Interstitial keratitis (IK) is a non-ulcerative, non-suppurative inflammation of the corneal stroma1). It does not directly involve the epithelium or endothelium and is characterized primarily by lymphocytic infiltration and neovascularization of the stroma. It appears as a common final pathway of many corneal diseases; inflammation and vascular invasion lead to stromal scarring and vision loss.
The overall incidence of interstitial keratitis is rare, accounting for only 3% of all corneal transplants performed in the United States. In the US, HSV (herpes simplex virus) and syphilis account for more than 50% of cases.
Linear interstitial keratitis is an extremely rare subtype of IK, characterized by horizontal linear stromal infiltrates1). Only 14 cases have been reported in the literature since 19261). The etiology is unknown, but an autoimmune mechanism is suspected1).
QWhat are the causes of interstitial keratitis?
A
The causes of interstitial keratitis can be broadly divided into infectious and immune-mediated. Among infectious causes, HSV (herpes simplex virus) and syphilis are the most common, along with varicella-zoster virus (herpes zoster virus), tuberculosis, and Lyme disease. Known immune-mediated causes include Cogan syndrome, sarcoidosis, and hidradenitis suppurativa. Identifying the underlying disease is crucial for determining the treatment strategy, making a comprehensive systemic evaluation essential.
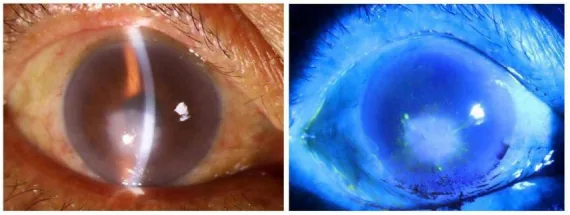
Jingjing Su, Ke Liu, Xiaofang Wu, Baotao Lin, et al. Case Report: Confocal microscopy in the early diagnosis of microsporidial keratitis 2026 Jan 15 Front Med (Lausanne).; 12:1745070 Figure 1. PMCID: PMC12852027. License: CC BY.
The left image is a slit-lamp view showing diffuse corneal stromal opacity and inflammatory findings. Fluorescein staining on the right shows no apparent epithelial defect, indicating that the lesion is primarily in the stroma.
Decreased visual acuity and blurred vision are the most common complaints. Marked photophobia and pain are characteristic. It may also be accompanied by conjunctival injection, foreign body sensation, and tearing.
Conjunctival injection: Ciliary injection is observed.
Corneal opacity: Presents with various patterns such as diffuse, fan-shaped, central, and circumferential.
Stromal neovascularization: Vascular invasion is observed in the deep stroma. In herpetic IK, it presents a “salmon patch” appearance4).
Corneal edema: May be accompanied by stromal and epithelial edema. In disciform keratitis, circular stromal edema with Descemet’s membrane folds is observed8).
Keratic precipitates: In herpetic disciform keratitis, small to medium-sized KP are seen in the center of the lesion8).
Quiescent Stage and Associated Findings
Ghost vessels: Remaining as collapsed vessels after regression of active-stage neovascularization. A characteristic finding of IK.
Corneal scar: A firm stromal opacity that develops after inflammation subsides, classified by severity as nebula, macula, or leucoma.
Lipid keratopathy: Deposition of cholesterol and phospholipids secondary to deep neovascularization. May appear as radial striae (steel wool keratopathy)4).
Decreased corneal sensation: In herpetic IK, decreased corneal sensation is important as an auxiliary diagnostic finding4)8).
Herpes stromal keratitis is one of the most common causes in developed countries. It is a condition in which the host immune response (delayed-type hypersensitivity) to HSV occurs in the corneal stroma8). The basic disease types are disciform keratitis and necrotizing keratitis8). Recurrent episodes lead to progression of vascular invasion and scar formation.
Syphilitic interstitial keratitis is caused by congenital syphilis in 90% of cases and develops in the early teens. Most cases are bilateral, and if untreated, it heals spontaneously over months to years but leaves severe scarring. In children with congenital syphilis, steroid-induced intraocular pressure elevation is a management issue2).
Cogan syndrome is a rare autoimmune vasculitis characterized by interstitial keratitis and vestibuloauditory dysfunction6). In a literature review of 55 pediatric cases, IK was found in 62% and uveitis in 36%6). Aortitis occurs in 16% and can lead to fatal cardiovascular complications6). Atypical Cogan syndrome may be associated with occlusive retinal vasculitis7).
Hidradenitis suppurativa (HS) has been reported as a rare cause of IK3). Ocular complications occur in 13.89% of HS patients, and IK is thought to be mediated by an autoimmune mechanism3). Some cases present with high titers of c-ANCA positivity3). Severe cases of HS-associated IK with progressive corneal thinning and ectasia leading to perforation have also been reported5).
Interstitial keratitis is a clinical diagnosis based on the findings of non-ulcerative stromal keratitis with deep stromal neovascularization. In addition to a comprehensive ophthalmic examination, systemic evaluation to identify the underlying disease is essential.
Syphilis serology (RPR/VDRL + FTA-ABS) should be performed in all cases of interstitial keratitis. This is because it is a treatable cause and accounts for a considerable number of cases.
Definitive diagnosis of herpetic IK is made by viral isolation, but this is difficult in practice8). Diagnosis is made by integrating the history of corneal herpes, recurrent nature, decreased corneal sensation, and detection of viral DNA by PCR8).
Anterior segment OCT (AS-OCT) is useful for evaluating interstitial keratitis. In non-infectious interstitial keratitis, it appears as a well-defined, localized hyperreflective lesion in the mid-stroma, sometimes accompanied by hyporeflective areas above and below reflecting edema. After treatment, the hyperreflective area becomes more compact, with corneal thinning and deep stromal hyperreflectivity (scarring) remaining as sequelae. Linear interstitial keratitis shows a hyperreflective area limited to the anterior stroma1). Confocal microscopy (IVCM) reveals hyperreflective needle-shaped structures and contributes to the assessment of stromal inflammation1).
When Cogan syndrome is suspected, hearing tests are essential6)7). Contrast-enhanced MRI may confirm labyrinthitis of the inner ear and assist in diagnosis6). Echocardiographic evaluation for aortitis is also recommended6).
Disease
Differential points
Infectious corneal ulcer
Epithelial defect with purulent infiltration
Corneal endothelial disease
Secondary stromal edema, endothelial findings
Traumatic corneal scar
History of trauma, no inflammatory findings
QWhat tests are needed for interstitial keratitis?
A
In interstitial keratitis, ophthalmologic examinations (slit-lamp microscopy, intraocular pressure measurement, corneal sensitivity testing) as well as investigation of underlying diseases are important. Syphilis serology is mandatory in all cases. When herpes is suspected, PCR detection of viral DNA serves as a supplementary diagnostic tool. When Cogan syndrome is suspected, hearing tests and echocardiography are recommended. AS-OCT and confocal microscopy are useful for detailed evaluation of stromal lesions.
Steroid eye drops: The mainstay of treatment for interstitial keratitis, effective for relieving acute symptoms and suppressing scarring and corneal neovascularization. In severe cases, treatment begins with potent steroids such as betamethasone and is tapered over a period of months8).
Acyclovir eye ointment: In herpetic IK, concomitant use with steroid eye drops is essential8). Using steroids alone without acyclovir eye ointment tends to cause recurrence and exacerbation8).
Tacrolimus eye drops: Tacrolimus 0.03% eye drops were effective in a pediatric case of syphilitic IK with steroid-induced intraocular pressure elevation2). The patient remained recurrence-free for approximately 3 years, and intraocular pressure was maintained within normal range2).
Corneal transplantation: Indicated when severe corneal scarring unresponsive to drug therapy remains. However, the risk of rejection is high due to a history of inflammation and neovascularization.
Management of perforation: In cases of corneal perforation due to HS-associated IK, conjunctival flap covering was performed when closure with cyanoacrylate adhesive was insufficient5).
Treatment of underlying disease: Systemic antibiotic therapy is essential for syphilis and should be actively performed independently of keratitis. In Cogan syndrome, biologic agents are considered in addition to systemic steroids6).
In herpetic interstitial keratitis, in addition to suppressing the immune response with steroid eye drops, concomitant use of acyclovir ophthalmic ointment is necessary. If treated with steroid eye drops alone without acyclovir ophthalmic ointment, recurrence and reactivation are likely.8)
QWhat should be noted in the treatment of interstitial keratitis?
A
The most important step is identifying and appropriately treating the underlying disease. In herpetic cases, steroid eye drops and acyclovir ophthalmic ointment must always be used together. Using steroids alone increases the risk of recurrence. In syphilitic cases, systemic antibiotic therapy is essential. Long-term steroid use requires monitoring for elevated intraocular pressure and cataracts, and particular attention to intraocular pressure management is needed in children. In Cogan syndrome, early systemic treatment is important to prevent irreversible hearing loss.
The pathophysiology of interstitial keratitis varies greatly depending on the cause.
Herpetic interstitial keratitis is a condition in which the host immune and inflammatory response to HSV occurs in the corneal stroma8). It differs from epithelial keratitis in that the immune response, rather than viral proliferation, is the main driver. Disciform keratitis is a condition in which circular stromal opacity and edema develop due to a delayed-type hypersensitivity reaction8). Necrotizing keratitis involves neutrophil infiltration in response to complexes of viral antigens and antibodies in the stroma, which has been repeatedly inflamed and invaded by blood vessels, resulting in denser corneal opacity8). Histologically, it shows lymphocytic interstitial infiltration without superficial ulceration and extensive neovascularization.
Syphilitic interstitial keratitis is considered an immune reaction to syphilis antigens within the corneal stroma. In congenital syphilis, the pathogen invades the cornea, but the inflammation is primarily an immune response rather than an active infectious symptom. While it responds well to steroid therapy, systemic treatment alone has limited effect on corneal inflammation.
The pathogenesis of Cogan syndrome is suggested to involve DEP-1/CD148 autoantibodies6). DEP-1/CD148 is present in endothelial cells, neuronal/glial cells, and the inner ear, explaining the multi-organ involvement6). These antibodies show cross-reactivity with structural proteins of reovirus type III, suggesting that infection may trigger the onset6). In pediatric Cogan syndrome, systemic steroids achieved remission of ocular symptoms in 69% of cases, but hearing impairment remained as severe or complete hearing loss in 56%6).
In hidradenitis suppurativa (HS)-associated IK, inflammatory cytokines such as TNF-α and IFN-γ are thought to trigger corneal stromal inflammation5). In HS-associated IK, progressive ectasia (corneal dilation) can occur and may lead to perforation, even in the absence of corneal ulceration5).
Imaging findings of linear interstitial keratitis have been described in detail using AS-OCT and IVCM1). AS-OCT reveals hyperreflective areas localized to the anterior stroma, and IVCM shows hyperreflective needle-shaped structures throughout the full thickness of the stroma1). Cases have been reported for the first time in patients with a history of LASIK, and this condition should be recognized as a differential diagnosis after refractive surgery1).
Tacrolimus eye drops are attracting attention as a new treatment option for syphilitic IK2). In pediatric cases where long-term steroid use was difficult due to steroid-induced intraocular pressure elevation, tacrolimus 0.03% eye drops were effective in preventing recurrence and maintaining normal intraocular pressure for approximately three years2). Stronger therapeutic effects than cyclosporine eye drops have been reported2).
The association between hidradenitis suppurativa and IK has become increasingly recognized3)5). HS-associated IK responds to systemic immunosuppression including adalimumab, but has a tendency to recur and requires long-term management5).
In the management of obstructive retinal vasculitis in atypical Cogan syndrome, retinal photocoagulation of non-perfused areas is necessary, but cases have been reported where pattern scan laser resulted in insufficient coagulation effect and development of retinal neovascularization7). Even in the absence of subjective auditory symptoms, if IK is accompanied by systemic inflammation, Cogan syndrome should be suspected and hearing tests should be performed7).
In Cogan syndrome, ocular and auditory symptoms are often separated by a time lag. In atypical cases, the interval may be more than 2 years, making early diagnosis difficult. However, because the prognosis for hearing impairment is poor, systemic treatment should be initiated promptly when Cogan syndrome is suspected.6)
Barrientos LC, Wildes M. Linear Interstitial Keratitis: A Report of Two Cases and Review of Literature. Cureus. 2025;17(3):e80985. doi:10.7759/cureus.80985. PMID:40260341; PMCID:PMC12010693.
Martin J, Kopplin L, Costakos D. Syphilitic interstitial keratitis treated with topical tacrolimus. American journal of ophthalmology case reports. 2021;23:101175. doi:10.1016/j.ajoc.2021.101175. PMID:34368498; PMCID:PMC8326179.
Lyle K, Zimmer JL, Gillette WM, Recko MS. Interstitial keratitis presenting as the ocular manifestation of undiagnosed hidradenitis suppurativa. Proc (Bayl Univ Med Cent). 2024;37(3):479-481.
Ullman MA, Martinez CE, Margolis TP. A “shining” example of interstitial keratitis. Am J Ophthalmol Case Rep. 2021;21:101006.
Quigley C, Butler T, Murphy C, Power W. Perforation in interstitial keratitis associated with hidradenitis suppurativa: medical and surgical management. BMJ case reports. 2023;16(1). doi:10.1136/bcr-2022-251928. PMID:36707098; PMCID:PMC9884907.
Rücklová K, von Kalle T, Koitschev A, Gekeler K, Scheltdorf M, Heinkele A, et al. Paediatric Cogan´s syndrome - review of literature, case report and practical approach to diagnosis and management. Pediatric rheumatology online journal. 2023;21(1):54. doi:10.1186/s12969-023-00830-x. PMID:37291629; PMCID:PMC10251673.
Inokuchi C, Sato S, Terada M, Uematsu S, Shirai S. A Case of Bilateral Retinal Vasculitis in Atypical Cogan Syndrome. Cureus. 2024;16(8):e66984. doi:10.7759/cureus.66984. PMID:39280458; PMCID:PMC11402271.