Superior limbic keratoconjunctivitis (SLK) is a localized chronic inflammatory ocular surface disease primarily affecting the superior bulbar conjunctiva and limbus. It was first reported by Frederick Theodore in 1963 1). This condition is characterized by: (1) inflammation of the upper tarsal conjunctiva, (2) inflammation of the superior bulbar conjunctiva, (3) punctate vital staining of the superior cornea and limbus, (4) proliferation of the superior limbus, and (5) filamentary keratitis of the superior quadrant of the cornea or limbus.
It commonly occurs in individuals aged 50 years and older, with a female predominance (male-to-female ratio 1:3). It is often bilateral but may be asymmetric 2,13). Thyroid disease is present in 20–50% of SLK patients 2). However, the prevalence of SLK in thyroid eye disease is low, about 3%. Conversely, approximately 8% of patients with thyroid dysfunction have been reported to have SLK. Aqueous tear-deficient dry eye is found in about 25% of cases, and friction-related conditions including meibomian gland dysfunction (MGD) have been shown to worsen dry eye severity in Japanese populations 3).
When similar findings occur in contact lens (CL) wearers, it is classified as contact lens-related SLK (CL-SLK). Poor fitting or increased upper eyelid pressure are causative factors.
QHow is SLK related to thyroid disease?
A
In hyperthyroidism with proptosis, the upper eyelid pressure is relatively increased. This leads to enhanced friction between the upper eyelid undersurface and the superior cornea and conjunctiva, triggering SLK. Since 20–50% of SLK patients have thyroid disease, thyroid function tests are recommended when SLK is diagnosed.
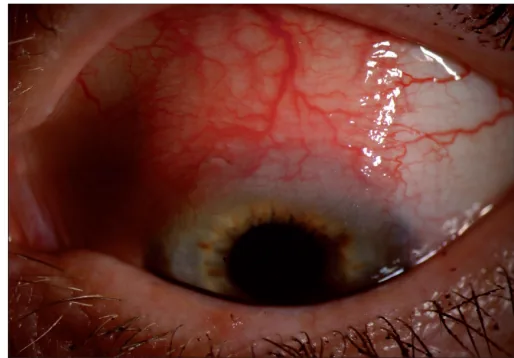
Moshirfar M, et al. Ocular surface squamous neoplasia masquerading as superior limbic keratoconjunctivitis. Middle East Afr J Ophthalmol. 2011. Figure 1a. PMCID: PMC3085160. License: CC BY.
In the superior bulbar conjunctiva exposed during downward gaze, hyperemia, conjunctival thickening, and dilated vessels centered on the superior limbus are seen. This shows typical clinical findings of superior limbic keratoconjunctivitis, corresponding to the description of main symptoms and clinical findings.
Localized hyperemia of the superior bulbar conjunctiva: Fan-shaped hyperemia localized from 10 to 2 o’clock, accompanied by mild swelling.
Epithelial keratinization: The epithelium of the superior bulbar conjunctiva becomes keratinized and stains positively with rose bengal or lissamine green 5).
Thickening and elevation of the superior limbus: In severe cases, a dike-like elevation may be present.
Epithelial damage of the superior cornea: Observed as punctate keratopathy or filamentary keratitis.
Papillary hypertrophy of the upper tarsal conjunctiva: Hyperemia and fine papillary reaction are seen in the upper tarsal conjunctiva adjacent to the lesion.
Coiled vascular abnormalities: A characteristic finding in the superior bulbar conjunctiva.
Superior conjunctivochalasis: Often coexists; when the patient looks downward and the upper eyelid is rubbed downward, the loose conjunctiva can be seen protruding into the superior tear meniscus.
The etiology is unknown. The most supported hypothesis is Cher’s friction theory, which proposes a multifactorial pathogenesis resulting from mechanical friction of the superior bulbar conjunctiva4). Relaxation of the superior bulbar conjunctiva leads to constant friction between the upper tarsal conjunctiva and the superior bulbar conjunctiva during blinking. This friction is thought to be the initial trigger for the development of SLK.
The following factors contribute to increased friction upstream:
Factor
Mechanism
Superior bulbar conjunctival laxity
Increased friction area and intensity during blinking
Hyperthyroidism
Relative increase in eyelid pressure due to proptosis
Decreased tear production
Increased friction due to insufficient lubrication
Secondary worsening of tear film lipid layer deficiency and increased friction3)
In the affected area, impaired epithelial differentiation leads to squamous metaplasia and a decrease in goblet cells. The reduction in goblet cells thins the mucin layer on the ocular surface, which further increases friction and creates a vicious cycle of persistent inflammation.
Slit-lamp microscopy: Check for folds, hyperemia, laxity, and filament formation in the superior bulbar conjunctiva. Eversion of the upper eyelid is essential.
Vital staining: Evaluate punctate staining of the superior bulbar conjunctiva, limbus, and superior cornea using fluorescein (blue-free filter recommended), rose bengal, and lissamine green5).
Impression cytology: A definitive diagnostic test that demonstrates keratinization of the conjunctival epithelium. Characteristic findings include snake-like appearance of condensed nuclear chromatin and loss of goblet cells in the palpebral conjunctiva.
Systemic examination
Thyroid function tests: In addition to T₃, T₄, and TSH, test for thyroid-stimulating antibodies, anti-peroxidase antibodies, and TSH receptor antibodies.
Schirmer test: Useful for evaluating concomitant aqueous tear-deficient dry eye.
Autoimmune tests: Consider anti-SS-A and anti-SS-B antibodies if Sjögren’s syndrome or rheumatoid arthritis is suspected.
In Sjögren’s syndrome, severe bulbar conjunctival epithelial damage is observed, but unlike SLK, it is often not accompanied by limbal thickening or hyperemia. CL-SLK is an SLK-like lesion that occurs in CL wearers. In addition, differentiation from allergic conjunctivitis, thyroid eye disease, floppy eyelid syndrome, lid-wiper epitheliopathy (LWE), and trachoma is necessary. Also note that after blepharoptosis surgery, SLK-like lesions can occur due to increased eyelid pressure.
In the Japanese dry eye clinical practice guidelines, SLK, along with lid-wiper epitheliopathy, filamentary keratitis, and conjunctivochalasis, is classified as a dry eye-related disease belonging to the core mechanism ② of “increased friction during blinking” 5).
QWhat is the most important point in diagnosing SLK?
A
The most important thing is to fully evert the upper eyelid and observe the superior bulbar conjunctiva. Because SLK lesions are localized superiorly, they are easily missed without eversion. Confirm epithelial damage of the superior bulbar conjunctiva with fluorescein staining (using a blue-free filter) or lissamine green/rose bengal staining.
Mild cases: Preservative-free artificial tears (Soft Santear ophthalmic solution 6 times/day) and sodium hyaluronate ophthalmic solution (Hyalein 0.1% 6 times/day) are used alone or in combination, and if necessary, low-potency steroids (fluorometholone 0.1% 2 times/day) are added.
Mild to moderate cases: Diquafosol sodium ophthalmic solution (Diquas 3%, 6 times/day) or rebamipide ophthalmic solution (Mucosta UD 2%, 4 times/day) is the mainstay. Rebamipide’s friction-reducing and mucosal repair effects are effective.
Severe cases: Rebamipide or diquafosol is combined with fluorometholone. If inflammation is severe, switch to betamethasone ophthalmic solution (Rinderon PF 0.1%, 1-2 times/day). When using steroid eye drops, be aware of increased intraocular pressure (steroid responder).
Cases with filamentary keratitis: Diquafosol eye drops may increase corneal filaments, so rebamipide is preferred. Corneal filaments are mechanically removed with forceps or a cotton swab after topical anesthesia.
Cyclosporine eye drops: Long-term follow-up studies have shown that topical cyclosporine reduces ocular surface inflammation in SLK and improves symptoms and clinical findings 6). Although not covered by insurance in Japan, it is an option for refractory cases.
In cases with concomitant aqueous tear-deficient dry eye, insertion of upper and lower punctal plugs is effective. If there is no tear deficiency, patients may complain of tearing, so it is recommended to insert only the upper punctal plug2).
Therapeutic soft contact lenses (bandage contact lenses: BCL) mechanically reduce friction on the superior limbus during blinking 9). Since Mondino et al. reported the combined use of pressure patching and soft CL in 1982, this has been positioned as a representative treatment for friction reduction 9).
Autologous serum eye drops (50% dilution) supply nutritional factors such as vitamin A, epidermal growth factor (EGF), TGF-β, insulin-like growth factor, and substance P, maintaining proliferation and differentiation of the ocular surface epithelium. Tsubota et al. reported efficacy for severe dry eye7), and Goto et al. demonstrated the effectiveness of autologous serum eye drops for SLK 8). The 50% concentration is a practical concentration that avoids excessive action of TGF-β, which has antiproliferative effects, while achieving sufficient repair effects compared to 100% dilution 12).
In recent years, there has been a case report of combined therapy with BCL and 50% autologous serum eye drops leading to two-year remission in refractory SLK complicated by dry eye and MGD10). In this case, a silicone hydrogel CL was worn for 6–8 hours during the day, and autologous serum eye drops were used at home six or more times daily.
If improvement is not achieved with the above conservative treatments, and there is superior bulbar conjunctival laxity, surgery for superior conjunctivochalasis (conjunctival resection) is indicated. This procedure involves removal of the subconjunctival Tenon’s capsule in the affected area and resection of the loose conjunctiva, aiming for inflammatory adhesion between the bulbar conjunctiva and sclera. Postoperative recurrence is rare, and long-term prognosis is good 2).
In young patients or those with glaucoma who may require filtration surgery in the future, the indication for surgery should be carefully determined. Elderly patients with superior conjunctival laxity and no glaucoma are good candidates.
Management of Cases Complicated by Thyroid Disease
If thyroid dysfunction is present, concurrent medical treatment by an internist should be performed. SLK symptoms often improve with control of thyroid function.
QCan SLK be cured?
A
SLK is a chronic disease that alternates between remission and exacerbation, but its frequency tends to decrease with age. The disease duration is said to be 1–10 years. Because it involves intense conjunctival inflammation, it may eventually lead to natural remission due to inflammatory scar formation. Surgery for superior conjunctivochalasis provides tight adhesion between the conjunctiva and sclera, resulting in no postoperative recurrence and good long-term prognosis.
Relaxation of the superior bulbar conjunctiva causes mechanical friction between the inner surface of the upper eyelid and the superior bulbar conjunctiva/limbus during blinking. This friction induces inflammation, leading to epithelial hyperproliferation and differentiation disorder. Differentiation disorder causes squamous metaplasia and a decrease in goblet cells. The decrease in goblet cells thins the mucin layer on the ocular surface, further enhancing friction. Thus, a vicious cycle is formed 4).
The Japanese dry eye diagnostic guidelines define “decreased stability of the tear film during eyelid opening maintenance” and “increased friction during blinking” as the two core mechanisms of dry eye. SLK, along with lid-wiper epitheliopathy, filamentary keratitis, and conjunctivochalasis, is considered a representative disease directly involved in increased friction, and increased friction in Kessing space (the microspace between the palpebral and bulbar conjunctiva) is positioned as the core of the pathology 5).
The following molecular changes have been reported in SLK-affected conjunctiva.
Epithelial keratinization: Increased expression of cytokeratins 10, 13, and 14 and increased expression of proliferating cell nuclear antigen (PCNA) have been observed, indicating abnormal differentiation and excessive proliferation of the conjunctival epithelium.
Increased expression of TGF-β2, tenascin, and integrin β1: In a Japanese study by Matsuda et al., the expression of these factors induced by mechanical trauma was elevated in SLK-affected conjunctiva, supporting the microtrauma theory as the origin of SLK at the molecular level 11).
Decrease in mucin-like glycoproteins: Levels of mucin-like glycoproteins are reduced in the keratinized superior bulbar conjunctival epithelium. These levels normalize after treatment with vitamin A eye drops or bandage contact lenses.
Keratinization of epithelial cells, dyskeratosis, acanthosis, and balloon-like degeneration of nuclei are observed. Infiltration of polymorphonuclear leukocytes, plasma cells, mast cells, and lymphocytes is seen in the stroma. Impression cytology shows a characteristic snake-like appearance of nuclear chromatin condensation in bulbar conjunctival epithelial cells, and in the palpebral conjunctiva, loss of goblet cells and an increase in inflammatory cells are observed.
QWhy does SLK only cause lesions in the superior region?
A
The upper eyelid exerts stronger pressure on the eyeball than the lower eyelid. Furthermore, if there is relaxation of the superior bulbar conjunctiva, significant friction occurs between the inner surface of the upper eyelid and the relaxed conjunctiva with each blink. In cases of exophthalmos due to hyperthyroidism, this friction is further enhanced. This induces chronic inflammation localized to the superior region.
In recent SLK treatment research, combination therapy that reduces friction and restores the ocular surface has attracted attention. A comprehensive review published by Lahoti et al. in 2022 organized the latest findings on the pathology, diagnosis, and treatment of SLK, systematically reviewing non-surgical therapies (artificial tears, vitamin A, cyclosporine, lifitegrast, autologous serum, therapeutic contact lenses) and surgical therapies (conjunctival resection, cauterization, cryotherapy) 2).
Regarding autologous serum eye drops, a prospective study by Semeraro et al. showed that 50% dilution is effective for various ocular surface diseases 12). In addition, Noor et al. reported a case of refractory SLK in which a combination of BCL and 50% autologous serum eye drops, along with MGD treatment using scleral IPL (intense pulsed light) therapy, achieved remission for two years 10).
In studies targeting the Japanese population, Kawashima and Yamada et al. showed that complications of MGD and friction-related diseases directly exacerbate dry eye severity, emphasizing the importance of early detection and intervention for friction-related diseases including SLK 3).
In the future, in addition to rebamipide and diquafosol, which are widely used as dry eye treatments, cyclosporine eye drops 6), autologous serum eye drops, and BCL combination therapy are likely to become standard options for refractory cases. Moreover, the approach of viewing SLK within a unified framework of friction-related ocular surface diseases is consistent with the thinking of Japanese dry eye clinical practice guidelines 5) and is expected to be emphasized in future guideline revisions.
Theodore FH. Superior limbic keratoconjunctivitis. Eye Ear Nose Throat Mon. 1963;42:25-28. PMID:13980870.
Lahoti S, Weiss M, Johnson DA, Kheirkhah A. Superior limbic keratoconjunctivitis: a comprehensive review. Surv Ophthalmol. 2022;67(2):331-341. doi:10.1016/j.survophthal.2021.05.009
Vu CHV, Kawashima M, Yamada M, et al. Influence of meibomian gland dysfunction and friction-related disease on the severity of dry eye. Ophthalmology. 2018;125(8):1181-1188. doi:10.1016/j.ophtha.2018.01.025
Cher I. Superior limbic keratoconjunctivitis: multifactorial mechanical pathogenesis. Clin Experiment Ophthalmol. 2000;28(3):181-184. doi:10.1046/j.1442-9071.2000.00284.x
Sahin A, Bozkurt B, Irkec M. Topical cyclosporine A in the treatment of superior limbic keratoconjunctivitis: a long-term follow-up. Cornea. 2008;27(2):193-195. doi:10.1097/ICO.0b013e318033bd25
Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjögren’s syndrome. Br J Ophthalmol. 1999;83(4):390-395. doi:10.1136/bjo.83.4.390
Goto E, Shimmura S, Shimazaki J, Tsubota K. Treatment of superior limbic keratoconjunctivitis by application of autologous serum. Cornea. 2001;20(8):807-810. doi:10.1097/00003226-200111000-00006
Mondino BJ, Zaidman GW, Salamon SW. Use of pressure patching and soft contact lenses in superior limbic keratoconjunctivitis. Arch Ophthalmol. 1982;100(12):1932-1934. doi:10.1001/archopht.1982.01030040912008.
Noor NA. Combination of bandage contact lens and autologous serum eye drop for the treatment of superior limbic keratoconjunctivitis. Clin Optom. 2023;15:75-80. doi:10.2147/OPTO.S404164
Matsuda A, Tagawa Y, Matsuda H. TGF-beta2, tenascin, and integrin beta1 expression in superior limbic keratoconjunctivitis. Jpn J Ophthalmol. 1999;43(4):251-256. doi:10.1016/S0021-5155(99)00021-0. PMID:10482468.
Semeraro F, Forbice E, Braga O, et al. Evaluation of the efficacy of 50% autologous serum eye drops in different ocular surface pathologies. Biomed Res Int. 2014;2014:826970. doi:10.1155/2014/826970
Nelson JD. Superior limbic keratoconjunctivitis (SLK). Eye (Lond). 1989;3(2):180-189. doi:10.1038/eye.1989.26
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.