Contact lens (CL) complications are a general term for corneal and conjunctival disorders caused or triggered by CL wear. The severity ranges from asymptomatic minor findings to severe cases such as corneal ulcers.
The main mechanisms by which CLs induce ocular disorders can be broadly classified into the following five categories.
Mechanical trauma: Epithelial damage due to irregularities of the lens edge or inner lens surface
Reduced corneal oxygen supply: Hypoxia due to low Dk/t lens wear or extended wear
Lubrication insufficiency: Localized dryness due to changes in tear film dynamics
Immune and allergic reactions: Response to lens deposits and bacterial endotoxins
Microbial infection: Infection associated with poor lens care and lens case contamination
In the examination of CL complications, it is important to infer the cause from corneal findings and eliminate that cause. Explain the cause, healing period, presence of sequelae, and necessity of CL change individually, and provide appropriate treatment.
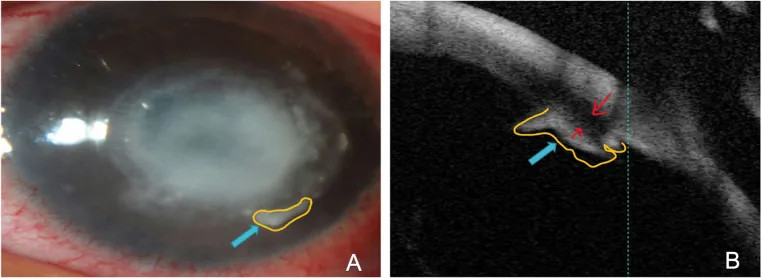
Alreshidi SO, et al. Differentiation of acanthamoeba keratitis from other non-acanthamoeba keratitis: Risk factors and clinical features. PLoS One. 2024. Figure 4. PMCID: PMC10931457. License: CC BY.
Slit-lamp photograph (A) showing well-defined retrocorneal plaque-like deposits associated with Acanthamoeba keratitis, and AS-OCT image (B) showing dense retrocorneal plaque-like deposits associated with fungal keratitis. These correspond to the corneal infiltrates discussed in the section “2. Main symptoms and clinical findings”.
The main subjective symptoms of CL complications are as follows.
Foreign body sensation/discomfort: Caused by epithelial damage or lens incompatibility. Most frequent.
Hyperemia: Caused by dilation of conjunctival vessels. Often associated with corneal infiltration or edema.
Ocular pain: Occurs with corneal erosion or infectious keratitis. Acute epithelial edema causes severe vision loss and ocular pain.
Tearing, blurred vision, visual loss: Appears depending on the severity of epithelial damage.
CL intolerance: Perceived as worsening wearing comfort or lens displacement.
Particular caution is required when hyperemia, discharge, and pain occur together, as this may indicate corneal infection.
All CLs reduce corneal sensitivity (hypoesthesia). Due to this reduced sensitivity, CL wearers may have difficulty noticing early symptoms of corneal damage.
Location: Limited to the 3 and 9 o’clock positions at the corneal limbus
Cause: During blinking, the HCL moves approximately 2 mm vertically, causing localized dryness as tears are drawn in from the 3 and 9 o’clock directions
Course: Mild cases heal in 3–5 days. Progression to erosion requires about 1 week and may leave corneal opacity
Smile-mark superficial punctate keratopathy (SCL)
Location: Lower pupillary area (corresponding to the shape of a smiling mouth)
Cause: Occurs in patients with pre-existing dry eye due to reduced tear fluid under the lens
Course: Managed with dry-eye eye drops. Advise early removal from the evening onward
Peripheral corneal infiltration: Inflammatory cells infiltrate due to epithelial damage caused by foreign bodies under the CL. Heals in about 1 week with antibiotics and low-concentration steroid eye drops.
Marginal corneal infiltration: Appears at multiple sites along the limbus. Caused by biofilm contamination of the lens case or pigment exposure from colored CLs.
SEALs (superior epithelial arcuate lesions): Arcuate confluent superficial punctate keratopathy in the 11 to 1 o’clock peripheral cornea. Caused by mechanical irritation from the inner surface of the CL. Distinguished from superior limbic keratoconjunctivitis by the absence of conjunctival staining.
Acute epithelial edema: Epithelial edema of the entire cornea, most pronounced centrally. Also called overwear syndrome.
Corneal erosion: A condition in which superficial punctate keratopathy worsens and the full epithelial layer is lost. All causes of superficial punctate keratopathy can lead to corneal erosion.
Giant papillary conjunctivitis (GPC): Giant papillae are observed upon upper eyelid eversion. Previously more common with conventional SCLs, but also seen with silicone hydrogel lenses in recent years.
QWhat should you do if pain occurs while wearing contact lenses?
A
First, remove the CL immediately. If pain is mild and there is no vision loss, you may discontinue wear and observe until the next day. However, if accompanied by redness, discharge, or severe pain, infectious keratitis is possible, so promptly visit an ophthalmologist. Do not discard the removed CL—bring it to your appointment to help identify the cause.
HCL (RGP-CL): Characteristic 3-and-9-o’clock staining occurs due to movement during blinking. Lens edge impressions and pseudo-dendritic keratitis may occur when the lens is bound.
SCL: Materials with low oxygen permeability (HEMA) and continuous wear readily lead to corneal hypoxia. In cases complicated by dry eye, smile-mark punctate keratopathy may be observed.
Silicone hydrogel (SiHy) lenses: These have high oxygen permeability but may cause SEALs due to the stiffness of the material. Donut-shaped punctate keratopathy has been reported due to incompatibility with PHMB disinfecting solutions.
Cosmetic CLs: In products where pigment is exposed on the corneal side, donut-shaped punctate keratopathy and corneal infiltration may occur at the pigmented area.
Lens case contamination: If not replaced for 3 months or longer, biofilms form and cause marginal corneal infiltration.
Allergy to care solutions: MPS (multipurpose solution) may cause corneal epithelial damage.
Forgotten neutralization: Forgetting to neutralize the disinfecting solution may cause mild chemical injury.
Overnight wear: Nighttime wear is a major risk factor for microbial keratitis1). Educating CL users and providing instruction on proper lens care help reduce infection risk1).
Contact lens wear is one of the greatest risk factors for microbial keratitis. Causative organisms include Pseudomonas aeruginosa, Staphylococcus, Streptococcus, and Serratia. It has been reported that 88% of patients with Acanthamoeba keratitis (AK) were contact lens wearers.
QDo daily disposable lenses have fewer complications?
A
Daily disposable lenses require no lens care, eliminating the risk of case contamination and minimizing protein buildup, making giant papillary conjunctivitis and care-solution-related complications unlikely. However, dry-eye-related smile-mark punctate keratopathy and complications from overnight wear can still occur with daily disposable lenses.
Slit-lamp microscopy is essential for diagnosing CL-related corneal disorders. In HCL wearers, a key point is to observe the lens surface for deposits and wettability before staining with fluorescein. Deposits become visible as the lens surface dries.
Total corneal epithelial damage: Consider drug toxicity, severe dry eye, and overnight wear.
Acute epithelial edema can be misdiagnosed as a full-thickness epithelial defect. Even without epithelial defects, tight junctions can weaken and allow fluorescein penetration, causing the entire cornea to appear stained 10 minutes after application.
In the differential diagnosis between SEALs and superior limbic keratoconjunctivitis (SLK), SLK differs in that the conjunctival epithelium also stains with fluorescein. Pseudodendritic keratitis is seen with HCL binding and resembles the dendritic ulcer of herpes keratitis in that the ends of linear lesions branch into two or more branches.
Discontinuation of CL wear and removal of the cause are the basics. Based on the corneal findings, the cause is inferred, and the healing period, presence or absence of sequelae, and necessity of CL change are explained individually.
Superficial punctate keratopathy: Heals in 3 to 5 days with CL discontinuation and eye drops. In refractory superficial punctate keratopathy, tear film break-up may be involved.
Corneal erosion: Epithelial repair takes about one week and may leave corneal opacity. Antibiotic eye drops and hyaluronic acid eye drops are prescribed.
CL-related corneal abrasion: The use of eye patches or therapeutic CLs is not recommended due to concerns about secondary infection risk1).
After healing, CL change according to the cause is performed. Changing to SCL for 3-and-9 o’clock staining, selecting a safe SCL for SEALs, and changing to a silicone hydrogel lens with excellent water retention for smile-mark superficial punctate keratopathy are effective.
Treatment consists of discontinuing CL wear and using antibiotic + low-concentration steroid (0.1% fluorometholone) eye drops. Steroid use is desirable because infiltrative lesions may remain as opacity, but if poor compliance is anticipated, NSAID eye drops are used to monitor the course.
Indications: Small non-central ulcer with infiltration ≤2 mm and ≥3 mm from the visual axis
Treatment: Empiric therapy with fluoroquinolone eye drops
Visual Threat
Indications: Infiltration >2 mm, <3 mm from the visual axis, or worsening after 48 hours of treatment
Treatment: Perform corneal culture + Gram stain, initiate vancomycin + fortified tobramycin eye drops every hour. Adjust medication based on culture results.
Immediate discontinuation of contact lenses is mandatory. Common causative organisms include Pseudomonas aeruginosa and Staphylococcus species. For Acanthamoeba keratitis, combination therapy with polyhexamethylene biguanide, propamidine isethionate, and other agents is used.
The mainstay is discontinuation of contact lens use or switching to daily disposables. Use 0.1% fluorometholone 4 times daily for 1–2 weeks. Even after symptom improvement, returning to the original lens often leads to recurrence; changing the lens type is recommended.
When using BCL for pain relief in microcystic and bullous corneal epitheliopathy, thin lenses with high water content and high Dk value are considered safe2). Concomitant use of prophylactic broad-spectrum antibiotics is recommended to prevent secondary infection2). BCL does not provide a long-term solution for corneal edema2).
QAre silicone hydrogel lenses safe?
A
Silicone hydrogel lenses have dramatically improved oxygen permeability compared to conventional HEMA lenses, significantly reducing hypoxia-related complications. However, due to the stiffness of the material, SEALs may occur, and incompatibility with certain care solutions has been reported to cause donut-shaped superficial punctate keratopathy. Proper care and regular check-ups are important for any CL.
CLs limit the supply of atmospheric oxygen to the cornea. Lenses with low oxygen permeability (Dk/t) increase anaerobic metabolism in the corneal epithelium, leading to epithelial edema from osmotic pressure elevation due to lactate accumulation. In the era of PMMA lenses, epithelial edema localized to the central cornea, known as central circular clouding, was commonly observed.
Conventional HEMA-based SCLs, which were mainstream until around 1990, frequently caused acute epithelial edema due to oxygen deficiency. However, high-Dk silicone hydrogel lenses are now mainstream, and hypoxic complications have decreased.
Friction between the contact lens and the ocular surface during blinking causes epithelial damage. With HCL, the lens moves approximately 2 mm vertically with each blink, drawing tear fluid from the 3 o’clock and 9 o’clock directions. This depletes tears in those areas, leading to superficial punctate keratopathy. When mechanical stimulation from the lens edge is added, it can progress to corneal erosion and corneal infiltration.
With SCL, friction between the upper eyelid and the CL surface can cause lid-wiper epitheliopathy (LWE) and SEALs. SEALs occur at the site where the upper eyelid presses against the CL and are particularly likely when the corneal side surface of the lens is irregular.
Chronic mechanical stimulation and bacterial endotoxins from CL wear trigger an immune response, leading to sterile infiltrates. This is often caused by inadequately disinfected SCLs or biofilms inside the lens case.
Giant papillary conjunctivitis involves a type I allergic reaction to proteins deposited on the CL surface. Constant contact and stimulation of the upper tarsal conjunctiva by the lens leads to inflammation and formation of giant papillae.
Biofilm formation inside the lens case is an important risk factor for infectious keratitis. Bacteria within biofilms have high resistance to disinfectants, making regular replacement of the lens case essential for prevention.