Acanthamoeba keratitis (AK) is a corneal infection caused by Acanthamoeba, a free-living amoeba widely found in soil, freshwater, and tap water. It was first reported by Nagington et al. in 1973–74, and the first case in Japan was reported by Ishibashi et al. in 1988. Initially, it was an extremely rare disease except for trauma-related cases, but since the 2000s, the number of cases has increased with the widespread use of contact lenses (CLs), and it is now a globally important issue, particularly among CL users10).
The primary causative species are Acanthamoeba castellanii and A. polyphaga, and among genotypes, the T4 type accounts for 94.3% of all cases4). Acanthamoeba has two forms—trophozoite and cyst—and when growth conditions deteriorate, it encysts and becomes resistant to various drug treatments10). Acanthamoeba keratitis accounts for approximately 1.5% of all microbial keratitis cases, with an estimated incidence of about 2.3 eyes per million people. According to 2015 data from the UK and the Netherlands, the annual incidence is reported to be approximately 0.31–0.48 per 10,000 CL users, with about half of those cases resulting in visual impairment1).
Acanthamoeba keratitis is one of the leading causes of severe contact lens-related keratitis, with 85–90% of patients being CL wearers. In a Japanese survey of severe corneal infections among CL wearers, acanthamoeba keratitis was reported as the second most common after Pseudomonas aeruginosa corneal ulcer. Delayed treatment can lead to corneal perforation or blindness, and this disease can cause irreversible visual impairment in young, healthy, socially active individuals.
A case-control study by Carnt et al. (2023) showed that the use of reusable daily care lenses was associated with an approximately 3.8-fold higher risk of developing acanthamoeba keratitis compared to daily disposable lenses (OR 3.84; 95% CI 1.75–8.43)1). The frequency of severe inflammatory complications was also high; in a cohort of 194 cases by Carnt et al. (2018), scleritis was observed in approximately 20% and stromal ring infiltrates in approximately 15%, with poor outcomes including final visual acuity ≤0.1, perforation, and corneal transplantation reaching 48% of all cases2). As a severe corneal infection in contact lens users, this poses a public health challenge.
QCan it develop even without using contact lenses?
A
CL wearers account for the majority, but it can also develop in non-CL wearers following trauma or exposure to contaminated water. In India and other regions, trauma-related cases are common11).
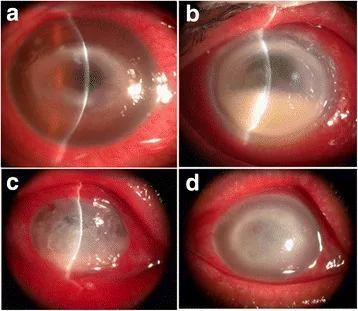
Zhong J, et al. Associated factors, diagnosis and management of Acanthamoeba keratitis in a referral Center in Southern China. BMC Ophthalmol. 2017. Figure 1. PMCID: PMC5625641. License: CC BY.
Four slit-lamp photographs showing gray-white stromal infiltration and opacity in the cornea. The ring-shaped infiltration characteristic of Acanthamoeba keratitis is visible especially in the upper row, making these images suitable for explaining the main clinical findings.
The most characteristic symptom of Acanthamoeba keratitis is severe eye pain disproportionate to the clinical findings. Since patients complain of intense pain even when the lesion is very mild, this disease should not be ruled out even if corneal findings at the time of examination are minimal.
Eye pain: Initially remains limited to mild foreign body sensation, but gradually changes to severe pain. Invasion of corneal nerves (radial keratoneuritis) is thought to be the cause of the pain.
Hyperemia: Accompanied by severe ciliary injection, observed from the early stage.
Lacrimation and eyelid swelling: Severe lacrimation occurs along with intense pain, often accompanied by eyelid swelling. Discharge is rarely reported.
Vision loss: Becomes pronounced as the lesion extends to the central cornea. Opacities involving the pupillary area often reduce visual acuity to 0.1 or worse.
The progression of symptoms is insidious, often taking several weeks to 1–2 months from onset to the fully developed stage. However, pain is relatively noticeable from an early stage, and patients often find it unbearable, leading to repeated visits to the clinic. In a report by Carnt et al. (2018), the median duration of symptoms exceeded 37 days in cases with poor prognosis, and this disease should always be suspected in CL wearers with prolonged pain and keratitis2).
Clinical Findings (Findings Confirmed by Physician Examination)
Acanthamoeba keratitis progresses insidiously and presents characteristic clinical findings depending on the disease stage. Based on corneal findings, it is classified into three stages: early, transitional, and advanced. The Infectious Keratitis Treatment Guidelines, 3rd Edition, also clearly describe the most characteristic findings of the “early” and “advanced” stages10).
Early Stage
Radial keratoneuritis: Linear infiltration along the nerves from the limbus toward the central cornea. This is a highly specific finding for Acanthamoeba keratitis.
Epithelial/subepithelial infiltration: Punctate, patchy, and linear opacities cluster together.
Pseudodendritic lesions: Irregular, jagged linear lesions with frayed edges are seen on fluorescein staining. Differentiation from herpetic dendritic lesions (with terminal bulbs) is important.
Ciliary injection and limbal edema: Present even when corneal lesions are mild.
Advanced Stage
Ring infiltrate: A horizontally elongated oval stromal opacity centered in the mid-cornea. May be accompanied by corneal epithelial defects and progress to ring ulcer.
Disciform infiltrate: A large horizontally elongated oval area of edema and opacity in the central cornea.
Mutton-fat keratic precipitates and hypopyon: Inflammation spreads into the eye, producing fatty deposits on the posterior corneal surface.
Corneal perforation and scleritis: Seen in the most severe cases, and may be complicated by secondary glaucoma.
In the transitional phase between the early and advanced stages, the lesion begins to extend from the subepithelium into the superficial stroma, with linear and patchy opacities joining to form an irregular ring. Throughout the course, the inflammatory response is consistently severe, and the lesion progresses slowly. The period from the early to the advanced stage is typically about 1 to 2 months, and whether an accurate diagnosis and treatment can be started during this time greatly affects the prognosis.
In addition to this three-stage classification, a three-tier classification is also used: “Stage 1: epitheliopathy only,” “Stage 2: epithelial defect, perineural infiltrates, and stromal infiltrates,” and “Stage 3: stromal ring infiltrate.” Carnt et al. (2018) showed that a Stage 3 ring infiltrate, as part of the definition of severe inflammatory complications (SIC), is independently associated with poor prognosis2). Both classifications agree that early diagnosis before the appearance of stromal ring infiltrate is key to improving prognosis.
Acanthamoeba is a free-living amoeba found ubiquitously in soil, fresh water, tap water, pools, shower water, and other environments. It takes two forms: the trophozoite (active form) and the cyst (dormant form with a double wall). Cysts are highly resistant to freezing, heating, radiation, and various drugs.
Modifiable risk factors related to contact lens wear are as follows1).
Use of reusable soft contact lenses: OR 3.84 (95% CI 1.75–8.43) compared to daily disposable lenses
Use of hard contact lenses (including RGP): OR 4.56 (95% CI 1.03–20.19)
Reuse of lenses (reusing daily disposable lenses): OR 5.41 (95% CI 1.55–18.89)
Showering while wearing lenses: OR 3.29 (95% CI 1.17–9.23)
Low frequency of regular follow-up visits: OR 10.12 (95% CI 5.01–20.46)
Rinsing lenses or cases with tap water: The most common risk factor for orthokeratology lens-related Acanthamoeba keratitis3)
Carnt et al. estimated that simply switching from reusable soft lenses to daily disposable lenses could prevent 30–62% of Acanthamoeba keratitis cases1).
Multi-purpose solution (MPS) is the most widely used contact lens care product, but disinfection testing against Acanthamoeba is not required during the product approval process, and its disinfectant efficacy is extremely low, although there are some differences between products. Since Acanthamoeba requires bacteria as a food source for growth, preventing bacterial contamination through thorough rubbing and rinsing is key to infection prevention. Boiling disinfection can kill Acanthamoeba, but it is not performed with modern frequent-replacement soft lenses or daily disposable lenses.
Tap water is one of the main sources of Acanthamoeba, and rinsing lenses or lens cases with tap water is consistently cited as the greatest risk factor for contact lens-related Acanthamoeba keratitis worldwide. Wearing lenses while exposed to water—such as during showering, bathing in hot springs, swimming in pools, the sea, or rivers—also increases infection risk through the same mechanism. Case-control studies in Australia and the United Kingdom have consistently shown elevated odds ratios for the behavior of “showering while wearing lenses”, making it an important component of basic lifestyle guidance for lens wearers1).
In non-contact lens wearers, the pathogenesis of Acanthamoeba keratitis is primarily associated with trauma. Cases occurring after corneal epithelial damage caused by contaminated natural environmental foreign bodies such as plant fragments, sand, soil, and agricultural debris have been reported in tropical and developing countries including India. In Japan, sporadic cases of Acanthamoeba keratitis following trauma or ocular foreign bodies have been reported, but the predominant cause remains contact lens-related.
QAre daily disposable lenses safe?
A
Daily disposable lenses carry a lower risk compared to reusable lenses. However, behaviors such as wearing them in the shower or reusing them increase the risk1). Adherence to proper usage is essential.
Diagnosis of Acanthamoeba keratitis is challenging and often delayed. According to a German registry, 47.6% of Acanthamoeba keratitis cases were misdiagnosed as herpes keratitis4). Accurate diagnosis requires a combination of correct interpretation of clinical findings and microbiological examination.
In CL wearers presenting with treatment-resistant keratitis, this disease must always be included in the differential diagnosis. The following items must be confirmed during history taking:
Contact lens wear history and type: reusable soft, orthokeratology, or RGP; duration of wear; daily wearing time
Lens care method: care products used, whether rubbing/cleaning is performed, case replacement frequency
Tap water / water exposure history: lens rinsing with tap water, showering/bathing/hot spring use while wearing lenses, wearing lenses in pools, sea, or rivers
Symptom progression: onset time, discrepancy between pain severity and clinical findings, history of steroid eye drop use
Diagnosis based on slit-lamp microscopy findings is important. Understanding the characteristic findings according to disease stage (see Clinical Findings) and clinically suspecting the disease based on CL wear history and water exposure history is the first step.
Fluorescein staining findings are useful for differentiation. Herpetic dendriform lesions form terminal bulbs, whereas the pseudodendriform lesions of Acanthamoeba keratitis lack these bulbs and are observed as non-elevated, irregular clusters of lines.
With slit-lamp microscopy, findings change over time as the disease progresses, so it is important to perform detailed observations repeatedly not only at the initial visit but also at intervals of several days to one week. Particularly in the early stage, combining fluorescein staining, bright-light observation, and corneal sensitivity testing improves diagnostic accuracy. Corneal sensitivity decreases as radial keratoneuritis progresses, but clinically it is distinguished from herpetic keratitis by the presence of severe pain associated with the lesion.
The characteristics of the main examination methods are shown below.
Examination Method
Sensitivity
Specificity
Culture (Non-nutrient agar with E. coli overlay)
33–50%
100% (Gold standard)
Confocal microscopy (IVCM)
Approximately 90%
91.1–100%
PCR (18S rRNA gene)
71–84%
100%
Culture: Inoculate a corneal scraping specimen onto non-nutrient agar coated with E. coli. Since the organism does not grow on ordinary bacterial media, preparation of a special medium is essential. Although it is the gold standard for definitive diagnosis, its sensitivity is low at 33–50%3).
Smear microscopy: This is an extremely useful test. Fungiflora Y® staining enables fluorescent staining of the cyst wall. Diff-Quik™ (rapid staining) and Gram staining are also used. Identification of double-walled cysts is key to diagnosis.
Confocal microscopy (IVCM): This is a non-invasive and rapid test that allows direct observation of highly reflective double-walled cysts. Its sensitivity is approximately 90%, surpassing that of culture3). It requires specialized equipment and trained examiners.
PCR: Targets the Acanthamoeba 18S rRNA gene. Since Acanthamoeba is not normally present on the ocular surface, a positive result indicates a very high probability that it is the causative organism.
Corneal biopsy: Considered when cultures and PCR are negative, and the lesion is primarily within the stroma with an intact epithelium.
Specialized culture media and stains for microscopic examination are often not available in general clinics. Therefore, it is advisable to promptly refer the patient to a specialized facility as soon as this disease is suspected.
Herpes simplex keratitis: Differentiating from early pseudodendritic lesions is most important. Herpetic dendritic ulcers form rounded terminal bulbs at their ends and appear as well-defined elevated lesions. Pseudodendritic lesions in Acanthamoeba keratitis are not elevated and appear as irregular clusters of lines. In the mature stage, disciform keratitis in herpes appears as a well-defined perfect circle, while Acanthamoeba keratitis shows a horizontally elongated oval with irregular margins.
Fungal keratitis: Differentiation is difficult in the mature stage of stromal lesions, but fungal infections are characterized by feathery edges due to hyphae and satellite lesions with strong abscess formation. In Acanthamoeba keratitis, the margins appear as clusters of “fluffy” patchy opacities.
Bacterial keratitis: Usually progresses rapidly, worsening significantly within 48 hours, which differs from the slow progression of Acanthamoeba keratitis. In contact lens wearers, consider co-infection with bacterial keratitis caused by Pseudomonas aeruginosa, Streptococcus pneumoniae, and other bacteria.
Herpes zoster keratitis: Differentiate by checking for the presence or history of skin rash in the first division of the trigeminal nerve.
Mixed infections with multiple pathogens are not rare, and co-infection with bacteria such as Pseudomonas aeruginosa and Acanthamoeba has been reported, especially in contact lens wearers. It is important to perform smear microscopy, culture, and PCR comprehensively to identify the causative organism. In cases where the clinical picture resembles herpes but does not respond to antiviral drugs, or where treatment was started for bacterial infection but shows no improvement, prompt reassessment including Acanthamoeba should be performed.
QWhy is diagnosis often delayed?
A
Early clinical findings resemble herpes keratitis, and pseudo-dendritic lesions are easily mistaken for dendritic ulcers. In fact, approximately half of Acanthamoeba keratitis cases have been reported to be misdiagnosed as herpes4). In contact lens wearers with treatment-resistant keratitis, Acanthamoeba keratitis should be actively suspected, and early culture and confocal microscopy should be performed.
Treatment of Acanthamoeba keratitis is difficult and requires a long duration. No drugs with insurance coverage exist for Acanthamoeba, and treatment requires the use of self-prepared eye drops. The third edition of the Japanese Infectious Keratitis Clinical Practice Guidelines recommends “strongly recommend self-prepared eye drops (evidence level B)” for CQ-7: “Can self-prepared eye drops be recommended for the treatment of Acanthamoeba keratitis?“10).
Standard Treatment in Japan: Triple Combination Therapy
In Japan, the standard treatment is a triple therapy combining lesion debridement, topical anti-Acanthamoeba agents, and systemic antifungal agents10). Early diagnosis and prompt initiation of treatment are considered key to success.
This is the most important procedure in treatment. The Japanese guidelines for infectious keratitis also summarize its significance as follows10).
Direct therapeutic effect: Physically removes Acanthamoeba organisms.
Contribution to diagnosis: The debrided material can be examined by microscopy, culture, and PCR to enable diagnosis.
Improved drug penetration: Removing the corneal epithelium enhances the penetration of eye drops.
Assessment of treatment response: The clinical course can be evaluated by continuously examining the debrided material.
The corneal epithelium parasitized by Acanthamoeba has weak adhesion to the basement membrane, and even epithelium that appears healthy can be easily detached with gentle scraping. The principle is to remove all such epithelium10). Debridement is typically performed about once or twice a week, depending on the disease stage and clinical findings.
The first-line agents are biguanide disinfectants, which are prepared in-house and used. A major advantage is that they are effective not only against trophozoites but also against cysts; however, their tissue penetration is poor, requiring frequent instillation.
Chlorhexidine gluconate (CHG) eye drops 0.02–0.05%: Among topical antiseptic disinfectants, use products indicated for “conjunctival sac irrigation and disinfection.” Products containing ethanol for disinfection must never be used10).
PHMB (polyhexamethylene biguanide) eye drops 0.02%: High-grade stock solution is difficult to obtain, and some facilities may find it impractical to prepare in-house10).
A randomized controlled trial in the UK (51 eyes) reported no significant difference in clinical improvement rates within 2 weeks between the 0.02% PHMB monotherapy group (18/23 eyes = 78%) and the 0.02% CHG monotherapy group (24/28 eyes = 85.7%), indicating equivalent efficacy9)10). The Cochrane Review also identifies both agents, alone or in combination, as the best available evidence at present13).
The following may be used concomitantly as adjunctive agents.
Propamidine isethionate (Brolene®): Imported personally from overseas for use.
Antifungal eye drops: Pimaricin 5%, fluconazole 0.2%, miconazole, voriconazole 1%. Effective against trophozoites but not against cysts, therefore used as an adjunct to biguanides10).
1% voriconazole eye drops: A small RCT (18 eyes) conducted in India compared 1% voriconazole monotherapy with 0.02% PHMB + 0.02% CHG combination therapy and found no significant differences in corneal ulcer size, visual improvement, or healing time11). An observational study by Musayeva et al. (Germany, 26 cases) reported that adding 1% voriconazole to PHMB + CHG resulted in infection control in all cases, suggesting its usefulness as an adjunctive therapy12).
Typical prescription examples are as follows.
Hexzac W (0.02% CHG): Instill every hour (off-label use)
Atropine 1% ophthalmic solution: Instill 1–3 times daily (anti-inflammatory and cycloplegic)
During initial intensive treatment, frequent instillation is performed every hour (including at night), with gradual tapering based on clinical response. Typically, the frequency is reduced from every hour to every 2 hours after about one week, then gradually to every 3 hours and every 4 hours at monthly intervals. The treatment course usually lasts several months to over half a year, and abrupt tapering should be avoided as it may lead to recurrence.
In the systematic review for CQ-7 of the Infectious Keratitis Clinical Practice Guideline 3rd edition (“Can in-hospital formulated eye drops be recommended for the treatment of Acanthamoeba keratitis?”), it was determined that the benefits outweigh the harms given the absence of any approved pharmacotherapy under insurance coverage, and the conclusion of “strongly recommended” (evidence level B) was presented10). CHG eye drops are relatively inexpensive, but it should be noted that only a limited number of medical institutions are capable of in-hospital formulation.
When implementing triple combination therapy, management of concomitant infections and inflammation is also necessary. For prevention of bacterial co-infection, new quinolone eye drops (levofloxacin 1.5%, etc.) are used concomitantly, and for iridocyclitis, a mydriatic agent (atropine 1%) is used. Steroids are generally not used; however, only in cases where severe inflammatory findings persist despite adequate response to anti-amoebic treatment, short-term, low-dose steroid eye drops may be used in a limited manner at the discretion of a specialist. However, the indications are limited, and they are contraindicated at the initial visit or in the early stages of treatment.
In-hospital formulated eye drops are often prepared by the pharmacy department of each institution, and protocols for concentration and storage period vary by facility. Generally, the expiration period is approximately 4 weeks for 0.02% CHG and about 2 weeks for 0.02% PHMB. Patients should be instructed to store them in a cool place, shake before use, and strictly adhere to the expiration date.
Systemic administration of antifungal drugs (such as oral itraconazole) may be used in combination. The Japanese guidelines state that “the efficacy of systemic administration has not been clarified,” and its role remains only adjunctive10).
Evaluation of treatment efficacy is performed comprehensively using periodic microscopy, culture, and PCR of lesion scrapings, reduction in infiltration size on slit-lamp findings, and alleviation of subjective symptoms (particularly pain). In facilities where IVCM can be performed regularly, it enables non-invasive assessment of residual cysts within the cornea. With effective treatment, in early-stage cases, transparent healing with only minimal scarring can be expected. Conversely, even in fairly advanced cases, opacification can be reduced with extended treatment, and a characteristic feature of Acanthamoeba keratitis is that corneal shape changes are surprisingly minimal. Therefore, if treatment efficacy is confirmed even with slow progress, there is no need to rush into corneal transplantation.
On the other hand, when treatment is completely ineffective, therapeutic corneal transplantation must be performed before Acanthamoeba spreads to the periphery; otherwise, enucleation may be necessary in the worst case. Important indicators of progress after initiating treatment include: ① improvement in pain, ② reduction in infiltration size, ③ progression of corneal epithelialization, and ④ resolution of inflammatory complications (hypopyon, scleritis, ring infiltrate). If these findings show no improvement even after 3 to 4 weeks, it is necessary to consider medication changes or surgical intervention.
Surgical treatment is considered for cases that are resistant to drug therapy or have developed corneal perforation10).
Superficial keratectomy: Performed in cases with poor response to drug therapy, when the effect of lesion scraping is uncertain, to remove the lesion along with the pathogen.
Therapeutic corneal transplantation (penetrating keratoplasty; PKP): Performed for cases unresponsive to drug therapy or with corneal perforation. Indications, techniques, and postoperative management vary by institution and no consensus has been established. If possible, it is desirable to perform surgery after inflammation has subsided, and if active infection remains, postoperative anti-amoebic therapy must be continued. The risk of recurrence after corneal transplantation is high, and graft failure has also been reported8).
Carnt et al. (2018) reported in a retrospective study of 194 cases that steroid use before initiation of anti-amoebic therapy increased the risk of poor prognosis by approximately 4-fold2). Twenty-five percent of poor prognosis cases required 55 or more outpatient visits and 58 or more months of follow-up. Additionally, age over 34 years, symptom duration over 37 days, and the presence of scleritis or stromal ring infiltrate were independent poor prognostic factors2).
QCan steroid eye drops be used?
A
The Japanese Infectious Keratitis Clinical Practice Guidelines, 3rd edition, do not recommend steroid eye drops for Acanthamoeba keratitis10). Steroid use before treatment is a poor prognostic factor2). However, in some cases with persistent severe inflammation, steroids may be used on a limited basis at the discretion of a specialist after sufficient anti-amoebic treatment.
The life cycle of Acanthamoeba consists of two stages: the trophozoite and the cyst. Trophozoites (20–40 μm in length) possess pseudopodia, are motile, feed on bacteria and yeast, and proliferate by binary fission. Trophozoites initiate invasion by adhering to mannosylated glycoproteins on the corneal epithelial surface. Cysts (10–20 μm in diameter) have a double-layered cyst wall and form under adverse conditions. Cysts exhibit resistance to desiccation, heat, and chemicals, and are highly tolerant to freezing, heating, radiation, and many drugs. This cyst resistance is the single most important factor that makes treatment of Acanthamoeba keratitis difficult.
Microtrauma to the corneal epithelium caused by contact lens wear promotes amoeba adhesion and invasion. Currently, contact lens care products (multipurpose solutions; MPS) are not required to be tested against Acanthamoeba, and their disinfectant efficacy is extremely low. However, since Acanthamoeba requires bacteria as a food source for growth, thorough rubbing and cleaning to prevent general bacterial contamination is a practical preventive measure.
The progression of infection is as follows.
Adhesion to the epithelium: Amoebae attach to sites of corneal epithelial damage that occur during contact lens wear.
Proliferation and migration within the epithelium: Trophozoites move within the epithelium forming infectious foci. Infection begins in the superficial central cornea and gradually expands to the periphery.
Nerve invasion: Infiltrates along corneal nerves, causing radial keratoneuritis. Involvement of cytokines (such as interleukin-1) and nociceptors has been suggested4).
Deep stromal penetration: Infection progression is extremely slow, and it takes time to reach the deep corneal stroma. Meanwhile, the inflammatory response is consistently severe throughout the course.
A confocal microscopy study by Kurbanyan et al. reported that corneal nerve density, length, and branching are significantly reduced in active Acanthamoeba keratitis4). This neural change may contribute to the painless nature of Acanthamoeba keratitis.
Regarding orthokeratology (OK) lenses, the risk of developing Acanthamoeba keratitis is higher than with conventional RGP lenses. The unique reverse geometry design of OK lenses is thought to induce corneal epithelial thinning and superficial cell damage, and overnight wear-related corneal hypoxia together with tear pooling under the reverse curve are believed to promote pathogen colonization3). Additionally, many OK lens wearers are schoolchildren and young adults, and frequent lens washing or rinsing with tap water also contributes to the increased risk.
As noted earlier, cysts are resistant to many drugs, and this resistance is largely due to the double-layered cyst wall structure. The outer wall (ectocyst) is composed mainly of amorphous proteins, while the inner wall (endocyst) contains abundant cellulose-like polysaccharides, which inhibit the penetration of both hydrophilic and hydrophobic drugs. Because of this structural resistance, antifungal agents and aminoglycoside antibiotics are almost ineffective against cysts, and biguanide disinfectants (CHG, PHMB), which are effective against cysts, are the mainstay of treatment. However, biguanide disinfectants also have poor tissue penetration, making it essential to remove the epithelial barrier through lesion debridement. This is the theoretical basis for why lesion debridement is considered most important in Japan’s triple-combination therapy.
The host immune response plays a significant role in the clinical presentation of Acanthamoeba keratitis. Stromal ring infiltrate is thought to result from neutrophil and T-cell infiltration due to a delayed-type hypersensitivity reaction to Acanthamoeba antigens, while scleritis is presumed to occur through amoebic antigen or T-cell clone dissemination to the sclera via a mechanism similar to sympathetic inflammation2). Carnt et al. (2018) showed that these severe inflammatory complications are independently associated with age over 34 years, pre-treatment steroid use, and prior herpes treatment history, suggesting that individual differences in immune response are one of the factors influencing prognosis2).
7. Latest Research and Future Perspectives (Investigational Reports)
Studies are progressing on monotherapy using 0.08% PHMB, which is four times the concentration of conventional 0.02% PHMB.
Di Zazzo et al. (2024) reported the world’s first clinical use of 0.08% PHMB monotherapy in two cases that were resistant to standard therapy with 0.02% PHMB plus propamidine 0.1% for 4 to 6 weeks5). The protocol involved hourly instillation (16 drops/day during daytime only) for the first 5 days, followed by gradual tapering. In both cases, infection resolved within 15 to 30 days, and no recurrence was observed for over 7 months.
The ODAK trial (Dart et al. 2024) reported that the cure rate was approximately 86% for both PHMB 0.08% monotherapy and PHMB 0.02% plus propamidine 0.1% combination therapy5).
This is a technique that applies cross-linking using riboflavin and ultraviolet A (UVA) to infectious keratitis.
Watson et al. (2022) reported a case of refractory Acanthamoeba keratitis that had failed maximal medical therapy (including miltefosine, voriconazole, PHMB, and chlorhexidine) and was treated with PACK-CXL. Pain completely resolved within 4 weeks, and infiltrates decreased over 10 weeks6).
However, in vitro and in vivo experiments have not confirmed the amoebicidal or cysticidal effect of riboflavin/UVA irradiation6). Indirect mechanisms are suspected, including tissue protection through collagen stabilization, suppression of amoeba proliferation, reduction of amoeba burden by epithelial debridement, and pain relief from decreased corneal nerve density.
This agent belongs to the alkylphosphocholine class and is active against both trophozoites and cysts. In 2016, it received FDA orphan drug designation for the treatment of Acanthamoeba keratitis. It is positioned as adjunctive therapy for refractory cases that have failed standard treatment for 4 to 6 weeks6)7).
In a 4-case series by Smith et al. (2022), combination therapy including miltefosine was used together with corneal transplantation, and disease control was ultimately achieved in all cases7). However, some cases required discontinuation due to tolerability issues (gastrointestinal symptoms).
The main adverse effects of miltefosine include gastrointestinal symptoms (nausea, vomiting), teratogenicity, and nephrotoxicity. Stevens-Johnson syndrome and severe thrombocytopenia have been reported rarely 7). Regular monitoring of liver function is required during administration. It is not approved in Japan and is limited to personal import or use in clinical research. It is a treatment option whose future development is worth attention.
Carnt N, Minassian DC, Dart JKG. Acanthamoeba Keratitis Risk Factors for Daily Wear Contact Lens Users: A Case-Control Study. Ophthalmology. 2023;130(1):48-55. doi:10.1016/j.ophtha.2022.08.002. PMID:35952937.
Carnt N, Robaei D, Minassian DC, Dart JKG. Acanthamoeba keratitis in 194 patients: risk factors for bad outcomes and severe inflammatory complications. The British journal of ophthalmology. 2018;102(10):1431-1435. doi:10.1136/bjophthalmol-2017-310806. PMID:29298778.
Wu J, Xie H. Orthokeratology lens-related Acanthamoeba keratitis: case report and analytical review. The Journal of international medical research. 2021;49(3):3000605211000985. doi:10.1177/03000605211000985. PMID:33752507; PMCID:PMC7995463.
Wróbel-Dudzińska D, Ziaja-Sołtys M, Rymgayłło-Jankowska B, Derda M, Klepacz R, Zalewski D, et al. Complicated Diagnosis and Treatment of Rare Painless Acanthamoeba Keratitis. Journal of clinical medicine. 2025;14(13). doi:10.3390/jcm14134763. PMID:40649137; PMCID:PMC12251361.
Di Zazzo A, De Gregorio C, Coassin M. Novel Effective Medical Therapy for Acanthamoeba Keratitis. Eye & contact lens. 2024;50(6):279-281. doi:10.1097/ICL.0000000000001092. PMID:38709240; PMCID:PMC11101174.
Watson SH, Shekhawat NS, Daoud YJ. Treatment of recalcitrant Acanthamoeba Keratitis with Photoactivated Chromophore for Infectious Keratitis Corneal Collagen Cross-Linking (PACK-CXL). American journal of ophthalmology case reports. 2022;25:101330. doi:10.1016/j.ajoc.2022.101330. PMID:35112032; PMCID:PMC8790275.
Smith C, Ashraf N, Haghnegahdar M, Goins K, Newman JR. Acanthamoeba Keratitis: A Single-Institution Series of Four Cases With Literature Review. Cureus. 2022;14(1):e21112. doi:10.7759/cureus.21112. PMID:35165570; PMCID:PMC8830394.
Lin H, Khaliddin N. Different Outcomes of Acanthamoeba Keratitis: A Case Series. Cureus. 2023;15(11):e48129. doi:10.7759/cureus.48129. PMID:38046722; PMCID:PMC10692316.
Lim N, Goh D, Bunce C, Xing W, Fraenkel G, Poole TR, et al. Comparison of polyhexamethylene biguanide and chlorhexidine as monotherapy agents in the treatment of Acanthamoeba keratitis. American journal of ophthalmology. 2008;145(1):130-5. doi:10.1016/j.ajo.2007.08.040. PMID:17996208.
Bagga B, Sharma S, Gour RPS, et al. A randomized masked pilot clinical trial to compare the efficacy of topical 1% voriconazole ophthalmic solution as monotherapy with combination therapy of topical 0.02% polyhexamethylene biguanide and 0.02% chlorhexidine in the treatment of Acanthamoeba keratitis. Eye (Lond). 2021;35:1326-1333. doi:10.1038/s41433-020-1109-4. PMID:32719525; PMCID:PMC8182824.
Musayeva A, Riedl JC, Schuster AK, Wasielica-Poslednik J, Pfeiffer N, Gericke A. Topical Voriconazole as Supplemental Treatment for Acanthamoeba Keratitis. Cornea. 2020;39(8):986-990. doi:10.1097/ICO.0000000000002315. PMID:32243421.
Alkharashi M, Lindsley K, Law HA, Sikder S. Medical interventions for Acanthamoeba keratitis. Cochrane Database Syst Rev. 2015;(2):CD010792. doi:10.1002/14651858.cd010792.pub2.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.