Symblepharon is a condition in which the bulbar conjunctiva and palpebral conjunctiva form abnormal adhesions to each other. It was first described by Fuchs in 1892 1). Most cases are acquired, but congenital cases associated with cryptophthalmos have also been reported.
The causes are diverse. Persistent epithelial defects of the bulbar and palpebral conjunctiva, combined with an inflammatory response, lead to adhesion formation. Representative causative diseases are shown below.
Chemical trauma is one of the most common causes, with symblepharon occurring in up to 18% of severe ocular surface burns 3). Severe ocular complications after Stevens-Johnson syndrome/toxic epidermal necrolysis are seen in 4–11.1% of cases, and symblepharon develops as a chronic complication 1). In ocular cicatricial pemphigoid, chronic conjunctivitis persists due to autoimmune mechanisms, and symblepharon gradually progresses. In the staging of this disease, stage III corresponds to symblepharon.
QWhat is the difference between symblepharon and ankyloblepharon?
A
Ankyloblepharon is a condition where the upper and lower eyelids adhere to each other along the lid margin, and includes congenital ankyloblepharon filiforme adnatum and acquired forms due to trauma or inflammation. In contrast, symblepharon is adhesion between the bulbar and palpebral conjunctiva, and these are anatomically distinct conditions. However, severe symblepharon can secondarily lead to ankyloblepharon.
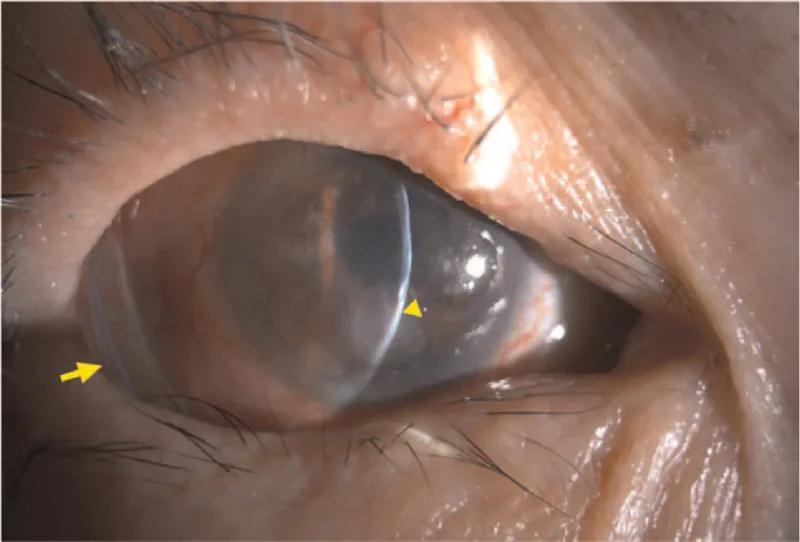
Hwang S, Kuo S. Corneal perforation in ocular cicatricial pemphigoid: A CARE-compliant case report. Medicine. 2021 Dec 23; 100(51):e28266. Figure 2. PMCID: PMC8702268. License: CC BY.
Anterior segment image showing adhesion between the palpebral and bulbar conjunctiva, with a shallow and shortened fornix. The conjunctival band adhesion restricts ocular motility.
Shortening or loss of the conjunctival fornix: The fornix becomes shallow due to adhesions between the palpebral and bulbar conjunctiva. Tear storage decreases and blinking function is impaired.
Ocular motility restriction: Mechanical restriction due to adhesions limits extraocular muscle movement. This may cause double vision.
Cicatricial entropion: Scar contraction of the palpebral conjunctiva causes the eyelashes to contact the ocular surface.
Extension of adhesions onto the cornea: Conjunctival tissue crosses the limbus and invades the cornea, obstructing the visual axis.
Keratization of the ocular surface: Chronic dryness due to fornix loss leads to keratinization.
The severity of symblepharon is sometimes classified using the Kheirkhah classification 4). It ranges from Grade I (linear adhesion between palpebral and bulbar conjunctiva) to Grade IV (complete obliteration of the fornix). In severe cases after SJS, it can reach Grade IVc3+ 1).
Symblepharon occurs secondary to conditions that cause extensive damage to the conjunctival epithelium.
Chemical trauma: Alkali agents are lipophilic and penetrate deep into tissues, often causing more severe damage than acids 2). Firework-related chemical trauma can also be a cause 4).
Stevens-Johnson syndrome/toxic epidermal necrolysis: Chronic inflammation following pseudomembrane formation in the acute phase leads to progression of symblepharon 1). Chronic ocular abnormalities persist in 30–50% of patients after SJS1).
Ocular cicatricial pemphigoid: Scarring changes in the conjunctiva progress through stages I to IV, with symblepharon occurring at stage III.
Chronic graft-versus-host disease (GVHD): Chronic pseudomembranous conjunctivitis after bone marrow transplantation can lead to symblepharon.
Trachoma: Scarring of the conjunctiva due to chronic conjunctivitis can cause symblepharon.
Surgical trauma: Recurrent pseudopterygium after pterygium surgery, or after glaucoma surgery, can also occur.
Young age, presence of autoimmune disease, and history of ocular surgery are risk factors for recurrence 3).
QHow can symblepharon after chemical trauma be prevented?
A
Thorough irrigation and anti-inflammatory treatment in the acute phase are fundamental. Frequent application of antibiotic eye ointment (4 times a day) maintains lubrication between conjunctival surfaces, and steroid eye drops and oral steroids suppress inflammation. If there is extensive conjunctival epithelial defect, early amniotic membrane transplantation is performed, and therapeutic contact lenses or conformers are used to prevent adhesion formation.
Slit-lamp microscopy: It is easy to miss with forward gaze alone; the key to diagnosis is to observe at low magnification with upward and downward gaze. Assess fornix shortening or loss, conjunctival scarring, and progression of adhesion onto the cornea.
Ocular motility test: Evaluate the degree of mechanical restriction due to adhesion. Use the Hess screen test (Hess red-green test) to quantitatively assess eye movements.
Systemic Examination
Differential diagnosis of causative diseases: Stevens-Johnson syndrome/toxic epidermal necrolysis and chemical trauma are determined from medical history. In middle-aged or older women with no history of trauma or surgery and bilateral chronic conjunctivitis with symblepharon, ocular pemphigoid should be considered first.
Autoimmune testing: If ocular pemphigoid is suspected, consider conjunctival biopsy with immunohistochemistry.
Symblepharon is a clinical finding, and differentiation of its underlying disease is important. Pseudopterygium involves conjunctival tissue invading the cornea during the healing process of corneal trauma or peripheral corneal ulcer, but its pathophysiology differs from symblepharon. Differentiation between ocular cicatricial pemphigoid and pseudopemphigoid is based on the presence of systemic symptoms and a history of long-term use of antiglaucoma eye drops.
For prevention of symblepharon in the acute phase, apply antibiotic ophthalmic ointment four times daily to maintain lubrication between conjunctival surfaces. Combine with steroid eye drops (0.1% fluorometholone or 0.1% betamethasone) to suppress inflammation. For extensive conjunctival epithelial defects, use therapeutic soft contact lenses or conformers. Manage dry eye symptoms with frequent artificial tear instillation.
In ocular cicatricial pemphigoid, systemic immunosuppressants (cyclosporine, cyclophosphamide) or oral steroids are needed to control the underlying disease. Performing surgery without controlling inflammation leads to rapid progression of adhesion and keratinization postoperatively.
Surgery is indicated when symblepharon causes eyelid fissure deformity, ocular motility restriction, or visual impairment. The basic procedure involves dissection and removal of the adhesive tissue, followed by tissue transplantation to the exposed scleral surface.
Amniotic Membrane Transplantation
Indications: Mild to moderate symblepharon. In fornix reconstruction, it promotes epithelial cell migration, adhesion, and differentiation, and has anti-inflammatory and anti-fibrotic effects2).
Limitations: In severe cases, residual conjunctival epithelial cells are insufficient, and recurrence rates are high (6–40%)4). In Case 2, 7 recurrences occurred over 8 years after amniotic membrane transplantation3).
Oral Mucosal Transplantation
Indications: Severe symblepharon. Easy to harvest and provides sufficient tissue volume. Contains goblet cells, improving tear film through mucin secretion4).
Outcomes: Oral mucosal autograft sutured to the sclera in 7 eyes showed no recurrence for 3 years4). In Case 1 before KPro, no recurrence for 2 years after OMAU3).
Martinez-Osorio et al. (2021) performed oral mucosal autograft (OMAU) sutured to the sclera in 7 eyes with severe symblepharon. Complete graft take and anatomical fornix restoration were achieved in all cases, with no recurrence during 3-year follow-up4).
Kate et al. (2022) reported that in managing symblepharon before KPro, the case using OMAU (Case 1) had no recurrence for 2 years, while the case using amniotic membrane transplantation (Case 2) had 7 recurrences over 8 years. Oral mucosa has the advantage of not depending on the contralateral conjunctiva even in bilateral disease3).
Other surgical techniques include Z-plasty and conjunctival sac reconstruction using conjunctival grafts from the contralateral eye. However, if the lacrimal gland and conjunctiva are severely damaged and there is no tear secretion, mucosal grafts are often ineffective.
Lam et al. (2023) used a large (5 cm × 10 cm) externally sutured amniotic membrane and a custom symblepharon ring (made from an intravenous infusion tube) in a 35-year-old man after alkali injury. Four months postoperatively, the corneal epithelial defect resolved and visual acuity improved to 20/25 2).
Venugopal et al. (2022) reported a technique for Grade 4 chemical injury-induced symblepharon, involving symblepharon lysis and amniotic membrane transplantation combined with placement of a Gore-Tex sheet in the fornix. Gore-Tex acts as a physical barrier to prevent recurrence of adhesions 5).
QWhy is oral mucosal graft superior to amniotic membrane transplantation in symblepharon surgery?
A
Amniotic membrane transplantation is an excellent substrate that promotes epithelial cell migration, but in severe cases, residual conjunctival epithelial cells are insufficient, leading to incomplete epithelialization and a high recurrence rate. Oral mucosal grafts directly transplant an epithelial layer, covering the exposed sclera with epithelium equivalent to conjunctiva. They also contribute to mucin secretion as they contain goblet cells. Additionally, even in bilateral disease, a sufficient amount can be harvested from the lower lip 3)4).
Symblepharon results from abnormal wound healing after extensive conjunctival epithelial damage. When epithelial cells are lost from both the bulbar and palpebral conjunctiva, exposed connective tissues come into contact and form fibrous adhesions. Inflammatory response is essential in this process, and inflammatory cell infiltration and fibroblast activation promote adhesion maturation.
Upregulation of TGF-β signaling is observed in adhesion tissue, promoting subconjunctival fibroblast response 3). Myofibroblasts are present in the adhesion area and contribute to scar tissue contraction 4). Therefore, even if adhesions are surgically released, recurrence is likely due to residual fibrotic tendency.
To prevent recurrence after surgery, it is important to sufficiently excise scar tissue and Tenon’s capsule to expose the sclera, and to cover the area completely with oral mucosal or conjunctival grafts 4). Preoperative steroid administration for three months and postoperative steroid therapy also improve prognosis 4).
QWhy do symblephara tend to recur?
A
If adequate epithelialization of the exposed scleral surface after adhesion release is not achieved, the connective tissues of the bulbar and palpebral conjunctiva come into contact again, leading to reformation of adhesions. Upregulation of TGF-β signaling enhances fibroblast response, and myofibroblast-mediated scar contraction promotes recurrence 3)4). In severe cases, conjunctival epithelial stem cells are also reduced, making spontaneous epithelial regeneration difficult.
In the surgical treatment of symblepharon, the selection of graft tissue and recurrence prevention strategies are the focus of research.
Martinez-Osorio et al. (2021) achieved anatomical success in all 7 eyes using a technique of direct suturing of oral mucosal autograft to the sclera, with no recurrence during 36–44 months of follow-up 4). OMAU is an old technique previously used for recurrent pterygium, but its utility has been re-evaluated in recent years.
Kate et al. (2022) reported a staged approach before KPro, showing that OMAU had superior long-term outcomes compared to amniotic membrane transplantation3). In severe cases with limbal stem cell deficiency, a staged strategy of symblepharon release → ocular surface stabilization → KPro or limbal transplantation is recommended.
Venugopal et al. (2022) reported a novel technique of placing a Gore-tex sheet in the fornix 5). Gore-tex acts as a physical barrier to prevent postoperative conjunctival re-adhesion and has been used for pterygium recurrence prevention.
Regenerative medicine approaches such as cultured limbal stem cell transplantation and cultured oral mucosal epithelial sheet transplantation are also expected to be applied in severe cases.
Wibowo E, Maharani RV, Sutikno NA. Symblepharon as Ocular Manifestation Post Stevens-Johnson Syndrome: A Rare Case. Romanian journal of ophthalmology. 2024;68(4):466-469. doi:10.22336/rjo.2024.84. PMID:39936062; PMCID:PMC11809831.
Lam SS, Sklar BA, Schoen M, Rapuano CJ. Severe ocular alkali injury managed with an externally sutured amniotic membrane and customized symblepharon ring. Taiwan journal of ophthalmology. 2023;13(1):101-105. doi:10.4103/2211-5056.362597. PMID:37252174; PMCID:PMC10220433.
Kate A, Doctor MB, Shanbhag SS. Management of Symblepharon Prior to Keratoprosthesis in Chronic Ocular Burns: A Sequential Approach. Cureus. 2022;14(4):e24611.
Martinez-Osorio H, Schellini SA, Marin-Muñoz LS. Long-term follow up of oral mucosa autograft sutured to the sclera in severe symblepharon. Am J Ophthalmol Case Rep. 2021;23:101099.
Venugopal A, Ravindran M. Gore-tex a magic sheet for symblepharon prevention! Indian J Ophthalmol. 2022. DOI:10.4103/ijo.IJO_515_22.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.