Peripheral ulcerative keratitis (PUK) is a group of diseases characterized by crescent-shaped destructive inflammation of the corneal stroma near the limbus. It features corneal stromal degeneration, inflammatory cell infiltration, and epithelial defects, and can progress to corneal thinning, descemetocele, and perforation. It is a general term for diseases presenting with peripheral corneal ulcers, including idiopathic Mooren’s ulcer, ulcers associated with collagen diseases such as rheumatoid arthritis, staphylococcal allergy (catarrhal corneal ulcer), and corneal phlyctenules.
The incidence is rare at 0.2–3 cases per million per year, with no gender difference 8). About 50% have an underlying systemic disease, of which approximately 20% are infectious 8). Rheumatoid arthritis (RA) is the most common cause, accounting for 34–42% of PUK patients 2).
Epidemiological Background of Rheumatoid Arthritis
Rheumatoid arthritis is the most common collagen disease. The prevalence in Japan is reported to be 5.4 per 1,000 women and 1.1 per 1,000 men. It is more common in women aged 30–60, and the proportion of men increases with age. About 70% of RA patients show a genetic correlation with HLA-DR4. It is also known that RA can develop or worsen after trauma or childbirth.
Among RA, the type complicated by vasculitis is called malignant rheumatoid arthritis. It is accompanied by scleritis, pleuritis, interstitial pneumonia, pericarditis, myocarditis, multiple mononeuritis, mesenteric artery embolism, and fingertip ulcers, and has a poor systemic prognosis. Most RA-related PUK occurs with this malignant rheumatoid arthritis, causing rapid corneal thinning and perforation.
The development of PUK is thought to involve autoimmune reactions against corneal antigens, deposition of circulating immune complexes, and hypersensitivity reactions to foreign antigens. A special feature of the peripheral cornea is that the limbus is densely packed with vascular networks, immune systems, and nervous systems, making it an environment where immune complexes are easily deposited. In PUK associated with collagen diseases, autoantibodies in the blood deposit in the corneal limbus and periphery, triggering a type III allergic reaction, and extracellular matrix-degrading enzymes released from infiltrated immune cells are involved in ulcer formation.
Mooren’s ulcer is defined as a peripheral corneal ulcer of unknown cause without systemic autoimmune disease. In contrast, PUK is a condition that develops in association with systemic diseases, and distinguishing between the two is important for determining treatment strategy. In Mooren’s ulcer, scleritis is mild, but in peripheral ulcers associated with collagen diseases, gray-white lesions progress toward the center of the cornea secondary to episcleritis or scleritis, often accompanied by vascular invasion.
QWhat is the difference between PUK and Mooren's ulcer?
A
PUK is a peripheral corneal ulcer that develops in association with systemic autoimmune diseases such as rheumatoid arthritis and ANCA-associated vasculitis. In contrast, Mooren’s ulcer is an idiopathic peripheral corneal ulcer without systemic disease, and involvement of autoantibodies against corneal epithelial cells has been suggested. Clinically, Mooren’s ulcer is associated with mild scleritis, whereas PUK is complicated by scleritis in about 36% of cases. Systemic evaluation is key to differentiation.
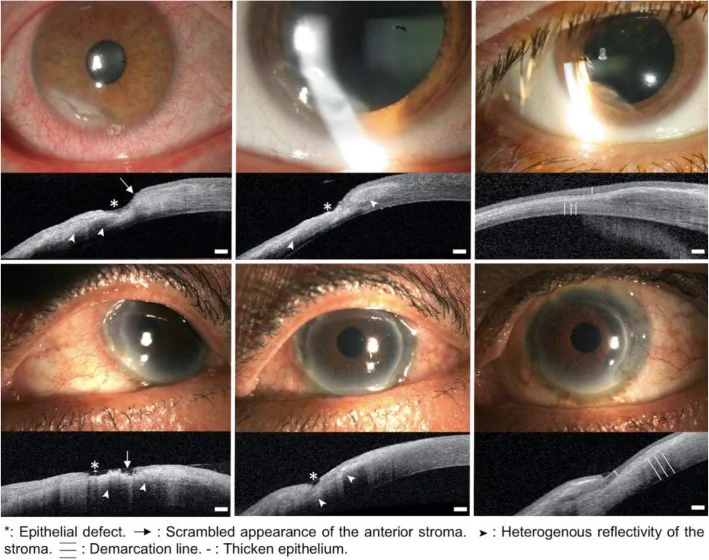
Bonnet C, Debillon L, Al-Hashimi S, et al. Anterior segment optical coherence tomography imaging in peripheral ulcerative keratitis, a corneal structural description. BMC Ophthalmol. 2020;20:205. Figure 1. PMCID: PMC7249626. License: CC BY 4.0.
Slit-lamp microscopy and AS-OCT images of two cases (upper row: case 1, middle row: case 2) that followed a good course with treatment, showing from left: active stage, healing process, and healed stage. These correspond to the findings of the peripheral cornea associated with the progression stages of the lesion (active, healing, healed) discussed in the section “2. Main Symptoms and Clinical Findings.”
Eye pain: Severe pain associated with corneal ulcer. When complicated by scleritis, it becomes deep pain radiating to the face or temple, intensifying enough to disturb sleep.
Hyperemia: Accompanied by ciliary injection, often localized. In cases complicated by scleritis, it presents as intense, circumferential hyperemia due to dilation and tortuosity of scleral vessels.
Decreased visual acuity: Occurs depending on the degree of corneal opacity and thinning.
Photophobia and tearing: Appear with corneal epithelial damage.
Dryness and foreign body sensation: In patients with rheumatoid arthritis, severe dry eye (secondary Sjögren syndrome) often coexists, accompanied by foreign body sensation and dryness of the ocular surface.
The corneal finding in PUK is a crescent-shaped stromal destruction localized near the limbus. In PUK associated with collagen disease, the lesion often progresses toward the central cornea secondary to scleritis or episcleritis.
Corneal stromal infiltration and ulceration: Crescent-shaped infiltration and stromal necrosis parallel to the limbus. The leading edge of the ulcer has a deep tunnel-like appearance called undermining.
Epithelial defect: The epithelium over the ulcer is lost, staining positive with fluorescein.
Corneal thinning: As it progresses, the corneal stroma becomes markedly thin. In severe cases, an hourglass cornea is observed 4).
Paracentral corneal perforation: In severe cases, perforation occurs near the central cornea. Perforation is accompanied by a pear-shaped pupil and prolapse of iris tissue 3).
Scleritis complication: Approximately 36% of PUK patients develop scleritis. Scleritis is inflammation of the deep scleral vascular plexus, causing scleral edema and cellular infiltration.
Ocular complications associated with rheumatoid arthritis range from dry eye to scleral perforation, showing a wide spectrum of severity. Important related findings for understanding PUK are listed below.
Keratoconjunctivitis sicca: Frequently complicates as secondary Sjögren syndrome.
Episcleritis: Inflammation of superficial vascular plexus such as Tenon’s capsule vessels. Mild pain and normal vision.
Scleritis (diffuse/nodular): Deep vascular congestion with eye pain. Mainly granulomatous inflammation and vasculitis.
Necrotizing scleritis: Central yellowish-white ischemic area. Poor prognosis; leads to blindness or difficulty preserving the eye without early treatment.
Scleromalacia perforans: Occurs in patients with long-term treatment for RA. Sclera gradually thins without congestion or pain around the thin area, exposing the uvea.
Peripheral corneal ulcer: Common in malignant rheumatoid arthritis, rapidly progresses to thinning and perforation.
QIn which type of rheumatoid arthritis is corneal ulcer more likely to occur?
A
Peripheral corneal ulcers and necrotizing scleritis are more likely to occur in malignant rheumatoid arthritis complicated by vasculitis. RA with extra-articular manifestations such as scleritis, pleuritis, interstitial pneumonia, pericarditis, mononeuritis multiplex, and fingertip ulcers falls into this type, and both ocular and systemic prognoses are poor. Control of rheumatoid arthritis disease activity is the basis of PUK treatment.
PUK is secondary to a wide variety of systemic diseases. Broadly classified into autoimmune, infectious, and others.
Autoimmune (most common)
Rheumatoid arthritis (RA): Accounts for 34–42% of PUK patients, the most common cause 2). Risk is particularly high in malignant rheumatoid arthritis complicated by vasculitis, which can rapidly lead to perforation.
ANCA-associated vasculitis: Granulomatosis with polyangiitis (GPA, formerly Wegener’s granulomatosis) causes scleritis and peripheral corneal ulcers resistant to standard treatment. PR3-ANCA positivity is about 80%.
Relapsing polychondritis: May be accompanied by scleritis or uveitis.
Inflammatory bowel disease (IBD): 2–5% of IBD patients develop ocular symptoms such as episcleritis, scleritis, or uveitis9).
Infectious and Other Causes
Large vessel vasculitis: Peripheral ulcerative keratitis (PUK) associated with giant cell arteritis (GCA) has been reported. FDG-PET was useful for diagnosis2).
Hidradenitis suppurativa (HS): A rare cause, but sharing of the Th17 pathway has been suggested3)7). Anterior uveitis is the most common ocular inflammation in HS patients; PUK is rare.
Granulomatous rosacea: Chronic inflammation and Th17 activation are involved; cases with PUK have been reported1).
Immune checkpoint inhibitors: Bilateral PUK has been reported as an immune-related adverse event (irAE) of ipilimumab/nivolumab combination therapy5).
Infectious: A case of Citrobacter koseri canaliculitis causing PUK has been reported6). PUK associated with tuberculosis has also been reported4).
QWhat systemic diseases cause PUK?
A
The most common cause is rheumatoid arthritis, accounting for about one-third of PUK patients. Other major causes include ANCA-associated vasculitis (e.g., granulomatosis with polyangiitis), polyarteritis nodosa, systemic lupus erythematosus, relapsing polychondritis, and inflammatory bowel disease. Rarely, it can also occur as an immune-related adverse event from hidradenitis suppurativa, granulomatous rosacea, or immune checkpoint inhibitors. Infectious causes include bacterial canaliculitis and tuberculosis.
Slit-lamp examination: Evaluate the extent and depth of peripheral corneal infiltration, ulceration, and thinning. Check for epithelial defects using fluorescein staining.
Differentiation between scleritis and conjunctival/episcleral injection: Instillation of 1:1000 diluted epinephrine resolves conjunctival and limbal injection, but does not resolve vascular dilation due to scleritis.
Fluorescein scleral angiography: Evaluates the presence of scleral non-perfusion areas and is used to differentiate from necrotizing scleritis.
Ocular ultrasound (B-scan): Useful for evaluating posterior scleritis. Findings include scleral thickening, scleral nodules, separation of Tenon’s capsule from the sclera, and signs of extraocular myositis.
Corneal scraping and culture: Performed to rule out infectious causes. If infection is strongly suspected, biopsy of the lesion may also be considered.
Anterior segment OCT (AS-OCT): Useful when corneal opacity is severe and depth assessment by slit-lamp examination is difficult. AS-OCT can classify PUK into the following three stages:
Acute stage: Loss of corneal epithelium, structural destruction of the anterior stroma with heterogeneous reflectivity, and decreased corneal thickness in the affected area.
Healed stage: A clear boundary line forms between the low-reflective epithelium and high-reflective stroma, with stabilization of scarred corneal thickening and thinning.
To identify underlying diseases, the following tests are performed systematically. For the diagnosis of rheumatoid arthritis, elevated ESR, elevated CRP, and positive rheumatoid factor (RF) are useful (RF is negative in about 1/4 of cases). MMP-3 is useful as a marker of synovial proliferation and is also used to assess disease activity.
Other tests such as peripheral blood tests, renal function, urinalysis, hepatitis B/C virus tests, sacroiliac joint X-ray, and sinus CT are added as needed. If large vessel vasculitis is suspected, FDG-PET is useful, with reported sensitivity of 90% and specificity of 98% 2).
Clear zone between the ulcer and limbus. Type III allergy to staphylococcus.
Catarrhal corneal ulcer is a sterile infiltration and ulceration that occurs in the peripheral cornea due to a type III allergic reaction to staphylococcal exotoxins. It commonly occurs at the 2, 4, 8, and 10 o’clock positions, and differs from PUK in that there is a 1-2 mm clear zone between the ulcer and the limbus. Mooren’s ulcer occurs suddenly in one or both eyes, presenting as an arcuate ulcer along the limbus with a steep undermined edge, but there is no clear zone between the ulcer and the limbus.
The goals of PUK treatment are to control inflammation, prevent secondary infection, promote ulcer healing, and prevent perforation. When associated with collagen disease, treatment of the underlying collagen disease is the highest priority, and treatment should be coordinated with the rheumatology department. PUK cannot be controlled if rheumatoid arthritis is poorly controlled. Even if short-term inflammation control is possible with PUK treatment alone, the risk of recurrence and perforation persists if systemic disease activity is high. Therefore, the treatment plan should be jointly determined by ophthalmology and internal medicine.
Artificial tears and punctal plugs: Used to treat dry eye and promote epithelialization. Preservative-free formulations are recommended. Hyaluronic acid eye drops (Hyalein®) and rebamipide eye drops (Mucosta®) may be used concomitantly.
Antibiotic eye drops: Used to prevent secondary infection.
0.05% cyclosporine eye drops: Used to suppress local inflammation. Since commercially available immunosuppressive eye drops are not indicated for this purpose, a 0.05% in-house preparation is used. Tacrolimus eye drops have also been reported for Mooren’s ulcer.
Dexamethasone subconjunctival injection: Inject 0.4 mL of Decadron® injection into the conjunctival hyperemia near the ulcer.
Topical steroid eye drops: Use with extreme caution as they may promote corneal melting (keratolysis). In mild cases with scleritis, 0.1% betamethasone eye drops may be started 4-6 times daily.
Oral doxycycline: Used concomitantly for its collagenase inhibitory effect. Vitamin C may also be used to aid collagen remodeling.
COX2 inhibitor (celecoxib): For mild scleritis, celecoxib 100 mg is taken orally twice daily. It is highly effective for pain and also effective for inflammation control. If there are no contraindications such as asthma, it should be actively used from the initial stage.
Cyanoacrylate adhesive: Applied to the ulcer bed when perforation is imminent 5).
Azathioprine: Indicated for treatment-resistant RA and vasculitis, but reports suggest its efficacy for scleritis is inferior to MTX and cyclophosphamide; caution is needed in selection.
Cyclosporine: Since 2013, its insurance coverage has expanded, and it is used for non-infectious uveitis and sclerouveitis. Start at 2–3 mg/kg/day and adjust so that trough blood levels do not exceed 150 mg/mL. Side effects include renal dysfunction, requiring regular blood tests. Contraindicated in scleritis associated with neuro-Behçet disease.
Biologics: Introduced in refractory cases resistant to immunosuppressant therapy.
Anti-TNF-α antibodies: Infliximab (Remicade®) and adalimumab (Humira®) are used. As DMARDs for rheumatoid arthritis, they show high efficacy in inhibiting bone destruction and are also effective for sclerouveitis.
Rituximab: Anti-CD20 antibody. Used for refractory PUK and vasculitis.
Etanercept caution: Paradoxical reactions inducing ocular inflammation including scleritis have been reported with TNFα inhibitors; not recommended for scleritis cases.
Adalimumab has been reported effective for PUK associated with hidradenitis suppurativa 7).
DMARD therapy for rheumatoid arthritis itself: Disease-modifying antirheumatic drugs are used early and aggressively to prevent progression of joint destruction. Immunosuppressants such as methotrexate and biologic DMARDs such as anti-TNF-α antibodies are central. In recent years, early use of biologics has suppressed bone destruction and significantly improved long-term quality of life (QOL). NSAIDs and oral steroids are used short-term for joint symptom relief.
Infection prevention: Before and during the use of immunosuppressive drugs or biologics, systemic examinations are required, and screening for reactivation of hepatitis B virus and latent tuberculosis infection is essential.
QCan steroid eye drops be used for PUK treatment?
A
Topical steroid eye drops may promote corneal melting (keratolysis), so they must be used cautiously in PUK treatment. The mainstay of treatment is systemic immunosuppressive therapy, with oral prednisolone 1–1.5 mg/kg/day as the cornerstone, combined with methotrexate in cases with rheumatoid arthritis and cyclophosphamide in cases with vasculitis. For topical treatment, cyclosporine eye drops and oral doxycycline are recommended.
Corneal perforation or impending perforation is an indication for surgical intervention.
Conjunctival resection (Brown’s surgery): Effective for Mooren’s ulcer. Resect the hyperemic conjunctiva 3–4 mm wide from the limbus, extending 2 clock hours from each end of the ulcer. Also applied to peripheral ulcers associated with collagen diseases.
Corneal epithelioplasty: After conjunctival resection, if the sclera is left exposed, pathological conjunctiva may re-extend. Therefore, thin corneal epithelial sheets prepared from donor cornea are sutured like a dike at the limbus in 2–3 pieces. A contact lens is worn postoperatively.
Superficial keratoplasty: Performed when disease activity is high and corneal perforation is unavoidable. Use preserved cornea, thoroughly scrape the proliferative tissue at the ulcer base with a golf knife, then transplant. May be combined with Brown’s surgery or corneal epithelioplasty.
Lamellar keratoplasty: There is a report of lamellar mini-keratoplasty performed in a case of checkpoint inhibitor-related PUK with perforation5).
Tenon’s capsule sling graft: For advanced PUK with an hourglass-shaped cornea, a modified Tenon’s capsule sling ring patch graft has been reported4). It has the advantage of being autologous tissue with no rejection.
Patch graft: For perforating scleromalacia, surgical scleral repair such as patch graft is performed at the perforation site to prevent phthisis bulbi.
Postoperatively, topical and systemic administration of steroids or immunosuppressive drugs must be continued to suppress rejection. In cases of perforation due to scleritis, scleral thinning is extensive and disease activity tends to persist postoperatively, so combination with systemic immunosuppressive therapy is essential.
Subconjunctival injection of dexamethasone implant (Ozurdex) has been reported to be effective for PUK. In elderly patients who cannot tolerate systemic immunosuppressive therapy, three injections controlled inflammation for 11 months without scleral melting or elevated intraocular pressure8).
The pathogenesis of PUK involves both humoral and cellular immunity. In rheumatoid arthritis and vasculitis, inflammatory cytokines are overproduced in the synovium and vascular walls, creating a predisposition for type III allergic reactions systemically. Immune complexes produced by autoantibodies deposit in the vessels of the corneal limbus and periphery, activating the classical complement pathway. Complement activation induces chemotaxis of neutrophils and macrophages, which release collagenases and proteases.
Pro-inflammatory cytokines (TNF-α, IL-6, etc.) stimulate keratocytes to produce matrix metalloproteinases (MMPs) 1). MMPs degrade collagen in the peripheral cornea, leading to corneal thinning and ulcer formation. In rheumatoid arthritis, joint pathology involves synovial lymphocyte infiltration, angiogenesis, and synovial proliferation, with inflammatory cytokines causing tissue destruction via chondrocyte death and osteoclast activation; similar mechanisms are thought to operate in the peripheral cornea.
Recently, the role of Th17 cells and IL-17 has gained attention 1). Cytokines such as TGF-β1, IL-6, and IL-21 promote Th17 differentiation, and IL-1 further stimulates it. IL-17 secreted by Th17 enhances MMP production, promoting corneal stromal degradation 1). Suppression of Th17 has been reported to reduce ocular complications of PUK 1).
In granulomatous rosacea, IL-37 is released from the epidermis, activating mast cells to release proteases such as chymase, tryptase, and MMPs 1). This inflammatory microenvironment is thought to promote Th17 polarization, leading to PUK development 1).
When peripheral corneal ulcers or necrotizing scleritis are present, visual prognosis is often poor. Necrotizing scleritis commonly occurs in the 60s, with bilateral involvement in about 60% of cases; without early appropriate treatment, it can lead to blindness or loss of the eye. In malignant rheumatoid arthritis, systemic vasculitis affecting the lungs, heart, and kidneys impacts not only visual function but also life prognosis. Scleromalacia perforans typically occurs in patients with long-standing RA, and by the time typical findings appear, the window for treatment has often passed. Early diagnosis and early treatment intervention are key to improving prognosis.
Reasons Why the Peripheral Cornea Is a Predilection Site
The limbus is the border between the corneal epithelium and conjunctival epithelium, and is a region rich in vascular, immune, and nervous systems. The limbus contains abundant Langerhans cells, which are involved in antigen presentation. While the central cornea is avascular, the peripheral cornea is more susceptible to immune complex and inflammatory cell supply from the limbal vascular network. Due to this anatomical characteristic, in peripheral ulcers associated with collagen diseases, immune complexes deposit in the limbus and peripheral cornea, triggering a type III allergic reaction, and extracellular matrix-degrading enzymes released from infiltrated immune cells contribute to ulcer formation.
QWhy do lesions occur in the peripheral cornea?
A
The limbus is a region where the vascular network, immune system, and nervous system are densely packed, and Langerhans cells are abundant. While the central cornea is avascular, the peripheral cornea is more easily supplied with immune complexes and inflammatory cells from the limbal vascular network. In autoimmune diseases, immune complexes deposit in limbal vessels, activating the complement system, and neutrophils and macrophages accumulate to destroy the corneal stroma, so lesions tend to occur in the peripheral region.
With the widespread use of immune checkpoint inhibitors (ICIs), PUK as an irAE has been reported. In combination therapy with ipilimumab (anti-CTLA-4 antibody) and nivolumab (anti-PD-1 antibody), the incidence of irAE is reported to be over 90% 5). ICI-related PUK may be resistant to high-dose steroid eye drops and cyclosporine eye drops, and cases requiring lamellar keratoplasty have been reported 5). Balancing continuation of cancer treatment and management of irAE is a challenge, and collaboration with oncology is essential.
For patients who cannot tolerate systemic immunosuppressive therapy, subconjunctival injection of a dexamethasone implant (Ozurdex) has been attempted 8). Repeated administration achieved long-term inflammation control without scleral melting or elevated intraocular pressure8). As a local treatment that avoids systemic side effects, further validation is expected.
Since the Th17/IL-17 pathway is deeply involved in the pathology of PUK, therapies targeting Th17 are attracting attention. In a case of PUK associated with granulomatous rosacea that responded to isotretinoin, it has been suggested that isotretinoin’s Th17-suppressive effect and regulatory T cell-promoting effect may have been involved 1).
A modified Tenon’s capsule sling graft for advanced PUK has been reported 4). Since it uses autologous tissue, there is no rejection, and it can be performed even when donor corneas are difficult to obtain 4).
Hsiao FC, Meir YJ, Hsiao CH, et al. Peripheral ulcerative keratitis in a patient with granulomatous rosacea. Taiwan J Ophthalmol. 2023;13(1):80-83. doi:10.4103/tjo.tjo-d-22-00079.
Uchida S, Kaji Y, Ui M, Kawashima H, Usui T, Ohira Y. Peripheral Ulcerative Keratitis Associated With Large Vessel Vasculitis. Cureus. 2021;13(6):e15767. doi:10.7759/cureus.15767. PMID:34290940; PMCID:PMC8290306.
Dallalzadeh LO, Ang MJ, Beazer AP, Spencer DB, Afshari NA. Peripheral ulcerative keratitis secondary to severe hidradenitis suppurativa. American journal of ophthalmology case reports. 2022;25:101403. doi:10.1016/j.ajoc.2022.101403. PMID:35198822; PMCID:PMC8844392.
Anitha V, Ghorpade A, Ravindran M. A modified Tenons sling annular graft for advanced peripheral ulcerative keratitis with an hourglass cornea. Indian J Ophthalmol. 2022;70(2):655-657. doi:10.4103/ijo.IJO_2035_21. PMID:35086257; PMCID:PMC9023998.
Aschauer J, Donner R, Lammer J, Schmidinger G. Bilateral corneal perforation in Ipilimumab/Nivolumab-associated peripheral ulcerative keratitis. Am J Ophthalmol Case Rep. 2022;28:101686. doi:10.1016/j.ajoc.2022.101686.
Acharya I, Jalloh MI, Trevisan CD, Haas CJ. Hidradenitis Suppurativa and Peripheral Ulcerative Keratitis. Journal of community hospital internal medicine perspectives. 2024;14(6):89-93. doi:10.55729/2000-9666.1408. PMID:39839173; PMCID:PMC11745191.
Ghoraba HH, Or C, Ahluwalia A, Mekonnen B, Yasar C, Yavari N, et al. Subconjunctival dexamethasone implant (Ozurdex) for peripheral ulcerative keratitis. American journal of ophthalmology case reports. 2025;39:102379. doi:10.1016/j.ajoc.2025.102379. PMID:40686761; PMCID:PMC12274858.
Campagne O, Vinet E, Engel L, et al. Ocular manifestations of inflammatory bowel disease. Ocul Surf. 2023;29:326-339.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.