Thygeson superficial punctate keratitis (TSPK) is a unique superficial keratitis first reported by Phillips Thygeson in 1950. It presents with recurrent, multiple punctate lesions confined to the corneal epithelium and very superficial stroma, without inflammation of the conjunctiva or corneal stroma.
There is no sex predilection, and it occurs in all age groups, although some studies report a female predominance. The median age of onset is 29 years, with reports ranging from 2.5 to 70 years. The prevalence and distribution may be underestimated.
The clinical course is characterized by repeated exacerbations and remissions. A single episode lasts 1–2 months, and remission takes 6 weeks. Some reports indicate that most cases stop recurring after 4 years, while others persist for more than 20 years, with the longest recorded duration being 41 years. Ultimately, it tends to resolve without clinical sequelae.
QHow does TSPK differ from multiple subepithelial infiltrates after adenoviral keratitis?
A
Both conditions present with multiple punctate to patchy opacities in the corneal epithelium to subepithelium, but they differ clinically. Multiple subepithelial infiltration after adenoviral keratitis has a history of preceding viral conjunctivitis and is often accompanied by conjunctival inflammation. In contrast, TSPK has no history of preceding viral infection, and the conjunctiva is quiet. Additionally, each lesion in TSPK is a cluster of smaller punctate lesions, whereas subepithelial infiltrates appear as relatively homogeneous opacities. If individual lesions are large and patchy, dimmer nummular keratitis should be considered.
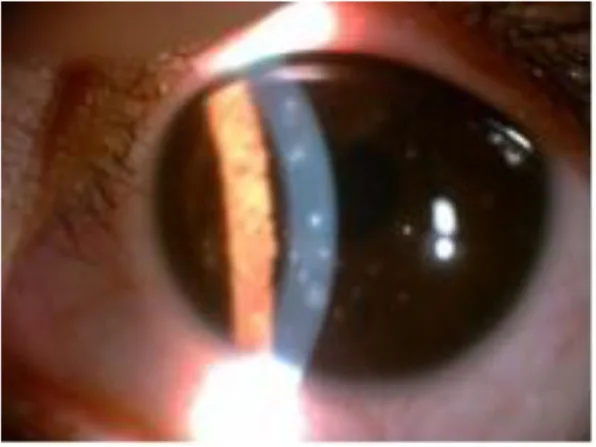
Tang XJ, et al. Thygeson’s superficial punctate keratitis (TSPK): a paediatric case report and review of the literature. BMC Ophthalmol. 2021. Figure 1. PMCID: PMC7845125. License: CC BY.
Slit-lamp photograph showing multiple scattered epithelial lesions in the left eye. These correspond to the corneal infiltrates discussed in the section “2. Main Symptoms and Clinical Findings.”
Punctate intraepithelial opacities: Gray-white, round to stellate, small raised opacities scattered within the central corneal epithelium. Each lesion is a cluster of granular lesions. Typically, about 20 lesions per eye, up to 50, are observed. The peripheral cornea is not involved.
Fluorescein staining: The center of the opacity stains punctately with fluorescein. It may also show a “beading” pattern of fluorescein.
Conjunctival quietness: No conjunctival hyperemia or inflammatory reaction. A few cases may show mild hyperemia or filament formation.
Corneal sensation: Normal or slightly decreased.
Pseudodendritic lesions: Rarely present a dendritic pattern, requiring differentiation from early herpetic keratitis1).
The etiology is unknown, but there are two hypotheses: viral and immunological mechanisms.
The viral hypothesis: In 1974, Lemp et al. reported a case where varicella-zoster virus (VZV) was isolated from the corneal surface of a TSPK patient. However, studies using PCR testing did not detect VZV, making the viral etiology unlikely.
As an immunological mechanism, a significant association with HLA-DR3 has been reported1). HLA-DR3 is a class II MHC molecule also associated with several autoimmune diseases (celiac disease, Addison’s disease, Sjögren’s syndrome, systemic lupus erythematosus). The effectiveness of immunosuppressive drugs such as cyclosporine A and tacrolimus suggests a T-cell-mediated immune mechanism.
Celiac disease is an autoimmune disease strongly associated with HLA-DQ2 and HLA-DQ8, and over 90% of patients carry the HLA-DR3 allele. Tagmouti et al. reported a case of TSPK in a 20-year-old woman with a 4-year history of celiac disease, suggesting that shared HLA-DR3 indicates an immunogenetic link between TSPK and celiac disease1).
QHow is HLA-DR3 related to TSPK?
A
HLA-DR3 is a class II major histocompatibility complex (MHC) molecule involved in regulating immune responses. Darrell et al. reported a significantly higher prevalence of HLA-DR3 in TSPK patients. HLA-DR3 is also associated with several autoimmune diseases such as celiac disease, Addison’s disease, and Sjögren’s syndrome. In TSPK, a T-cell-mediated hypersensitivity reaction to an antigen (possibly viral) within the epithelium is presumed, and HLA-DR3 is thought to increase susceptibility to this immune response1).
Corneal findings: Slightly elevated, gray-white, roundish punctate opacities scattered in the central cornea. Each lesion is an aggregate of granular changes, slightly elevated from the corneal surface.
Fluorescein staining: The center of the opacity stains punctately. Acute lesions stain slightly with fluorescein, but may or may not stain with vital dyes (rose bengal, lissamine green).
Conjunctival findings: The conjunctiva is quiet, characteristically lacking hyperemia or inflammatory reaction.
Confocal microscopy
Starburst-like hyperreflective deposits: Aggregates of starburst-like hyperreflective deposits are seen in the superficial and basal epithelial cell layers.
Langerhans cell infiltration: Infiltration of Langerhans cells into the basal epithelial layer is observed, suggesting involvement of immunological mechanisms.
Anterior stromal opacity: The longer the disease duration, the more severe the changes.
Topical steroids: The main treatment for TSPK. 0.1% fluorometholone eye drops four times daily rapidly resolves lesions. Due to frequent recurrences, topical steroids should be tapered over several months after symptom resolution. Maintain at the lowest possible dose and concentration.
Topical cyclosporine: Effective as an alternative to steroids. Tagmouti et al. administered 2% cyclosporine A eye drops three times daily with a 6-month taper, achieving complete remission. No recurrence was observed during 3 years of follow-up 1).
Tacrolimus: Used as eye drops and ointment, with reported efficacy.
Other Treatments
Artificial tears: Used for partial relief of clinical symptoms. If symptoms are mild, observation alone may suffice.
Therapeutic soft contact lenses: Used in severe cases. They cover raised corneal lesions and reduce friction with the palpebral conjunctiva during blinking. Caution is needed regarding the risk of microbial keratitis.
Ineffective treatments: Antibiotics are ineffective. Idoxuridine is contraindicated because it causes ghost opacities and scarring in the anterior stroma. PTK provides only partial improvement and has a high recurrence rate, so it is not recommended.
QWhat are the precautions for long-term steroid use in TSPK?
A
Since TSPK tends to recur, steroid eye drops may be used for a long period. In such cases, attention must be paid to increased intraocular pressure (steroidglaucoma) and cataract formation. The treatment goal is to use the minimum dose and lowest concentration that controls symptoms. Start with 0.1% fluorometholone and taper over several months after symptoms subside. If steroid side effects are a concern or tolerability is poor, consider switching to cyclosporine eye drops or tacrolimus.
The punctate opacities in TSPK are formed by intraepithelial infiltration of mononuclear cells, mainly lymphocytes. This is thought to be a hypersensitivity reaction to antigens (likely viral antigens) within the epithelium and responds well to low-concentration steroid eye drops.
Intracellular and intercellular edema is observed at the corneal epithelial level. Changes also extend to the subepithelial nerve plexus, Bowman’s layer, and anterior stroma. These changes are more severe in eyes with longer duration of TSPK.
Kobayashi et al. reported three consistent findings in TSPK patients using confocal microscopy. First, aggregates of stellate hyperreflective deposits in the superficial and basal epithelial cell layers. Second, invasion of Langerhans cells into the basal epithelial layer, suggesting involvement of antigen-presenting cells. Third, anterior stromal opacification. These changes can be found not only directly beneath intraepithelial lesions but also in areas without lesions, indicating a widespread immunological impact of the disease.
In advanced stages, subepithelial fibrosis or anterior stromal scarring may be observed. However, generally, scarring does not occur after lesion resolution, and since the lesions are confined to the corneal epithelium, the visual prognosis is good.
QDoes TSPK leave scars on the cornea?
A
Usually, each TSPK lesion resolves without leaving a trace over 4 to 6 weeks. Because the lesions are confined to the corneal epithelium, scarring after resolution is not observed. However, in long-standing cases, faint subepithelial opacities or anterior stromal scarring may occur. Confocal microscopy has reported that anterior stromal changes are more pronounced in eyes with longer disease duration. Overall, the visual prognosis is good.
Tagmouti et al. reported a case of TSPK in a 20-year-old woman with a 4-year history of celiac disease 1). Celiac disease is strongly associated with HLA-DQ2 and HLA-DQ8, and more than 90% of patients carry the HLA-DR3 allele. An association with HLA-DR3 has also been reported in TSPK, suggesting an immunogenetic link between the two diseases 1).
Tagmouti et al. state that “in cases of TSPK, screening for celiac disease should be considered given the common genetic predisposition” 1).
In this case, complete remission was achieved with a 6-month tapering regimen of cyclosporine A 2% eye drops three times daily, and no recurrence was observed during 3 years of follow-up 1). The efficacy of cyclosporine as an immunomodulatory therapy has been reconfirmed, and the importance of future research exploring the relationship between TSPK and autoimmune diseases has been demonstrated 1).
Tagmouti A, Lazaar H, Benchekroun M, et al. Association Between Thygeson Superficial Punctate Keratitis and Celiac Disease. Cureus. 2025;17(3):e80252. doi:10.7759/cureus.80252.
Moshirfar M, Peterson T, Ungricht E, McCabe S, Ronquillo YC, Brooks B, et al. Thygeson Superficial Punctate Keratitis: A Clinical and Immunologic Review. Eye Contact Lens. 2022;48(6):232-238. PMID: 35301272.