Superficial punctate keratitis (superficial punctate keratitis / superficial punctate keratopathy: SPK) is a condition in which the outermost cells of the corneal epithelium are shed in a punctate pattern due to various causes. When fluorescein vital staining is performed, the epithelial defects appear as punctate or clustered staining patterns. The basal cell layer is preserved; when damage extends deeper, it is called corneal erosion, and when it reaches the stroma, it is called corneal ulcer.
As an important premise, SPK is merely a ‘finding’ and not an independent disease name. It is most frequently observed as a finding in patients presenting with foreign body sensation in ophthalmology outpatient clinics, and a variety of underlying diseases may be hidden behind it. Therefore, in the management of SPK, identifying the cause is the first step in determining the treatment strategy.
On the other hand, what is exceptionally treated as an independent disease entity is Thygeson superficial punctate keratitis (Thygeson superficial punctate keratitis: TSPK). TSPK is a bilateral, recurrent corneal epithelitis reported by Phillips Thygeson in 1950, and is described in a separate section as idiopathic superficial keratitis for which no clear underlying disease can be identified.
SPK is not a disease name but rather a “clinical finding” observed as a result of corneal epithelial damage from various causes. Since definitive treatment is not possible without identifying the underlying cause, a thorough etiological investigation is required whenever SPK is observed. Only Thygeson superficial punctate keratitis is exceptionally treated as an independent disease entity.
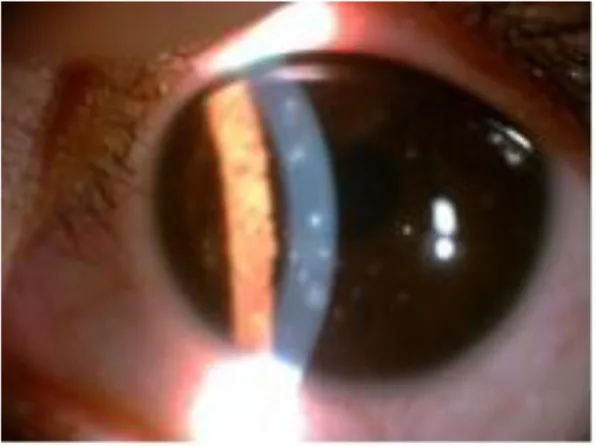
Tang XJ, et al. Thygeson’s superficial punctate keratitis (TSPK): a paediatric case report and review of the literature. BMC Ophthalmology. 2021;21:64. Figure 1. PMCID: PMC7845125. License: CC BY.
A slit-lamp photograph showing multiple isolated epithelial lesions (left eye). These correspond to the punctate epithelial lesions discussed in the section “2. Main Symptoms and Clinical Findings”.
The symptoms reported by patients are diverse, and nearly all symptoms that can occur in ophthalmic diseases may appear with SPK.
Foreign body sensation: The most frequent symptom, and the most common underlying condition among outpatients presenting with foreign body sensation as the chief complaint.
Pain/Ocular pain: Accompanied by mild to moderate pain depending on the extent of epithelial damage.
Decreased visual acuity/Blurred vision: Occurs when lesions extend into the pupillary area.
Photophobia: Sensitivity to light. Becomes prominent during exacerbation phases.
In many cases, slit-lamp microscopy cannot visually observe the lesion, making fluorescein vital staining the cornerstone of diagnosis. Staining patterns vary in morphology, including punctate, vortex-shaped, and crack-line patterns, with staining characteristics differing depending on the severity of the damage.
Observation points: Extend the observation area to the superior bulbar conjunctiva. Check for the presence of giant papillae and trachoma-like follicles.
Central Type
Main causative diseases: Neurotrophic keratopathy, Thygeson superficial punctate keratitis, mechanical damage from eyelashes, hard contact lens (HCL) related disorders, dry eye.
Key observation point: Check corneal sensitivity and eyelash status.
Diffuse: Drug toxicity (topical medication toxicity, antineoplastic drug side effects), severe dry eye, SCL related disorder, corneal epithelial dystrophy (Meesmann etc.).
Localized type: Conjunctival foreign body, herpes infection, 3 o’clock and 9 o’clock staining in CL wearers.
Mild SPK: Scattered punctate staining. Mild to moderate subjective symptoms.
Late staining (bath-powder keratopathy): Finding of fluorescein pooling some time after instillation. Indicates epithelial barrier dysfunction. Frequent in drug toxicity.
Hurricane keratopathy: A swirling staining pattern in the central cornea. A moderate finding of drug toxicity.
Epithelial crack line: Crack-like linear defects. A severe form of drug toxicity.
Persistent epithelial defect: A condition in which SPK progresses to widespread epithelial loss.
Findings of Thygeson Superficial Punctate Keratitis
TSPK is a distinct disease entity different from common cause-specific SPK and presents with characteristic clinical features.
Bilateral and recurrent: Usually bilateral, with a course of repeated exacerbations and remissions.
Elevated lesions in the central cornea: Gray-white, round to oval, slightly elevated punctate opacities are scattered. Each lesion is an aggregate of granular changes, typically about 20 per eye, up to a maximum of approximately 50.
Quiet conjunctiva: The absence of conjunctival injection or inflammatory reaction is an important clue for differential diagnosis.
Fluorescein staining: The center of the lesion stains in a punctate pattern. The corneal epithelium surrounding the lesion is normal.
Corneal sensation: Remains normal or only mildly decreased.
Frequency of subjective symptoms: Foreign body sensation 48.8%, photophobia 41.9%, blurred vision 36.0%, tearing 15.1%. Eye pain is rare.
Duration of illness: A single episode lasts 1–2 months, with approximately 6 weeks needed for remission. Recurrences may persist for years to decades, with the longest reported case lasting 41 years. Ultimately, it tends to resolve without scarring.
QTo what extent can the cause be narrowed down from the staining pattern?
A
The distribution pattern of fluorescein staining is a valuable clue for estimating the cause. Superior staining suggests superior limbic keratoconjunctivitis or allergy; central staining suggests neurotrophic keratopathy, Thygeson SPK, or HCL-related disorder; inferior and interpalpebral staining suggests dry eye or MGD; diffuse staining suggests drug toxicity or severe dry eye. However, the cause cannot be determined by staining pattern alone, and comprehensive evaluation of tear function, eyelids, corneal sensation, medications, and systemic disease is necessary.
Aqueous tear-deficient dry eye: Caused by decreased basal tear secretion. Schirmer I test ≤5 mm and tear breakup time ≤5 seconds are diagnostic guidelines3). Aging, Sjögren’s syndrome, rheumatoid arthritis, and anticholinergic medications are risk factors.
Short tear break-up time (BUT) dry eye: Tear volume is maintained but tear film stability is reduced, causing tear film breakup immediately after blinking. It is associated with VDT work, air conditioning, contact lens wear, and other factors3).
Meibomian gland dysfunction (MGD): Obstruction of the meibomian gland openings or abnormal lipid secretion impairs the oily layer of the tear film, resulting in evaporative dry eye and refractory SPK1,4). SPK in the lower to interpalpebral region is typical.
Hard contact lens-related disorder: Causes SPK localized to the central cornea. Prolonged wear time and poor lens fitting are risk factors.
Soft contact lens-related disorder: Presents with diffuse or inferior SPK. Lens contamination, prolonged wear time, and insufficient oxygen permeability are associated factors9). Three-and-nine-o’clock staining is a circular localized SPK that is characteristic of contact lens wear.
Trichiasis and entropion: Eyelashes scratch the corneal surface, causing mechanical damage.
Conjunctivochalasis: Redundant conjunctiva encroaches on the lower palpebral fissure, increasing friction during blinking.
Drug-induced toxic keratopathy: Preservatives in eye drops (benzalkonium chloride: BAC) are the primary cause, but the active ingredient’s toxicity can also be responsible. It is frequently reported with antiglaucoma medications, antibiotics, antifungals, antivirals, NSAID eye drops, beta-blockers, and topical anesthetics. Mild cases present with dry eye-like SPK in the interpalpebral fissure to inferior cornea, while severe cases progress to hurricane keratopathy, epithelial crack lines, and persistent epithelial defects. Long-term toxic exposure to eye drops can trigger limbal stem cell deficiency and pseudopemphigoid. Systemic administration of anticancer drugs such as TS-1 causes epithelial damage originating from the superior corneal limbus.
Phlyctenular keratitis (Meibomian keratoconjunctival epitheliopathy): A bilateral recurrent keratitis associated with meibomianitis, mediated by type IV allergy.
Herpes simplex virus keratitis (epithelial type): Typically presents as unilateral, with decreased corneal sensation and dendritic ulceration. In early stages, punctate or stellate epithelial findings may appear, requiring differentiation from SPK7).
Adenovirus keratitis: Observed as multiple subepithelial infiltrates associated with epidemic keratoconjunctivitis. A history of preceding conjunctivitis is a key differentiating feature.
Neurotrophic keratopathy: Corneal sensation decreases due to trigeminal nerve damage, leading to failure of epithelial repair and central-type SPK. Causes include corneal herpes, herpes zoster ophthalmicus, after trigeminal nerve surgery, and brainstem lesions.
Lagophthalmic keratopathy: The lower cornea becomes dry due to incomplete eyelid closure. Underlying conditions include facial nerve palsy, thyroid eye disease, orbital tumor, nocturnal lagophthalmos, and coma.
Diabetic keratopathy: Caused by diabetic neuropathy and decreased epithelial adhesion.
An idiopathic recurrent bilateral corneal epitheliopathy. An association with HLA-DR3 has been reported, suggesting an immunological mechanism2). An association with celiac disease has been reported through shared HLA-DR32). Immunosuppressive drugs such as cyclosporine A and tacrolimus are effective, suggesting a T-cell-mediated immune response. A viral etiology has also been proposed, but PCR studies have not identified a causative virus.
Collagen diseases such as rheumatoid arthritis, diabetes, and atopic dermatitis can be underlying conditions for SPK. Inquiring about systemic diseases is important when formulating a treatment plan.
The management of SPK involves not only confirming the clinical findings but also systematically investigating what is causing the epithelial damage—this is key to determining the treatment strategy.
History taking: Inquire about acute/chronic onset, unilateral/bilateral involvement, contact lens wear history, use of eye drops and systemic medications, history of trauma or foreign body exposure, and systemic diseases (rheumatoid arthritis, diabetes, atopy, Sjögren syndrome, etc.). Acute unilateral cases suggest exogenous causes (foreign body, chemicals), while chronic bilateral cases suggest endogenous causes (dry eye, MGD, drug toxicity).
Slit-lamp examination: Check for inflammatory findings such as subepithelial infiltrates, conjunctival injection, and anterior chamber inflammation.
Fluorescein vital staining: Estimate the cause based on the staining pattern (see CardGrid in Section 2).
Schirmer test I: Measures basal and reflex tear secretion. A value of 10 mm or more after 5 minutes is normal, while 5 mm or less suggests hyposecretory dry eye.
Tear break-up time (BUT): After fluorescein instillation, the patient maintains eyelid opening and the time until dry spots appear on the tear film is measured. A value of 5 seconds or less is considered abnormal and serves as a diagnostic criterion for short BUT-type dry eye3,8).
Tear meniscus observation: Evaluate the height of the tear meniscus at the lower eyelid margin. It shows low values in hyposecretory dry eye.
Cochet-Bonnet corneal aesthesiometer: Sensitivity decreases in conditions such as corneal herpes, diabetic keratopathy, post-LASIK, long-term contact lens wearers, and facial nerve palsy. Decreased sensation reduces reflex tear secretion, exacerbating SPK.
Confocal microscopy: In Thygeson SPK, stellate hyperreflective deposits are observed in the superficial and basal epithelial cell layers, Langerhans cell infiltration into the basal epithelial layer, and anterior stromal opacities. Changes are more severe in eyes with longer disease duration.
Tear fluid testing: Lactoferrin quantification, MMP-9 testing, and others are used as supplementary tests.
Systemic disease screening: Anti-SS-A/SS-B antibodies, HbA1c, serum IgE, and others are evaluated as needed.
Inferior SPK, shortened BUT, tear film abnormalities
Drug-induced toxic keratopathy
History of eye drops, interpalpebral SPK, late staining
Allergic keratoconjunctivitis
Superior SPK, giant papillae, itching
Neurotrophic keratopathy
Central SPK, decreased corneal sensation
Lagophthalmic keratopathy
Incomplete eyelid closure, inferior SPK
QWhat methods are available for assessing SPK severity?
A
Typical quantitative assessment methods include the AD classification, which evaluates the area and density of SPK on a 3-point scale each, and the fluorescein staining score on a 9-point scale, which divides the cornea into 3 regions and rates each from 0 to 3. Internationally, the NEI scale (15 points), which divides the cornea into 5 regions, is also used. Both are useful for tracking changes over time and evaluating treatment efficacy.
The basic principle of SPK treatment is the combination of “removing the cause” and “protecting and repairing the corneal epithelium”. Since treatment strategies vary significantly depending on the underlying disease, the approaches by cause are shown below.
Tear Supplementation and Protection
Sodium hyaluronate ophthalmic solution: Hyalein ophthalmic solution (0.1%) 4 to 6 times daily. It improves subjective symptoms, tear film stability, and corneal disorders, and its use is recommended in the dry eye clinical practice guidelines3).
Artificial tears: Preservative-free formulations are preferable. They are the first choice in mild cases or cases of drug toxicity.
Eye ointment: Used for corneal protection before bedtime. Tarivid eye ointment (0.3%) is a representative example.
Improving Tear Film Dynamics
Diquafosol sodium ophthalmic solution: Diquas ophthalmic solution (3%) 6 times daily. It promotes membrane-associated mucin expression and water secretion, and is effective for dry eye with shortened BUT. Clinical trials have shown improvement in subjective symptoms and epithelial damage, and it is recommended in the dry eye clinical practice guidelines3).
Rebamipide ophthalmic solution: Mucosta ophthalmic solution UD (2%) 4 times daily. It possesses both mucin production promotion and anti-inflammatory effects. Improvement in subjective symptoms and epithelial damage has been demonstrated, and it is also recommended3).
First-line: Hyalein ophthalmic solution (0.1%) 4–6 times daily.
Combination for shortened BUT type:
Diquas ophthalmic solution (3%) 6 times daily, or
Mucosta ophthalmic solution UD (2%) 4 times daily.
Severe cases: Perform punctal plug insertion or punctal suture. Compared with conventional eye drops, these procedures significantly improve subjective symptoms, tear film stability, and epithelial disorders3).
Adjuvant: Corticosteroid eye drops are useful for improving subjective symptoms and tear film stability, but should be used with attention to intraocular pressure elevation3).
Adjuvant therapy: If hyperemia or follicular conjunctivitis is prominent, consider low-concentration steroid eye drops, but be mindful of delayed wound healing.
Neurotrophic Keratopathy, Diabetic Keratopathy, and Exposure Keratopathy
Mild cases: If symptoms are mild, observation alone is sufficient.
Symptomatic cases: Fluorometholone ophthalmic solution (0.1%) 4 times daily.
Tapering: Because relapses recur, steroid eye drops should be tapered over several months even after symptoms subside, reducing to a maintenance dose of once weekly to every other week.
Alternative therapy:
A case report described cyclosporine A 2% eye drops 3 times daily tapered over 6 months, with no recurrence during 3 years of follow-up2).
Tacrolimus eye drops/ointment.
Therapeutic soft contact lenses (mechanical covering of raised lesions).
Contraindications & inefficacy: Do not use idoxuridine as it causes ghost opacities and anterior stromal scarring. Antibiotics are ineffective. Superficial keratectomy (PTK) is not recommended as it provides only partial improvement and has a high recurrence rate.
QHow are diquafosol and rebamipide used differently for SPK due to dry eye?
A
Both are ophthalmic solutions recommended for use in the dry eye clinical practice guidelines, but their mechanisms of action differ. Diquafosol sodium (Diquas ophthalmic solution 3%) promotes membrane-bound mucin expression and water secretion, and helps extend the tear film lipid layer, making it the first consideration in shortened BUT-type dry eye. Rebamipide (Mucosta ophthalmic solution UD 2%) has anti-inflammatory effects in addition to promoting mucin production, and is useful in cases involving ocular surface inflammation. Both are used in combination with sodium hyaluronate ophthalmic solution, and the attending physician selects based on the individual case3).
The corneal epithelium is constantly renewed through turnover from the basal cell layer. SPK is understood as an initial state in which the balance of turnover is disrupted due to increased shedding of the most superficial cells or decreased cell supply from the basal layer. In practice, the former, i.e. increased shedding, is the main cause in many cases.
Dry eye: Instability of the tear film causes drying of the ocular surface and stress on epithelial cells. Activation of inflammatory cytokines (IL-1, TNF-α) and MMP-9 disrupts the epithelial barrier6).
Meibomian gland dysfunction: Qualitative and quantitative abnormalities of meibomian gland lipids impair the tear film lipid layer, leading to increased evaporation and tear film instability1). Chronic inflammation creates a vicious cycle in which obstruction of the meibomian glands progressively worsens.
Drug toxicity: The preservative benzalkonium chloride (BAC) disrupts the phospholipid layer of corneal epithelial cell membranes, impairing barrier function. Even mild epithelial damage is visualized as late staining, where fluorescein readily penetrates. Long-term exposure leads to limbal stem cell dysfunction.
Neurotrophic keratopathy: Loss of trigeminal nerve innervation disrupts the supply of neurotrophic factors (substance P, CGRP, NGF), reducing epithelial adhesion and wound healing capacity.
Immunological mechanisms of Thygeson superficial punctate keratitis
In Thygeson SPK lesions, mononuclear cell infiltration predominantly composed of lymphocytes is observed within the epithelium. Findings supporting an immunological mechanism include the following.
Association with HLA-DR3: A significantly higher prevalence of HLA-DR3 has been reported in affected individuals2). HLA-DR3 is a class II major histocompatibility complex (MHC) molecule responsible for antigen presentation to T cells.
Langerhans cell invasion: Confocal microscopy consistently demonstrates invasion of Langerhans cells into the basal epithelial layer. Activation of antigen-presenting cells contributes to the pathogenesis.
Association with autoimmune diseases: Cases of comorbidity with HLA-DR3-related autoimmune diseases such as celiac disease, Addison disease, Sjögren syndrome, and systemic lupus erythematosus have been reported2).
Efficacy of immunosuppressive agents: Low-concentration corticosteroids, cyclosporine A, and tacrolimus are effective, suggesting a T-cell-mediated immune reaction.
In Thygeson SPK, intracellular and intercellular edema and subtle changes in the subepithelial nerve plexus, Bowman’s layer, and anterior stroma are observed. These changes are more severe in eyes with a longer disease duration. However, the lesions usually resolve without scarring, and the visual prognosis is favorable.
Tagmouti et al. reported a case of Thygeson SPK developing in a 20-year-old woman with a 4-year history of celiac disease2). Celiac disease is an autoimmune disorder strongly associated with HLA-DQ2 and HLA-DQ8, with over 90% of patients carrying the HLA-DR3 allele. An association with HLA-DR3 has also been previously suggested in Thygeson SPK, indicating an immunogenetic link between the two diseases.
Tagmouti et al. stated that “in cases of Thygeson superficial punctate keratitis, screening for celiac disease should be considered given the shared genetic predisposition”2).
In this case, complete remission was achieved with a 6-month tapered regimen of cyclosporine A 2% eye drops three times daily, with no recurrence during 3 years of follow-up2). This further confirms the efficacy of topical cyclosporine as an immunomodulatory therapy and highlights the importance of future research exploring the relationship between Thygeson SPK and autoimmune diseases.
With the development of targeted treatments for each layer of the tear film (lipid, aqueous, and mucin layers), pathology-based treatment options are expanding even for cases presenting with SPK as the main symptom. The TFOS DEWS III (2025) advocates for functional assessment of the tear film layers and personalized treatment strategies6,10). Biologic agents, intense pulsed light (IPL) therapy, and novel mucin secretagogues are under research and development.
Tagmouti A, Lazaar H, Benchekroun M, Boutaj T, Benchekroun S, Amazouzi A, et al. Association Between Thygeson Superficial Punctate Keratitis and Celiac Disease. Cureus. 2025;17(3):e80252. doi:10.7759/cureus.80252. PMID:40196095; PMCID:PMC11975144.
Jones L, Downie LE, Korb D, Benitez-Del-Castillo JM, Dana R, Deng SX, et al. TFOS DEWS II Management and Therapy Report. The ocular surface. 2017;15(3):575-628. doi:10.1016/j.jtos.2017.05.006. PMID:28736343.