, making it easier to prescribe for contact lens wearers.
Initial therapy (seasonal allergic conjunctivitis)
Section titled “Initial therapy (seasonal allergic conjunctivitis)”For seasonal allergic conjunctivitis, initial therapy with anti-allergic eye drops is recommended starting approximately 2 weeks before the predicted pollen dispersal date, or as soon as any symptoms appear 1). This reduces symptoms during the peak pollen season, and some reports indicate that it suppresses the onset of hay fever symptoms in about 30% of patients. For perennial allergic conjunctivitis, mediator release inhibitors are effective for maintaining mast cell membrane stabilization throughout the year.
Treatment strategy by disease type
Section titled “Treatment strategy by disease type”1) Seasonal and perennial allergic conjunctivitis (SAC / PAC)
Section titled “1) Seasonal and perennial allergic conjunctivitis (SAC / PAC)”- First-line: Anti-allergic eye drops (mediator release inhibitors or H₁ antagonists) 1).
- During periods of severe symptoms or when accompanied by nasal symptoms: Oral anti-allergic medications, and if necessary, concomitant use of NSAID eye drops 1).
- If symptoms cannot be controlled with anti-allergic eye drops: Steroid eye drops are used short-term in combination. The use of steroid eye drops for SAC/PAC is conditionally recommended 1); they should not be first-line treatment, and should be used only for a short period with regular intraocular pressure monitoring.
- For contact lens wearers or patients with dry eye, preservative-free formulations should be selected.
2) Atopic keratoconjunctivitis (AKC)
Section titled “2) Atopic keratoconjunctivitis (AKC)”- First-line treatment is anti-allergic eye drops. In cases with insufficient effect, steroid eye drops or immunosuppressive eye drops are used in combination 1).
- In AKC, steroid eye drops are used to suppress inflammation 1).
- Tacrolimus eye drops are also a useful option, but in Japan, insurance coverage is limited to vernal keratoconjunctivitis 1, 8). Cyclosporine eye drops are also a treatment option for AKC 1).
- Treatment of atopic blepharitis must be performed concurrently, and collaboration with dermatology and allergy departments is essential 5).
- When prescribing oral steroids, collaborate with internal medicine and dermatology specialists 1).
- In cases where systemic treatment with biologics including dupilumab or oral cyclosporine is performed, note the risk ratio of 2.64 for dupilumab-associated conjunctivitis 1).
3) Vernal keratoconjunctivitis (VKC)
Section titled “3) Vernal keratoconjunctivitis (VKC)”In vernal keratoconjunctivitis, treatment is intensified stepwise according to severity 1, 7).
- First, prescribe anti-allergic eye drops as a foundation.
- For moderate to severe cases, add immunosuppressive eye drops. Tacrolimus eye drops have relatively strong evidence of efficacy, and cyclosporine eye drops are also conditionally recommended 1, 8, 9).
- In severe cases that do not improve with two agents, add steroid eye drops 1).
- Cyclosporine plus steroid combination for proliferative changes, and tacrolimus plus steroid combination for severe cases are both considered conditionally 1).
- For the most severe cases not controlled with eye drops, consider oral steroids, subconjunctival steroid injection, conjunctival papillae resection, and corneal plaque scraping 1). For subconjunctival injection, use triamcinolone acetonide or betamethasone sodium phosphate suspension, but be cautious of intraocular pressure elevation, and avoid repeated use or use in children under 10 years old 1).
- After symptom improvement, switch steroid eye drops to a lower potency, then taper and discontinue, and control with two agents: anti-allergic eye drops and immunosuppressive eye drops.
Proactive therapy: If the remission period is long, gradually reduce the immunosuppressive eye drops from twice daily to once daily to twice weekly, and finally continue with a small maintenance dose. Adjust the dose based on symptoms to prevent recurrence 1).
4) Giant Papillary Conjunctivitis (GPC)
Section titled “4) Giant Papillary Conjunctivitis (GPC)”- Removal of the cause is most important. If contact lenses are the cause, discontinue use in principle. When resuming use, consider switching to daily disposable soft contact lenses, changing lens material or shape, and providing instruction on rubbing cleaning and changing care products 1).
- First-line treatment is anti-allergic eye drops (mainly mediator release inhibitors). In severe cases, short-term use of steroid eye drops (e.g., 0.1% fluorometholone 4 times daily) is added. Monitor intraocular pressure during use.
- If an ocular prosthesis is the cause, consider replacing or changing the type of prosthesis 1).
Immunosuppressive Eye Drops (Insurance-covered for VKC)
Section titled “Immunosuppressive Eye Drops (Insurance-covered for VKC)”Cyclosporine Eye Drops
Brand name: Papilock Mini Ophthalmic Solution 0.1% 1)
Dosage: 3 times daily
Characteristics: An immunosuppressant that inhibits the calcineurin pathway in T cells. When used in combination with anti-allergic and steroid eye drops, it allows gradual tapering of steroids 1, 9). Effective for limbal VKC. Onset of effect is somewhat delayed.
Clinical positioning: Conditionally recommended for VKC; for conjunctival proliferative changes, combination with steroid eye drops may be considered 1).
Tacrolimus Eye Drops
Brand name: Talymus Ophthalmic Solution 0.1% 1)
Dosage: 2 times daily
Characteristics: Has a stronger immunosuppressive effect than cyclosporine and is effective as monotherapy even in severe steroid-resistant cases 1, 8). Also useful in cases complicated by atopic dermatitis.
Clinical positioning: An important treatment option for VKC and AKC, but AKC is not covered by insurance. For severe conjunctival proliferative changes, combination with steroid eye drops may be considered 1).
Both agents may cause stinging or a burning sensation upon instillation, and during use, attention should be paid to the development of infections including herpetic keratitis. They are indicated for VKC in both children and adults1).
Other Precautions
Section titled “Other Precautions”Surgical Treatment for AKC Complications
Section titled “Surgical Treatment for AKC Complications”Complications arising during the course of AKC may require surgical treatment5).
- Amniotic membrane transplantation: Performed for persistent corneal epithelial defects.
- Corneal transplantation: Performed for corneal opacity, severe ulceration, or thinning, but the rejection rate is high in AKC patients, and strict control of inflammation is necessary postoperatively.
- Cataract surgery: Performed for atopic cataract presenting with anterior and posterior subcapsular opacities.
- Eyelid surgery: Correction of trichiasis, ectropion, and entropion.
Q
Why are immunosuppressive eye drops necessary for vernal keratoconjunctivitis and atopic keratoconjunctivitis?
A
In vernal keratoconjunctivitis and atopic keratoconjunctivitis, in addition to type I allergic reactions, Th2 cells (type 2 helper T cells) are deeply involved in pathogenesis. In some cases, conventional anti-allergic eye drops alone cannot control T cells, and immunosuppressive eye drops such as cyclosporine and tacrolimus suppress T cell activation, improving eosinophil infiltration, proliferative changes, and corneal epithelial damage. Tacrolimus eye drops, in particular, are an important treatment option for severe cases.
Q
Is it safe to use steroid eye drops for a long time?
A
Steroid eye drops are basically used for short-term combination therapy in cases not controlled by anti-allergic eye drops and are not first-line treatment. They carry risks of increased intraocular pressure, cataract formation, and infection induction, especially in children where the frequency of increased intraocular pressure is high, so regular intraocular pressure measurement is necessary during use. In vernal keratoconjunctivitis, steroids can be tapered by combining with immunosuppressive eye drops, so long-term use of steroids alone is generally avoided.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”Immediate and Late Phases of Type I Allergy
Section titled “Immediate and Late Phases of Type I Allergy”The basic mechanism of allergic conjunctivitis is a type I (immediate) allergic reaction.
Immediate phase (within about 15 minutes after antigen exposure): When allergens reaching the conjunctiva cross-link with IgE antibodies on the surface of sensitized conjunctival mast cells, the mast cells degranulate, releasing chemical mediators such as histamine, tryptase, leukotrienes, and prostaglandins all at once 10, 11). Released histamine acts via H₁ receptors to cause capillary dilation, increased vascular permeability, sensory nerve stimulation, and increased mucus secretion, manifesting as ocular itching, conjunctival hyperemia, conjunctival edema, and tearing.
Late phase (several hours later): Cytokines (IL-4, IL-5, IL-13, etc.) and adhesion molecules (ICAM-1, VCAM-1, etc.) are expressed, leading to infiltration of eosinophils, neutrophils, lymphocytes, and basophils into the conjunctival tissue 10, 11). Tissue-damaging proteins released from eosinophils, such as major basic protein (MBP) and eosinophil cationic protein (ECP), damage the corneal and conjunctival epithelium, causing corneal lesions such as punctate keratitis, persistent corneal epithelial defects, and shield ulcers 14).
Th2 Cells and Special Pathophysiology of VKC and AKC
Section titled “Th2 Cells and Special Pathophysiology of VKC and AKC”While mild SAC/PAC primarily involve the immediate phase of type I allergy, in vernal keratoconjunctivitis and atopic keratoconjunctivitis, Th2 cells (type 2 helper T cells) play a central role in pathogenesis 1, 13). In animal models, strong conjunctival eosinophil infiltration is not induced by type I allergic reactions alone; it is only induced when Th2 cells are involved. Histopathology of giant papillae in vernal keratoconjunctivitis shows eosinophil infiltration, fibroblast proliferation, extracellular matrix deposition, and numerous T cell infiltrates. Tear eosinophil counts have been reported to correlate with the severity of corneal damage 13).
In the conjunctival tissue of AKC, in addition to type I hypersensitivity, type IV (delayed-type) hypersensitivity characterized by infiltration of T cells, macrophages, and dendritic cells is also involved. Histological features include goblet cell proliferation, eosinophil and mast cell infiltration into the epithelium, and mononuclear cell infiltration in the lamina propria. Decreased corneal sensitivity and reduced conjunctival goblet cell density have also been reported5, 14).
Pollen hatch-out mechanism
Section titled “Pollen hatch-out mechanism”Japanese cedar pollen has a large particle size and cannot directly pass through the conjunctival epithelium. However, when pollen absorbs moisture from tears and bursts (hatch-out), antigen proteins (Cry j 1, Cry j 2, etc.) are eluted, pass through the conjunctival epithelium, reach deep mast cells, and initiate an allergic reaction. This mechanism explains why diluting tears and washing away pollen with artificial tears is effective for prevention.
Mechanism of giant papillary conjunctivitis
Section titled “Mechanism of giant papillary conjunctivitis”The involvement of type I allergy in GPC is not always clear; it is thought to be primarily caused by repeated mechanical irritation from contact lenses, their deposits, or exposed sutures, as well as immune reactions to lens materials and deposited proteins1). Infiltration of eosinophils, mast cells, and basophils is observed in conjunctival tissue, but the rates of serum antigen-specific IgE antibody positivity and eosinophil positivity are lower than in other disease types1).
Mechanism of AKC complications
Section titled “Mechanism of AKC complications”The pathogenesis of ocular complications characteristic of AKC is summarized as follows5, 12).
- Keratoconus: Repeated mechanical damage to the cornea from chronic eye rubbing and weakening of corneal structure due to chronic inflammation are involved.
- Atopic cataract: Characterized by anterior subcapsular and posterior subcapsular opacities, it develops as lens opacification independent of steroid use.
- Herpes simplex keratitis: Patients with AKC have a high risk of bilateral herpetic keratitis, requiring special attention during immunosuppressive therapy.
- Retinal detachment: It is reported to be more frequent in patients with atopic dermatitis, and an association with eye scratching behavior has been suggested.
7. Latest research and future perspectives
Section titled “7. Latest research and future perspectives”Biologic agents
Section titled “Biologic agents”Omalizumab (anti-IgE monoclonal antibody) is a biologic used for bronchial asthma and chronic urticaria. Overseas case reports and small observational studies have reported its efficacy for refractory vernal keratoconjunctivitis and severe atopic keratoconjunctivitis. It is not covered by insurance for ophthalmic diseases in Japan and is currently considered an investigational option11).
JAK inhibitors (e.g., upadacitinib): By selectively inhibiting the JAK-STAT pathway, they suppress IL-4/IL-13 signaling and are being investigated for their potential to improve both skin and ocular symptoms while avoiding dupilumab-associated conjunctivitis.
Novel mechanism eye drops
Section titled “Novel mechanism eye drops”New molecules that simultaneously inhibit multiple targets, such as eye drops (rVA576) that block both complement C5 and leukotriene B4, are in development, with phase I clinical trials underway.
Primary prevention and lifestyle
Section titled “Primary prevention and lifestyle”Probiotics: Prenatal and postnatal probiotic intake has been reported to potentially reduce the incidence of atopic diseases by up to 30%, but conclusive evidence has not been established. It has also been suggested that antibiotic use may increase the risk of atopic diseases through changes in the gut microbiota.
Breastfeeding: Breastfeeding, especially before 3 months of age, has been suggested as a possible protective factor against atopic diseases. No evidence of benefit has been found for vitamin or mineral supplements.
Disclaimer
Section titled “Disclaimer”8. References
Section titled “8. References”- 日本眼科アレルギー学会診療ガイドライン作成委員会. アレルギー性結膜疾患診療ガイドライン(第3版). 日眼会誌. 2021;125(8):741-785. https://www.nichigan.or.jp/member/journal/guideline/detail.html?dispmid=909&itemid=429
- Hogan MJ. Atopic keratoconjunctivitis. Trans Am Ophthalmol Soc. 1952;50:265-281.
- 庄司純, ほか. アレルギー性結膜疾患診断における自覚症状、他覚所見および涙液総IgE検査キットの有用性の検討. 日眼会誌. 2012;116(6):485-493. CiNii: https://cir.nii.ac.jp/crid/1520290883483009152
- 岡本茂樹, ほか. 2017年度日本眼科アレルギー学会アレルギー性結膜疾患実態調査. 日眼会誌. 2022;126(7):625-635. http://journal.nichigan.or.jp/Disp?mag=0&number=7&start=625&style=abst&vol=126&year=2022
- Chen JJ, Applebaum DS, Sun GS, Pflugfelder SC. Atopic keratoconjunctivitis: A review. Journal of the American Academy of Dermatology. 2014;70(3):569-75. doi:10.1016/j.jaad.2013.10.036. PMID:24342754.
- Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Current opinion in allergy and clinical immunology. 2015;15(5):482-8. doi:10.1097/ACI.0000000000000204. PMID:26258920.
- 福島敦樹. 春季カタルのパターン治療のためのプロトコール. あたらしい眼科. 2013;30(4):491-496.
- Ohashi Y, Ebihara N, Fujishima H, et al. A randomized, placebo-controlled clinical trial of tacrolimus ophthalmic suspension 0.1% in severe allergic conjunctivitis. J Ocul Pharmacol Ther. 2010;26(2):165-174. doi:10.1089/jop.2009.0087.
- Takamura E, Uchio E, Ebihara N, Okamoto S, Kumagai N, Shoji J, Nakagawa Y, Namba K, Fukushima A, Fujishima H, Miyazaki D, Ohashi Y.. [A prospective, observational, all-prescribed-patients study of cyclosporine 0.1% ophthalmic solution in the treatment of vernal keratoconjunctivitis]. Nippon Ganka Gakkai Zasshi. 2011;115(6):508-515. PMID:21735754.
- Sánchez-García S, Habernau Mena A, Quirce S. Biomarkers in inflammatory allergic conjunctivitis: a systematic review for biomarkers. Clin Transl Allergy. 2019;9:27.
- Leonardi A, Bogacka E, Fauquert JL, Kowalski ML, Groblewska A, Jedrzejczak-Czechowicz M, et al. Ocular allergy: recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy. 2012;67(11):1327-37. doi:10.1111/all.12009. PMID:22947083.
- 内尾英一. 免疫抑制点眼薬の使用法. 日眼会誌. 2015;119(3):136-141.
- Kumar S. Vernal keratoconjunctivitis: a major review. Acta ophthalmologica. 2009;87(2):133-47. doi:10.1111/j.1755-3768.2008.01347.x. PMID:18786127.
- Wakamatsu TH, Satake Y, Igarashi A, Dogru M, Ibrahim OM, Okada N, et al. IgE and eosinophil cationic protein (ECP) as markers of severity in the diagnosis of atopic keratoconjunctivitis. The British journal of ophthalmology. 2012;96(4):581-6. doi:10.1136/bjophthalmol-2011-300143. PMID:22275342.