Vernal keratoconjunctivitis (VKC) is an allergic conjunctival disease primarily involving a type I allergic reaction, with proliferative changes in the conjunctiva (giant conjunctival papillae, limbal proliferation) 7). In the Japanese Guidelines for Allergic Conjunctival Disease, 3rd edition, allergic conjunctival disease (ACD) is defined as “an inflammatory disease of the conjunctiva primarily involving a type I allergic reaction, accompanied by subjective symptoms and objective findings triggered by antigens,” and VKC is classified as a severe type with conjunctival proliferative changes and corneal lesions 7).
The term “vernal” means spring, and it was named because it tends to worsen in spring. However, many cases actually have a perennial course, and the pathology involves not only type I allergy but also a type IV hypersensitivity reaction driven by CD4-positive type 2 helper T cells (Th2 cells).
Allergic conjunctival diseases are classified into the following four types 7).
Allergic conjunctivitis (AC): No proliferative changes in the conjunctiva. Subdivided into seasonal (SAC) and perennial (PAC).
Atopic keratoconjunctivitis (AKC): Chronic ACD accompanied by facial atopic dermatitis. Often involves conjunctival fibrosis and corneal neovascularization/opacification.
Vernal keratoconjunctivitis (VKC): Proliferative ACD. Some cases are complicated by atopic dermatitis. Presents various corneal lesions such as corneal epithelial disorders, corneal erosion, persistent corneal epithelial defect, shield ulcer, and corneal plaque.
According to a nationwide survey in Japan, the overall prevalence of allergic conjunctival diseases has reached 48.7%, a marked increase compared to the 1993 Ministry of Health and Welfare field survey (15–20%)7). The breakdown by disease type is as follows7).
The age distribution of VKC, according to a 2017 nationwide survey, shows the highest peak in the 20s, with another significant peak during school age, and it is more common in boys around 10 years old7). The age of onset ranges from 5 to 25 years, with a peak at 10–12 years. In most cases, symptoms naturally resolve around puberty, but in about 12% of patients, symptoms persist into adulthood. Although more common in boys, the gender difference narrows with age.
In Japan, symptoms tend to worsen during the hot and humid summer months and in spring when cedar and cypress pollen are dispersed. However, because house dust and mites are common causative antigens, many cases follow a perennial course. Furthermore, while an epidemiological survey by the Japanese Ophthalmological Society’s Allergic Eye Disease Research Group from 1993 to 1995 showed that allergic conjunctivitis as a whole peaked in the teens and decreased with age, the 2017 survey revealed a shift to a pattern with the highest peak in the 40s and a smaller peak in the teens7). This change is thought to reflect alterations in antigen exposure, improvements in diagnostic techniques, and demographic shifts.
VKC is classified into three types based on the location of clinical findings.
Palpebral type: Characterized by cobblestone-like giant papillae on the upper tarsal conjunctiva. This is the most common type. It often presents with punctate keratopathy, corneal ulcers, and mucous discharge.
Limbal type: Characterized by gelatinous limbal elevations and Horner-Trantas dots. Mild cases may be missed without fluorescein staining.
Mixed type: Features of both palpebral and limbal types.
Many patients have a personal or family history of atopy. NGS (next-generation sequencing) analysis of monozygotic twins and their father showed associations of HLA-DQB105:01, HLA-DRB101:01:01, and HLA-A*32:01:01 with VKC2). However, a clear correlation with a single causative genetic locus has not been established.
QWhat is the difference between VKC and atopic keratoconjunctivitis (AKC)?
A
VKC typically develops around age 10, features cobblestone giant papillae on the upper tarsal conjunctiva, and often resolves spontaneously after puberty. In contrast, AKC develops in the 20s to 50s, is associated with atopic dermatitis, follows a chronic course, and tends to cause conjunctival sac shortening, symblepharon, and corneal opacities. While VKC is often associated with sensitization to house dust and mites, AKC is characterized by a higher eosinophil positivity rate in conjunctival scrapings and markedly elevated serum IgE. However, VKC cases complicated by atopic dermatitis tend to be more severe, and differentiation between the two can sometimes be difficult.
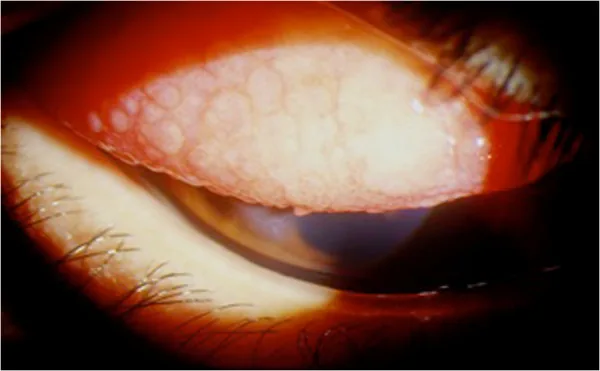
Mehta JS, et al. Diagnosis, Management, and Treatment of Vernal Keratoconjunctivitis in Asia: Recommendations From the Management of Vernal Keratoconjunctivitis in Asia Expert Working Group. Front Med (Lausanne). 2022;9:882240. Figure 2. PMCID: PMC9376221. License: CC BY.
This shows the palpebral conjunctival type, a clinical subtype of vernal keratoconjunctivitis, characterized by large cobblestone-like papillae on the upper palpebral conjunctiva. This corresponds to the cobblestone giant papillae discussed in the section “2. Main Symptoms and Clinical Findings.”
VKC is characterized by a stronger complaint of eye pain compared to other allergic conjunctival diseases. Patients often report eye pain rather than itching or foreign body sensation, and severe cases can lead to visual impairment 7).
Itching: This is the most diagnostically specific subjective symptom in allergic conjunctival diseases. Severe ocular itching is an important diagnostic clue for suspecting VKC 7).
Eye pain: Particularly severe in VKC, associated with corneal lesions.
Mucoid discharge: VKC may present with yellow, viscous discharge that is stringy in nature.
Photophobia and tearing: These intensify with the progression of corneal complications.
Foreign body sensation: Caused by giant papillae contacting the cornea.
Blurred vision: Occurs when corneal epithelial damage or corneal plaques extend to the pupillary area.
In highly active states, patients may be unable to move upon waking due to severe blepharospasm and mucous discharge, a condition called “morning misery.” This significantly impacts school and daily life and can lead to school refusal.
Giant papillae, limbal proliferation, and shield ulcers are highly specific objective findings that are central to the diagnosis of VKC 7).
Findings of the Palpebral Type
Cobblestone giant papillae: Flat papillae exceeding 1 mm in diameter are densely packed on the upper tarsal conjunctiva, presenting a cobblestone appearance. Papillae with a diameter of 1 mm or more are considered giant papillae.
Indicators of activity: The degree of hyperemia, mucoid discharge between papillae, and fluorescein staining of the papillary apices serve as indicators of disease activity.
Observation method: Eversion of the upper eyelid is essential, and evaluation is performed using a slit-lamp microscope.
Findings in the bulbar type
Horner-Trantas spots: White spots observed at the corneal limbus, composed of degenerated epithelial cells and eosinophil aggregates. They are classified as mild, moderate, or severe based on the number of spots around the entire limbus.
Gelatinous limbal elevation: The corneal limbus becomes gelatinously swollen. Limbal papillae may coalesce.
Pseudogerontoxon: In cases with severe limbal inflammation, an opacity resembling an arcus senilis may persist in the peripheral superficial stroma7).
Corneal complications progress in a stepwise manner according to disease severity. Severity increases in the order of punctate superficial keratitis, desquamative punctate superficial keratitis, epithelial erosion, and shield ulcer7).
Punctate superficial keratopathy: This is the first corneal epithelial disorder to appear in mild cases.
Shield ulcer: An oval shallow ulcer forms in the superior cornea. Direct cellular damage to the corneal epithelium by eosinophil-derived major basic protein (MBP) and eosinophil cationic protein (ECP) underlies the pathogenesis.
Corneal plaque: A plaque containing fibrin and mucus deposits on the base of the shield ulcer, causing delayed epithelial regeneration.
Histological examination of the cornea in the cicatricial stage of VKC reveals epithelial hyperplasia, loss of Bowman’s layer, stromal hyalinization, and neovascularization3). Immunohistochemically, ABCG2 (a limbal stem cell marker) is lost while p63 remains, suggesting partial dysfunction of limbal stem cells3). This finding is important for prognostic evaluation after corneal transplantation (DALK or PKP).
A rare complication is tarsal conjunctival keratinization. Bilateral tarsal conjunctival keratinization was first reported in a patient with long-standing VKC (onset in childhood, duration >20 years), and was managed with lesion excision and conjunctival autograft without recurrence for 4 years4). In the same case, corrected visual acuity of 0.8 (20/25) was achieved with scleral lens (PROSE) wear4).
QWhy does shield ulcer occur?
A
MBP (major basic protein) and ECP (eosinophil cationic protein) released from eosinophils cause direct cellular damage to the corneal epithelium. Mechanical friction from giant papillae adds to this, forming an oval shallow ulcer (shield ulcer) in the upper cornea. When fibrin and mucus deposit on the ulcer base, a corneal plaque forms, hindering epithelial regeneration. During the active phase, MBP and ECP have antibacterial effects, making infection less likely; however, indiscriminate use of steroids during remission increases the risk of bacterial keratitis, requiring caution.
VKC cannot be explained solely by simple IgE-mediated type I allergy. CD4-positive Th2 cell-driven type IV hypersensitivity plays a crucial role. In animal model studies, type I allergy alone did not induce conjunctival eosinophil infiltration, whereas involving Th2 cells induced strong conjunctival eosinophil infiltration. This finding indicates that Th2 cells play a central role in the pathogenesis of VKC.
Th2 cells: Produce cytokines such as IL-4, IL-5, and IL-13, promoting eosinophil recruitment and activation.
Eosinophils: Consistently detected in conjunctival scrapings. MBP and ECP have direct cytotoxicity to the corneal epithelium. A correlation between corneal damage, a severity indicator of VKC, and tear eosinophil count has been reported.
Mast cells: Through IgE-mediated degranulation, produce a biphasic response: an immediate phase (histamine release) and a late phase (leukotriene production).
Histopathology of conjunctival giant papillae shows eosinophil infiltration, fibroblast proliferation, extracellular matrix deposition, and numerous T cell infiltrates. Thus, giant papilla formation involves not only type I allergic reactions but also T cell-dependent chronic inflammation.
The most common causative antigens for VKC are house dust and mites; in addition, reactions to many types of antigens such as pollen and animal dander are not uncommon7). Therefore, symptoms may persist year-round rather than only seasonally.
Age and sex: More common in boys aged 5–25 years. Frequently occurs during school age.
Climate: Higher prevalence in hot, dry regions (West Africa, Mediterranean coast, Middle East, India, East Asia). Associations with summer temperature rises and urban heat island effects are also discussed.
Atopic predisposition: Frequent comorbidity or family history of atopic dermatitis, bronchial asthma, and allergic rhinitis.
Endocrine factors: The prevalence decreases after puberty, suggesting the involvement of sex hormones. An increased prevalence of growth hormone deficiency (GHD) has been reported in patients with VKC 5).
VKC and atopic keratoconjunctivitis are allergic corneal diseases and also risk factors for infectious keratitis 6).
QWhy is it more common in boys?
A
The exact mechanism is not understood, but there is a hypothesis that sex hormones promote eosinophil recruitment in the conjunctiva. The gender difference narrows after puberty, and symptoms also improve, suggesting the involvement of endocrine factors. Additionally, boys tend to engage in outdoor activities more frequently than girls, leading to greater antigen exposure, which is considered a contributing factor.
Diagnosis is made in three steps using clinical symptoms (A), type I allergic predisposition (B: systemic and local), and type I allergic reaction in the conjunctiva (C) 7).
Diagnostic category
Requirements
Clinical diagnosis
A only (presence of clinical symptoms characteristic of ACD)
Clinical definitive diagnosis
A + B (clinical symptoms + positive total IgE in tears, positive serum antigen-specific IgE, or positive skin reaction)
Definitive diagnosis
A + B + C or A + C (in addition to above, eosinophils positive in conjunctival scraping)
Important diagnostic criteria for VKC include giant papillae, limbal proliferation, corneal lesions (shield ulcer, corneal plaque), eye pain, discharge, and conjunctival injection7). Clinical diagnosis is made based on characteristic findings (cobblestone giant papillae, Horner-Trantas dots, shield ulcer) and history of itching and eye pain, and confirmed by laboratory tests.
The following tests are combined according to disease type and severity7).
Eosinophil test in conjunctival scraping: After topical anesthesia, evert the upper eyelid, gently massage the tarsal conjunctiva with a glass rod, collect mucus from the conjunctival surface with forceps or a spatula, and smear onto a glass slide. After Hansel staining (Eosinostain®-Torii, Torii Pharmaceutical), the presence of even one eosinophil under light microscopy is considered positive. The positivity rate is high in VKC.
Tear total IgE test (Allerwatch® Tear IgE, Wakamoto Pharmaceutical / Minaris Medical): A rapid diagnostic kit using immunochromatography. The test strip is inserted into the lower conjunctival sac to collect tears. Results are available in about 10 minutes. Sensitivity for ACD is reported as 73.6% and specificity as 100%, with caution needed for false negatives7). The positivity rate by disease type is highest in VKC at 94.7%, followed by AKC 80.5%, GPC 75.0%, PAC 65.4%, and SAC 61.9%7).
Serum antigen-specific IgE antibody test: Select antigens with high positivity rates in allergic conjunctival disease patients, such as mites, house dust, Japanese cedar, orchard grass, and timothy grass (up to 13 items covered by insurance). Multi-item simultaneous testing methods such as View Allergy 39 (Thermo Fisher Diagnostics) and MAST Immunosystems V (Minaris Medical) are available as screening tests under insurance coverage.
Skin test: Perform a prick test or scratch test. A wheal with a maximum diameter of 3 mm or more, or a reaction at least half the size of the positive control wheal, is considered positive. Exercise caution in patients with severe bronchial asthma, history of anaphylaxis, or significant cardiovascular disease.
Conjunctival provocation test: Not covered by insurance, and no standard solution is commercially available, so it is rarely performed except for research purposes.
Eversion of the upper eyelid is essential: Giant papillae commonly occur on the upper tarsal conjunctiva, so observation after eyelid eversion is key to diagnosis.
Use of fluorescein staining: Active papillae may stain at the apex with fluorescein. Additionally, shield ulcers, superior corneal epithelial defects, Horner-Trantas dots, and limbal lesions in mild cases are often first noticed after staining. Using a blue-free filter enhances contrast and facilitates observation.
Papillae with a diameter of 1 mm or more are called giant papillae: This serves as a diagnostic basis for vernal keratoconjunctivitis (VKC) and giant papillary conjunctivitis (GPC).
Atopic keratoconjunctivitis (AKC): Onset in the 20s to 50s, primarily involves the lower tarsal conjunctiva, chronic course with conjunctival sac shortening and symblepharon. Atopic dermatitis is a prerequisite.
Seasonal and perennial allergic conjunctivitis (SAC/PAC): No conjunctival proliferative changes. Papillae remain mild.
Giant papillary conjunctivitis (GPC): Caused by mechanical irritation from contact lenses, ocular prostheses, or surgical sutures. Rapid improvement upon removal of the cause is a major difference from VKC.
Viral conjunctivitis: Unilateral onset, preauricular lymphadenopathy, and follicular formation. Caused by adenovirus, herpes simplex, varicella-zoster, enterovirus, etc.
Chlamydial conjunctivitis: Characterized by giant follicles in the lower fornix.
QHow accurately can VKC be diagnosed with the Allerwatch tear IgE test?
A
In vernal keratoconjunctivitis cases, the positive rate of the Allerwatch tear IgE test is reported to be 94.7%, showing a high positivity rate among allergic conjunctival diseases7). For allergic conjunctival diseases overall, the sensitivity is 73.6% and specificity is 100%; while specificity is high, sensitivity has limitations, so it is important to interpret results in conjunction with clinical findings, keeping false negatives in mind. The test is a simple rapid diagnostic kit using immunochromatography, and results can be obtained in about 10 minutes by inserting a test strip into the lower conjunctival sac.
Treatment of VKC is based on the Japanese Guidelines for the Management of Allergic Conjunctival Disease, 3rd Edition (2021)7). Since VKC involves Th2 cells playing a central role in pathogenesis, it cannot be controlled with anti-allergic eye drops alone, which lack T-cell suppressive effects. Combination with immunosuppressive eye drops or steroid eye drops that regulate T-cell function is necessary.
Used as immunosuppressive eye drops depending on conditions
May help reduce steroid dose or prevent recurrence
Tacrolimus eye drops
Primary treatment with relatively strong evidence of efficacy
Particularly important in severe cases, steroid-resistant cases, and steroid responders
Combination of immunosuppressive and steroid eye drops
Considered for severe proliferative changes
Gradually taper steroids based on disease activity
A meta-analysis of tacrolimus ophthalmic solution showed improvement in corneal epithelial damage score with a standardized mean difference of -0.89 (95% CI -1.32 to -0.46) and in palpebral papillae score with -0.83 (95% CI -1.68 to 0.03)7). Since no increase in intraocular pressure was observed, it is positioned as a major treatment option for VKC7).
Mediator release inhibitors: Stabilize mast cell membranes and inhibit histamine release. Examples include sodium cromoglicate.
H1 receptor antagonists: Competitively inhibit histamine binding to receptors. Examples include olopatadine and epinastine. Selected when itching is severe. Administered prophylactically as initial treatment before the season.
Immunosuppressive eye drops
Cyclosporine ophthalmic solution (Papilock Mini® 0.1%): Launched in 2006. Instilled 3 times daily. Covered by insurance for VKC. In a post-marketing all-case survey, significant improvement in both subjective and objective findings was observed from 1 month after starting instillation, and many cases reported reduction or discontinuation of steroid eye drops.
Tacrolimus ophthalmic solution (Talymus® 0.1%): Launched in 2008. Instilled twice daily. Covered by insurance only for VKC (not covered for AKC). Has stronger immunosuppressive effect than cyclosporine and is effective in steroid responders7).
Anti-allergic eye drops are used as the foundation, and immunosuppressive eye drops or steroid eye drops are added depending on severity and corneal lesions 7).
Foundation eye drops: 1) Patanol® 4 times daily or 2) Alesion® 4 times daily
During exacerbation: Add 3) Talymus® (tacrolimus) 2 times daily or 5) Flumetholon® 4 times daily
If no improvement: Change 5) Flumetholon® to 3) Talymus®, or add 4) Papilock Mini® (cyclosporine) 3 times daily
If no improvement with 3 agents: Change 4) to 3) Talymus®
If still no improvement: Change 5) Flumetholon® to 6) Rinderon®
If uncontrollable with above: Consider oral steroids or surgical giant papilla resection
After improvement, first taper and discontinue steroid eye drops, then taper immunosuppressive eye drops. In case of recurrence, restart immunosuppressive eye drops, and add steroid eye drops if still not controlled.
VKC is common in young people, and it is important to note that younger individuals have a higher proportion of steroid responders (steroid-induced glaucoma). Regular visits and intraocular pressure measurements are essential. High-potency steroids (Rinderon®) provide rapid effects but carry the risk of a vicious cycle of self-discontinuation upon improvement and subsequent worsening. Particularly after age 10, when medication management shifts from guardians to the patient, attention should be paid to decreased self-management ability.
During remission, indiscriminate continuation of steroids increases the risk of bacterial keratitis, unlike the active phase where MBP and ECP maintain antibacterial effects. In cases complicated by atopic dermatitis, attention should also be paid to MRSA carriage/infection and induction of herpes simplex.
Shield ulcer / corneal plaque: Scrape the ulcer base or plaque with a golf knife or spatula. In principle, this should be performed after VKC has remitted. Performing it during the active phase may lead to persistent epithelial defects and increased infection risk.
Excimer laser phototherapeutic keratectomy (PTK): Selected when corneal opacity remains after plaque removal. It often allows removal of opacity without leaving residual scarring.
Amniotic membrane transplantation: Performed to cover persistent epithelial defects. The amniotic membrane has anti-inflammatory and wound-healing promoting effects and is effective as a covering material for shield ulcers and persistent corneal epithelial defects. After surgery, continued control of the underlying disease with immunosuppressive eye drops is necessary.
If control is not achieved with immunosuppressive eye drops and steroid eye drops, consider the following:
Oral steroids: Oral steroids in children pose a risk of growth impairment, so the prescription period should be as short as possible. If long-term administration is necessary, collaboration with a pediatrician is essential.
Local steroid injection (subtarsal injection): Pay particular attention to elevated intraocular pressure.
Surgical giant papilla resection: Performed to remove inflammatory masses; complete resection is not necessary. It provides rapid effects, but continued use of immunosuppressive and steroid eye drops after surgery is essential. With advances in immunosuppressive eye drops, the need for surgical treatment has significantly decreased.
Prevention and self-care emphasize the following 7):
Removal of indoor dust mites: Keep the room clean at all times, and manage room temperature and humidity. Wash bedding at least once a week and vacuum frequently.
Pollen countermeasures: Wear goggles or sunglasses when going out, and wash face after returning home.
Cold compresses: Cool the eyelid skin with a cold pack.
Artificial tear eye drops: Dilute antigens.
Instruction to avoid eye rubbing: Avoiding mechanical irritation also helps reduce the risk of developing keratoconus.
Initial treatment: If the season when symptoms worsen is known, starting anti-allergic eye drops before the season is effective.
QHow are cyclosporine and tacrolimus used differently?
A
Tacrolimus (Talymus®) has a stronger immunosuppressive effect than cyclosporine (Papilock Mini®) and is an important option for severe cases, cases unresponsive to cyclosporine, and steroid responders 7). Cyclosporine is considered more effective for the bulbar type of VKC, while tacrolimus is considered more effective for cases complicated by atopic dermatitis. Anti-allergic eye drops, cyclosporine, tacrolimus, and steroid eye drops are selected stepwise according to severity 7). Proactive therapy with tacrolimus (continued at low frequency after remission) is effective in preventing relapse.
The pathophysiology of VKC is a complex immune reaction involving both type I allergy (immediate type) and type IV hypersensitivity (delayed type).
In type I allergy, antigens that enter the tear fluid trigger mast cell degranulation via IgE. In the immediate phase, histamine is released, causing congestion and itching; in the late phase, newly synthesized mediators such as leukotrienes amplify inflammation.
In type IV hypersensitivity, Th2 cells produce IL-4, IL-5, and IL-13, promoting eosinophil recruitment and activation. Activated eosinophils release cytotoxic proteins such as MBP and ECP, causing direct damage to the corneal epithelium. Animal experiments have shown that type I allergy alone cannot induce conjunctival eosinophil infiltration, but the involvement of Th2 cells induces strong conjunctival eosinophil infiltration. This finding supports the central role of Th2 cells in VKC.
In recent years, the JAK/STAT pathway has been recognized as playing an important role in Th2 cytokine signaling. JAK1 mediates signaling of IL-4, IL-5, IL-13, IL-31, and TSLP (thymic stromal lymphopoietin), making it a central pathway in allergic inflammation 1). Therefore, JAK inhibitors are attracting attention as a new treatment option for refractory VKC.
Histopathological findings of conjunctival giant papillae show eosinophil infiltration, fibroblast proliferation, extracellular matrix deposition, and numerous T-cell infiltrates. The basic pathology of papillae is an angiogenic response, accompanied by thickening of the conjunctival epithelium and subepithelial inflammatory cell proliferation, with fibrous tissue protruding in a papillary shape. A blood vessel is present at the center, surrounded by cell infiltration mainly composed of lymphocytes and plasma cells. Because they occur on the hard tarsal plate, they are common in the upper tarsal conjunctiva.
Histological examination of corneal buttons in the cicatricial phase of VKC revealed epithelial hyperplasia, loss of Bowman’s layer, stromal hyalinization, and neovascularization3). Immunohistochemistry showed loss of ABCG2 (a limbal stem cell marker) while the basal cell marker p63 was retained 3). This finding suggests that VKC-induced limbal stem cell damage is not complete stem cell failure but rather partial functional impairment, which is an important insight for prognosis after corneal transplantation (DALK or PKP) 3).
In an 18-year-old female with severe VKC and atopic dermatitis, marked flattening of giant papillae was achieved 2 months after starting oral upadacitinib, a selective JAK1 inhibitor 1). Although the case was refractory with a markedly elevated serum IgE of 8973 IU/mL, a favorable course was observed in combination with tacrolimus eye drops 1).
JAK1 mediates signaling of Th2 cytokines (IL-4, IL-5, IL-13, IL-31) and TSLP 1). JAK1 inhibition by upadacitinib comprehensively suppresses these cytokines and may represent a new treatment option for severe cases resistant to conventional immunosuppressive eye drops 1).
In a VKC family of monozygotic twins and their father, HLA analysis by NGS (next-generation sequencing) revealed associations of HLA-DQB105:01, HLA-DRB101:01:01, and HLA-A*32:01:01 with VKC 2). This is the first report of NGS-based HLA analysis in VKC 2).
In an immunohistochemical study of corneal tissue from the cicatricial phase of VKC, 3 cases (4 eyes) that underwent DALK or full-thickness corneal transplantation showed epithelial hyperplasia, loss of Bowman’s layer, stromal hyalinization, and neovascularization3). The findings of ABCG2 negativity and p63 positivity led to the conclusion of partial limbal stem cell dysfunction 3).
Bilateral tarsal conjunctival keratinization was reported in a VKC patient with long-term disease duration (over 20 years since childhood onset) 4). This is the first case report of tarsal conjunctival keratinization in VKC 4). It was managed by lesion excision and conjunctival autograft, with no recurrence over 4 years 4). Corrected visual acuity of 0.8 (20/25) was achieved with scleral lens (PROSE) wear 4).
An increased prevalence of growth hormone deficiency (GHD) has been reported in patients with VKC5). In an 11-year-old boy with VKC, GHD was confirmed, and switching to tacrolimus eye drops and fluorometholone eye drops led to marked improvement within 6 weeks5). GH therapy has been reported to reduce inflammatory markers such as CRP and IL-6, drawing attention to the involvement of GHD in the pathology of VKC5).
Effective cases have been reported with omalizumab, an anti-IgE monoclonal antibody. Additionally, clinical trials of dupilumab, an anti-IL-4 receptor alpha antibody, are ongoing for atopic keratoconjunctivitis, and its application to VKC is anticipated. These biologic agents may offer new options for refractory cases that do not respond adequately to conventional immunosuppressive eye drops. However, while dupilumab is widely used for atopic dermatitis in dermatology, it is known to have a high incidence of conjunctivitis and blepharitis as ocular surface side effects, requiring careful risk-benefit assessment when applied to VKC.
Future challenges include accumulating evidence on the long-term use of immunosuppressive eye drops, particularly long-term safety data for tacrolimus eye drops over 10 years, establishing optimal combination protocols with steroid eye drops, follow-up of childhood-onset cases into adulthood, and RCTs on the timing of initial treatment7). Continuous implementation of nationwide epidemiological surveys is also important to track changes in VKC prevalence over time.
QWill JAK inhibitors be used for VKC treatment in the future?
A
There is a case report of upadacitinib (a JAK1-selective inhibitor) being effective for refractory VKC1). Since JAK1 broadly mediates Th2 cytokine signaling, it theoretically has a mechanism of action consistent with the pathology of VKC. However, at present, it is not approved for VKC and remains at the case report stage. Future clinical trials to verify safety and efficacy are expected. Currently, tacrolimus eye drops (Talymus®) remain the main treatment option7).
Mima R, et al. Refractory vernal keratoconjunctivitis with atopic dermatitis improved by upadacitinib: a case report. Am J Ophthalmol Case Rep. 2024;35:102069.
Artesani MC, et al. Next-generation sequencing HLA typing with monozygotic twins and their father with vernal keratoconjunctivitis. Pediatr Allergy Immunol. 2021;32(7):1549-1553.
Jaffet J, et al. Histopathological and immunohistochemical analysis of corneal buttons in vernal keratoconjunctivitis. Ocul Surf. 2022;24:24-32.
Kate A, et al. Tarsal conjunctival keratinization in long-standing vernal keratoconjunctivitis: a case report. BMC Ophthalmol. 2022;22:182.
Fukushima A, Tabuchi H. A Case of Vernal Keratoconjunctivitis With Growth Hormone Deficiency. Cureus. 2022;14(10):e30615. doi:10.7759/cureus.30615. PMID:36426321; PMCID:PMC9681536.
American Academy of Ophthalmology Cornea/External Disease Preferred Practice Pattern Panel. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P1-P47.