Microsporidia are obligate intracellular spore-forming fungi. Previously classified as protozoa, genetic analysis has reclassified them as highly specialized fungi that retain a mitochondrion-derived organelle (mitosome). About 1200 species are known, of which 15 are involved in human infection.
Ocular infections present two distinct clinical forms. Keratoconjunctivitis is more common in immunocompromised patients, especially those with HIV/AIDS and low CD4+ T-cell counts. Stromal keratitis is characteristic of infection in immunocompetent individuals.
In a study of 4822 cases of microbial keratitis in India, 19 cases (0.4%) were microsporidial keratitis. Reports are increasing, mainly in Southeast Asia. In Japan, cases have been reported during temporary returns from Southeast Asia, as well as cases without travel history triggered by soil contamination. In recent years, water exposure-related case clusters have also been reported in the United States 2).
QCan microsporidial keratitis occur in immunocompetent individuals?
A
Yes, it can occur in immunocompetent individuals. In immunocompetent patients, it mainly presents as stromal keratitis, with risk factors including water exposure, soil exposure, contact lens wear, and post-corneal surgery. In recent years, reports in immunocompetent individuals have been increasing worldwide.
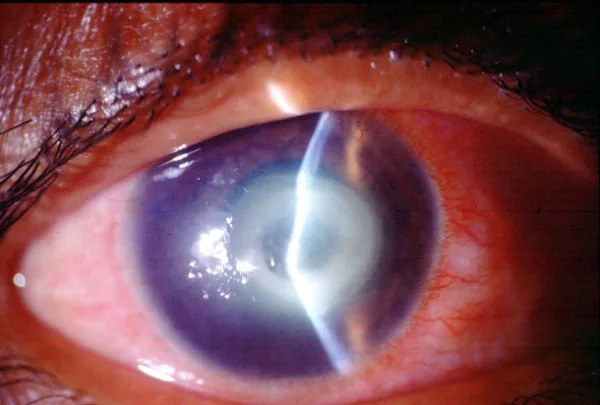
Geeta K Vemuganti, Prashant Garg, Savitri Sharma, Joveeta Joseph, et al. Is Microsporidial keratitis an emerging cause of stromal keratitis? – a case series study 2005 Aug 17 BMC Ophthalmol. 2005 Aug 17; 5:19 Figure 2. PMCID: PMC1200253. License: CC BY.
A large white infiltrate in the central corneal stroma with marked conjunctival hyperemia. This is a clinical picture of microsporidial keratitis showing a central dominant infiltrative lesion.
Hyperemia, foreign body sensation, photophobia, and decreased visual acuity are the main complaints. In the keratoconjunctivitis type, symptoms may be limited to mild irritation 5). In the stromal keratitis type, symptoms progress slowly, and it is not uncommon for patients to take several months to over a year from onset to consultation 6).
The clinical picture differs greatly between the keratoconjunctivitis type and the stromal keratitis type.
Keratoconjunctivitis type
Multiple punctate epithelial lesions: Coarse, raised, round to oval epithelial lesions appear multifocally 1). They show variable staining with fluorescein.
Non-suppurative conjunctivitis: Accompanied by mild to moderate conjunctival hyperemia, with papillary or follicular reactions.
Subepithelial infiltrates: May progress to nummular or disciform lesions 1).
Stromal keratitis type
Multifocal granular infiltrates: White fine granular infiltrates scattered in the corneal stroma. They may have a crystalline appearance 7).
Slow progression: Lesions gradually enlarge and coalesce, progressing centripetally toward the center 7).
Corneal edema and Descemet’s folds: May be accompanied by stromal edema and keratic precipitates 1).
Multiple granular infiltrates within the corneal epithelium are characteristic of this disease, and differentiation from multiple corneal subepithelial infiltrates due to adenovirus is important. If multiple granular infiltrates within the corneal epithelium are found in a patient with a history of travel to Southeast Asia, this disease should be considered and epithelial debridement performed.
In patients with keratoconjunctivitis, cases have been reported where immune-mediated corneal endotheliitis occurred after the resolution of epithelial keratitis 1). Twelve days after the initial visit, a sudden decrease in visual acuity (20/400), corneal edema, and diffuse corneal endothelial deposits appeared, which rapidly improved with steroid eye drops.
Immunodeficiency: HIV/AIDS (especially CD4-positive T cell count <100/mm³) is the greatest risk factor.
Water exposure: Freshwater lakes, ponds, hot springs, swimming pools. Among 15 cases in the US, 10 had a history of environmental exposure, including scuba diving in lakes, duck hunting in marshes, and swimming in freshwater pools 2).
Post-corneal surgery: Cases have been reported after Trans-PRK 6), LASIK, and corneal transplantation 7).
Steroid use: In addition to topical steroid eye drops, intravitreal steroid injections can also be a risk factor 5).
Contact lens wear: Increased contact with contaminated water is involved.
Exposure to soil/mud: Cases have also been reported from sports such as rugby.
QWhat environmental exposures are risk factors?
A
Exposure to freshwater lakes, ponds, rivers, hot springs, and swimming pools is an important risk factor. In a case series from Georgia, USA, 10 out of 15 cases had a history of water exposure such as swimming in lakes, activities in swamps, or use of well water 2). Contact with soil or mud is also a risk.
Microsporidial keratitis is suspected when culture-negative keratitis does not respond to conventional antibacterial treatment 3). Detection of spores is essential for definitive diagnosis.
Staining of corneal scrapings is the basis of diagnosis. It is desirable to combine smear microscopy and culture to identify the causative organism. Testing is recommended before administration of antimicrobial agents.
The main staining methods useful for detecting spores are shown below.
Staining Method
Spore Staining Appearance
Characteristics
Modified Ziehl-Neelsen
Red
Clear against acidic background
Calcofluor white
Green fluorescence
Targets chitin wall
Chromotrope 2R
Bright red
Septate structures also visible
Other stains used include Gram stain (positive), Giemsa stain, peripheral iris anterior synechiae stain, and KOH direct microscopy 6). On histopathology, Masson’s trichrome stain can identify red spores 6).
In vivo confocal microscopy (IVCM) is useful as a non-invasive diagnostic aid. Characteristic findings include numerous hyperreflective oval structures approximately 5 µm in diameter scattered within the corneal stroma7). It is also used for pathogen detection before surgery 7) and for monitoring treatment response 3).
PCR testing: Species-specific PCR can identify Encephalitozoon species at the molecular level. However, PCR can also detect DNA from dead organisms, so caution is needed in interpreting results.
Transmission electron microscopy (TEM): This is the gold standard for identifying microsporidia, but it is costly, time-consuming, and not suitable for routine diagnosis.
Corneal biopsy: Considered when cultures are negative and there is no response to empirical treatment 3). Sampling from the edge of the infiltrate increases the detection rate of viable pathogens 8).
Microsporidia are obligate intracellular parasites and do not grow in standard culture media, so culture tests are typically negative 7).
QWhat is the most effective test for confirming the diagnosis of microsporidial keratitis?
A
Detection of spores by special staining (e.g., modified Ziehl-Neelsen, calcofluor white) of corneal scrapings or corneal biopsy tissue is necessary for definitive diagnosis. Confocal microscopy can noninvasively detect spore-like structures and is useful as a diagnostic aid 7). Transmission electron microscopy is the gold standard but is not practical for routine diagnosis.
There are no established guidelines for microsporidial keratitis, and treatment is based on the type and severity of the disease.
Treatment of Epithelial Type
Epithelial debridement: Serves both diagnostic and therapeutic purposes. It physically removes spores within the epithelium.
Voriconazole 1-2% eye drops: High efficacy has been reported with monotherapy 2). Activity resolved in all cases after an average of about 40 days 2).
Fluoroquinolone eye drops: Monotherapy with moxifloxacin, etc., is also effective, with resolution reported in 99% of cases.
Observation: Spontaneous resolution may occur in immunocompetent individuals.
Treatment of Stromal Type
Voriconazole eye drops + oral albendazole: Complete resolution of stromal opacity has been reported with 4 weeks of combination therapy 3).
PHMB + chlorhexidine + fluconazole: Resolution was achieved with triple therapy of PHMB 0.04%, chlorhexidine 0.04%, and fluconazole 0.3% 4).
Fumagillin eye drops: Starting at 2 mg/mL and tapering over 2 years resulted in cure without recurrence 7).
Therapeutic keratoplasty: Performed in cases unresponsive to medical therapy. Both PKP and DALK have been reported 6)7).
Stromal microsporidial keratitis is often treatment-resistant. In a large case series, 25 of 34 cases (73.5%) required keratoplasty 4). However, in recent years, cases cured with conservative medical therapy alone have been accumulating 3)4). If the lesion progresses slowly and there are no ocular complications, continuing medical therapy patiently is also an option 4).
It has been suggested that epithelial debridement may promote drug penetration and contribute to healing not only in the epithelial type but also in the stromal type 4).
QCan microsporidial stromal keratitis be cured with medication alone?
A
Several cases of cure with medication alone have been reported. There are cases of cure with voriconazole eye drops plus oral albendazole 3) and with PHMB plus chlorhexidine plus fluconazole plus oral albendazole 4). However, in large case series, approximately 74% required corneal transplantation, and many cases are refractory to medication.
Microsporidial infection occurs through spores that are resistant to environmental conditions. The size of spores is minute, ranging from 1 to 4 µm depending on the species.
Invasion of host cells involves the polar tubule, which is unique to microsporidia. Changes in osmotic pressure within the spore cause the polar tubule to evert and extend, penetrating the adjacent host cell membrane. The spore contents (sporoplasm) are injected into the host cytoplasm through the polar tubule.
Once inside the host cell, microsporidia proliferate intracellularly and fill the cytoplasm. When spores mature, the host cell lyses, releasing new spores into the surroundings. The released spores spread to adjacent cells or the external environment, expanding the infection.
The route of infection to the ocular surface is not fully understood. Direct contact with contaminated water and traumatic inoculation to the ocular surface are suspected. Microsporidia may remain latent within the host and reactivate during immunosuppression. Transmission after transplantation via donor cornea has also been reported.
Host defense against microsporidial infection involves both cellular and humoral immunity 5). Local use of steroids (including not only eye drops but also intravitreal injections) suppresses local immunity and may promote the development of microsporidial keratitis as an opportunistic infection 5). Cyclosporine has also been shown experimentally to modify the immune response to microsporidia 5).
In the stromal keratitis type, numerous spores are present between the collagen lamellae of the corneal stroma, and slightly smaller structures are also observed within keratocytes 3). The inflammatory reaction is relatively mild, reflecting the slowly progressive nature of the disease.
Evidence on the diagnosis and treatment of microsporidial keratitis is mainly based on case reports and small case series, with no large-scale prospective studies. Notable recent findings are presented below.
Huang AS et al. (2021) reported 15 cases of microsporidial keratitis accumulated over 10 years in the state of Georgia, USA 2). All cases were immunocompetent individuals, and a history of freshwater exposure was confirmed in 10 cases. Monotherapy with 1-2% voriconazole eye drops resulted in resolution of activity in all cases, with a mean treatment duration of 40.1 ± 17.1 days.
Spena et al. (2023) reported three cases of microsporidial stromal keratitis that developed after corneal transplantation 7). All cases were initially diagnosed as herpetic keratitis. In vivo confocal microscopy was useful for preoperative pathogen detection, and therapeutic corneal transplantation combined with fumagillin eye drops (2 mg/mL, high-dose initiation and long-term taper) led to cure without recurrence.
Raghavan et al. (2022) achieved complete resolution in a case of stromal microsporidial keratitis treated with steroids for 9 months, using a triple combination of PHMB 0.04% + chlorhexidine 0.04% + fluconazole 0.3% and oral albendazole 4). They suggested that enhanced drug penetration via epithelial debridement may have contributed to healing.
Future challenges include standardizing the optimal concentration and duration of voriconazole monotherapy, establishing noninvasive diagnostic protocols using confocal microscopy, and elucidating the epidemiological association between environmental factors including water exposure and disease onset. Given the reclassification of microsporidia as fungi, systematic evaluation of antifungal efficacy is also required.
Chandran K, Tendolkar S, Kalra P, Murthy SI. Rare presentation of sequential epithelial microsporidiosis and endotheliitis. BMJ case reports. 2021;14(4). doi:10.1136/bcr-2020-237490. PMID:33795265; PMCID:PMC8023631.
Huang AS, Cho JS, Bertram BA. Microsporidial Keratitis Related to Water Exposure: A Case Series. Cureus. 2021;13(6):e15760. doi:10.7759/cureus.15760. PMID:34164251; PMCID:PMC8214417.
Donovan CP, Margo CE, Espana EM. Stromal microsporidial keratitis successfully treated with medical therapy. American journal of ophthalmology case reports. 2021;23:101178. doi:10.1016/j.ajoc.2021.101178. PMID:34368500; PMCID:PMC8326187.
Raghavan A, Raja DR, Venkatapathy N, Rammohan R. A case of stromal microsporidiosis: medical strategies employed for successful resolution. BMJ case reports. 2022;15(2). doi:10.1136/bcr-2021-246233. PMID:35165126; PMCID:PMC8845186.
Chou TY, Bansal J, Seidman R, et al. Bilateral microsporidial keratoconjunctivitis in a clinically healthy female receiving intravitreal steroid injections: associations and potential risk factors. Am J Ophthalmol Case Rep. 2022;27:101659.
Alabduljabbar M, Sirajuddin F, Maktabi A, AlShabeeb R. A Rare Microsporidial Infection in Lamellar Corneal Tissue, following Transepithelial Photorefractive Keratectomy. Case reports in ophthalmology. 2023;14(1):127-133. doi:10.1159/000528894. PMID:37034379; PMCID:PMC10074259.
Spena R, Bovone C, Ciarmatori N, Pellegrini M, Yu AC, Zauli G, et al. Microsporidial Stromal Keratitis in Post-Keratoplasty Eyes. Journal of clinical medicine. 2023;12(11). doi:10.3390/jcm12113706. PMID:37297901; PMCID:PMC10253265.
American Academy of Ophthalmology. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P95-P198.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.