Conjunctivitis is a general term for inflammation of the conjunctiva. It is characterized by hyperemia and edema due to dilation of conjunctival vessels, and is usually accompanied by discharge. The prevalence varies depending on cause, age, and season.
Conjunctivitis is broadly classified into infectious and non-infectious types.
Infectious: Viruses, bacteria, and Chlamydia are the representative pathogens. Approximately 80% of infectious conjunctivitis in adults is viral, followed by bacterial. In children, bacterial and viral conjunctivitis occur at nearly equal rates.
Non-infectious: Allergic conjunctivitis is the most common, affecting 15–40% of the population. Some cases are secondary to drug toxicity or systemic diseases such as sarcoidosis.
In recent years, conjunctivitis has gained attention as an ocular manifestation of COVID-19. The overall incidence of conjunctivitis among hospitalized patients is approximately 5.9%, rising to 12.7% in severe cases4).
QIs Conjunctivitis Contagious?
A
Infectious conjunctivitis (viral and bacterial) is transmitted to others through contact. In particular, adenovirus has a high transmission risk of 10–50%. In contrast, allergic conjunctivitis is non-infectious and does not spread. See Causes and Risk Factors for details.
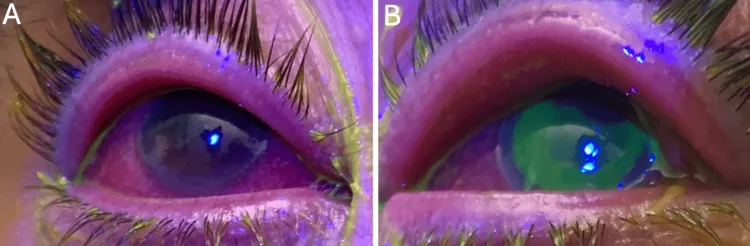
Sinan Albear, Stephen LoBue, Ayorinde Cooley, Traeson Brandenburg, et al. Povidone-Iodine as an Adjuvant Therapy for Refractory Gonorrhea Keratoconjunctivitis: A Case Report 2025 May 7 Cureus.; 17(5):e83676 Figure 2. PMCID: PMC12143893. License: CC BY.
A shows diffuse superficial punctate keratopathy of the right cornea under fluorescein staining. B shows a large epithelial defect in the left eye, with both eyes exhibiting conjunctival hyperemia and eyelid swelling.
The main subjective symptoms common to conjunctivitis are as follows.
Foreign body sensation: Caused by corneal epithelial damage or mechanical irritation of conjunctival papillae. It is seen in both infectious and non-infectious types.
Hyperemia: Due to dilation of conjunctival vessels. It is the most frequent finding.
Discharge: Its characteristics vary depending on the cause (described below).
Lacrimation: Due to increased reflex tear secretion. It is also associated with pain from epithelial damage.
Itching: The most characteristic symptom of allergic conjunctival disease (ACD). It is caused by histamine released from mast cells stimulating trigeminal C fibers.
The characteristics of ocular discharge serve as important clues for identifying the cause.
No follicles or papillae: Characteristic of staphylococcal conjunctivitis.
Follicular
Conjunctival follicles: Lymphoid follicles composed primarily of B cells. Commonly occur in the inferior palpebral fornix.
Serous discharge: Characteristic of viral conjunctivitis.
Preauricular lymphadenopathy: Observed in adenovirus and chlamydial infections.
Suppurative
Profuse purulent discharge: Yellow, cream-like discharge overflowing from the palpebral fissure.
Eyelid swelling and chemosis: Reflects severe inflammation.
Risk of corneal perforation: Unique to gonococcal conjunctivitis.
Other important findings:
Conjunctival papillae: Arise in various chronic inflammatory conditions. Those 1 mm or more in diameter are called giant papillae, typically seen in vernal keratoconjunctivitis and contact lens‑related giant papillary conjunctivitis. On slit‑lamp examination, papillae are distinguished from follicles by vessels spreading from the center, whereas follicles have vessels around their periphery.
Conjunctival hemorrhage: Characteristic as hemorrhagic patches in enteroviral conjunctivitis. Rarely seen in ACD.
Chemosis: Caused by leakage of plasma components. Common in ACD but also occurs in acute infections.
Pseudomembrane: Coagulation of fibrin and neutrophils into a membranous form due to intense inflammation. Common in adenoviral conjunctivitis, especially in infants. In infants, the immature epithelial structure causes the entire infected epithelium to slough off, resulting in minimal bleeding upon removal. In adults, removal causes bleeding.
Conjunctival scarring: Occurs irreversibly as a sequela of inflammation. Severe cases may progress to symblepharon.
Multiple subepithelial infiltrates (MSI): Punctate infiltrates appearing in the superficial corneal layer 5–10 days after the onset of EKC. A characteristic finding of EKC.
Differentiation between conjunctival and ciliary injection: Conjunctival injection is most intense in the fornix and weakens toward the limbus, appearing bright red in the superficial layer. Ciliary injection is most intense at the limbus and appears purplish-red in the deep layer.
COVID-19-associated conjunctivitis presents with follicular reaction, conjunctival edema, and serous discharge3). Pseudomembranous inflammation and subconjunctival hemorrhage have also been reported3).
QCan the cause be determined by the color of eye discharge?
A
The characteristics of discharge aid in identifying the suspected cause. Large amounts of yellow creamy purulent discharge suggest gonococcus; yellowish-white seropurulent discharge suggests pneumococcus or Haemophilus influenzae; serofibrinous discharge suggests adenovirus. However, microbiological testing is necessary for definitive diagnosis.
Haemophilus influenzae, Streptococcus pneumoniae, Moraxella species
Adults
Staphylococcus species
Elderly
Staphylococcus species, Streptococcus pneumoniae, Corynebacterium species
In recent years, drug-resistant bacteria such as methicillin-resistant Staphylococcus aureus (MRSA), penicillin-resistant Streptococcus pneumoniae (PRSP), and drug-resistant Haemophilus influenzae (BLNAR) have been increasing, and some cases of conjunctivitis have become refractory to treatment.
Neisseria gonorrhoeae is the only bacterium capable of infecting intact corneal epithelium, and inflammation extending to the cornea can lead to perforation. In adults, it presents as a sexually transmitted infection. The proportion of fluoroquinolone-resistant N. gonorrhoeae has been reported to exceed 80% in Japan2).
The representative viruses that cause conjunctivitis fall into the following three groups.
Adenovirus: Accounts for 65–90% of viruses causing conjunctivitis. There are two clinical forms: epidemic keratoconjunctivitis (EKC) and pharyngoconjunctival fever (PCF). The main causative viruses of EKC are the new D species types 54, 56, and 64. PCF is caused by adenovirus types 3, 4, and 7.
Enterovirus: Causes acute hemorrhagic conjunctivitis (AHC). Includes enterovirus type 70 (EV70) and coxsackievirus A24 variant (CA24v). The incubation period is short, ranging from half a day to one day. It resolves within about one week without sequelae.
Herpesvirus: Herpes simplex virus (HSV) accounts for 1.3–4.8% of all acute conjunctivitis cases. It is usually unilateral. The presence of periocular vesicles and keratitis is important for differential diagnosis.
Conjunctivitis caused by Chlamydia trachomatis is broadly classified into trachoma and inclusion conjunctivitis. What is currently seen in Japan is inclusion conjunctivitis, which is one of the sexually transmitted conjunctival infections. Chlamydial infection should be suspected in prolonged follicular conjunctivitis that does not respond to antibiotics (the follicles become giant). Chlamydia can only replicate intracellularly, and treatment requires a long duration.
This is a type I allergic reaction to transient allergens (e.g., pollen) or persistent allergens (e.g., house dust mites). A history of current or past atopic diseases (eczema, asthma, urticaria, rhinitis) is a risk factor. It is more common from spring to summer.
Neonatal conjunctivitis is primarily caused by birth canal infection (vertical transmission). The causative microorganism and the time to onset show characteristic patterns. N. gonorrhoeae presents at 1–3 days after birth, Chlamydia at 3–10 days, and Moraxella at 7–10 days or later. Gonococcal conjunctivitis carries a high risk of corneal perforation.
In Japan, neonatal ocular prophylaxis with fluoroquinolone eye drops is performed, but breakthrough infections due to fluoroquinolone-resistant gonococcus have been reported2).
Conjunctival hyperemia can occur as a partial symptom of systemic infections. It is seen in measles, rubella, Kawasaki disease, dengue fever, etc., and does not require eye drop treatment. In Kawasaki disease, bilateral non-suppurative conjunctivitis (sparing the limbus) is one of the diagnostic criteria7).
Conjunctivitis is the most common ocular symptom of COVID-196). ACE-2 receptors for SARS-CoV-2 are expressed in the cornea and conjunctiva, making the ocular surface a potential infection target3). Cases have also been reported where conjunctivitis appears as the only symptom of COVID-193).
QDo Contact Lenses Increase the Risk of Conjunctivitis?
A
Contact lens wear can cause giant papillary conjunctivitis (CL-GPC). Constant contact and friction between the lens and the upper tarsal conjunctiva leads to inflammation and giant papillae. In addition, contamination of lenses or storage solution poses a risk of infectious conjunctivitis, making proper lens care important.
Microbiological examination to detect causative microorganisms is key to diagnosis8).
Smear microscopy: Examination of smear specimens of discharge or conjunctival scrapings.
Giemsa staining: Multipurpose screening stain. With the rapid stain Diff-Quick®, staining results nearly equivalent to conventional methods can be obtained in 15 seconds8). All microorganisms stain blue.
Gram staining: Differentiates between gram-positive and gram-negative bacteria. With the rapid kit Favor G®, staining is possible in 3 minutes8).
Culture and isolation: Identification of causative bacteria and antimicrobial susceptibility testing is possible. Specimens should be collected using a swab with transport medium and promptly submitted for culture. Refrigerated storage is recommended. However, the causative organism is detected in only about half of bacterial conjunctivitis cases. Culture is recommended for neonates, recurrent cases, treatment-resistant cases, and suspected gonococcal infection.
Adenovirus antigen detection kit: Rapid diagnosis using immunochromatography (Adenocheck®, Capilia® Adeno Eye). Sensitivity is approximately 80%, and attention to false negatives is necessary. Minimally invasive kits using tear fluid as a specimen are also available.
Allerwatch® Tear IgE: Measures total tear IgE levels using immunochromatography. Specificity is nearly 100%. Sensitivity varies by severity, at approximately 60% for allergic conjunctivitis and approximately 90% for vernal keratoconjunctivitis.
Eosinophil staining (such as Eosinostain®): If eosinophils are demonstrated in conjunctival secretions, allergic conjunctival disease (ACD) can be diagnosed.
Chlamydia is diagnosed by fluorescent antibody testing or PCR of conjunctival scrapings. If a diagnosis of chlamydial infection has already been made in another department, there is no need for repeat testing in ophthalmology. Fluorescent antibody testing and PCR are useful for herpes simplex virus, but because asymptomatic shedding in tear fluid can occur, a positive result may not reflect pathogenicity.
Treatment for conjunctivitis is selected according to the underlying cause. Determining the treatment approach based on an accurate diagnosis is fundamental.
Empiric therapy is initiated as the initial treatment, and the medication is changed based on culture results.
Adults: Fluoroquinolones (e.g., levofloxacin, gatifloxacin, moxifloxacin) or cephalosporin antibacterial eye drops are selected, keeping staphylococci in mind. Instill 3–4 times daily.
Children: Cephalosporins or macrolides are selected, targeting Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella. Among fluoroquinolones, tosufloxacin (OzeX®·Tosuflo®) has pediatric insurance coverage in Japan.
Neonates: The beta-lactam cefmenoxime (Bestron® ophthalmic solution 0.5%) is the first-line choice. Instill 5 times daily.
The effect of antibacterial eye drops usually appears within a few days, and healing occurs in approximately one week. If symptoms persist, consider the possibility of resistant bacteria, chlamydial infection, allergic conjunctivitis, or canaliculitis.
Gonococcal conjunctivitis: Often shows resistance to fluoroquinolones. Cephalosporins are selected as first-line treatment, but for multidrug-resistant gonococcus, intravenous ceftriaxone (Rocephin®) is used in combination2).
MRSA: Ofloxacin ophthalmic solution (Ofusaron®), vancomycin ophthalmic ointment, or Arbekacin® self-compounded eye drops (1 ampule dissolved in 20 mL saline) are used.
Moraxella conjunctivitis: Most antibacterial drugs are usually effective. Fluoroquinolone eye drops 3 times daily. For blepharitis/angular conjunctivitis, eye ointment 2 times daily.
Neonates: Ofloxacin (Tarivid®) 0.3% eye ointment 5 times daily for approximately 8 weeks. For severe cases or when systemic symptoms are present, combine with azithromycin (Zithromax® pediatric fine granules 10%) 10 mg/kg once daily for 3 days.
Adults: Long-term topical treatment plus oral administration of azithromycin or doxycycline.
Adenovirus: No effective antiviral drug currently exists. Antibacterial eye drops for secondary infection prevention and nonsteroidal anti-inflammatory eye drops are used. Steroid eye drops are effective for MSI. Infection prevention measures (hand washing, instrument disinfection, examination room cleaning) are most important.
Herpetic conjunctivitis: Acyclovir (Zovirax®) eye ointment 5 times daily. For herpes zoster, systemic antiviral therapy is administered, so topical treatment is usually unnecessary for conjunctivitis alone.
Acute hemorrhagic conjunctivitis: No specific treatment exists; only antibacterial eye drops for secondary infection prevention. Heals without sequelae in approximately 1 week.
Treatment of the underlying disease is fundamental. Steroid eye drops (dexamethasone 4–6 times daily or fluorometholone 3 times daily) are used for conjunctival inflammation. Pseudomembranes are carefully removed with forceps when they cause corneal epithelial damage. Care should be taken to minimize conjunctival invasion and bleeding. In ligneous conjunctivitis, if tranexamic acid is involved, discontinuation leads to improvement5).
QIs an antibacterial agent necessary for viral conjunctivitis?
A
No effective antiviral drug exists for adenovirus. Antibacterial eye drops are sometimes used for secondary infection prevention, but routine use is not recommended. Most cases resolve spontaneously within 1–2 weeks. If MSI (multiple subepithelial infiltrates) appear, steroid eye drops are effective.
The conjunctiva is a thin, vascularized mucous membrane composed of non-keratinized stratified squamous epithelium that covers the inner surface of the eyelids and the anterior sclera. Mucin (MUC-5AC) secreted by conjunctival goblet cells contributes to tear film stability. Accessory lacrimal glands (glands of Krause and Wolfring) are scattered in the lamina propria and secrete tear fluid.
Bacterial: Caused by abnormal proliferation of the normal conjunctival flora or direct external infection. Bacteria infiltrate the conjunctival epithelium and sometimes the lamina propria. Gonococci adhere to mucosal epithelial cells via pili and outer membrane proteins and can invade healthy corneal epithelium. Lipooligosaccharide (LOS) in the outer cell wall acts as an endotoxin.
Viral (adenovirus): Highly contagious, with an incubation period of 5–12 days and an infectious period of 10–14 days. Inflammation is predominantly lymphocytic and characterized by follicular reaction. In EKC, MSI appears in the subepithelial cornea as an immune response.
Chlamydia: Elementary bodies invade host cells and transform into reticulate bodies for replication. They then revert to elementary bodies and are released extracellularly. Since treatment drugs are effective only against reticulate bodies, long-term treatment is required for elimination of elementary bodies.
Type I allergic reaction is fundamental. When allergens crosslink surface IgE receptors, conjunctival mast cells are activated, releasing histamine, leukotrienes, prostaglandins, and cytokines. These increase vascular permeability, causing edema and infiltration of eosinophils and neutrophils.
Mechanisms of Pseudomembranous and Ligneous Conjunctivitis
A pseudomembrane is a membranous substance composed of fibrin, neutrophils, and exudate, formed on the conjunctival surface due to intense inflammation. Ligneous conjunctivitis is caused by type I plasminogen deficiency due to recessive mutations in the PLG gene5). Plasminogen is the precursor of plasmin, the main enzyme for fibrinolysis; its deficiency impairs fibrin removal from mucosal surfaces, leading to the formation of thick, woody pseudomembranes5).
SARS-CoV-2 uses the ACE-2 receptor to enter host cells. ACE-2 receptors are also expressed on the cornea and conjunctiva3), making the ocular surface a potential target for infection. It has also been suggested that the virus may be shed into the respiratory tract via the nasolacrimal duct3). The high frequency of conjunctivitis in severe COVID-19 may reflect the spillover of a systemic cytokine storm onto the ocular surface4).
In the phase 3 INVIGORATE trial (crossover, quadruple-blind) involving patients with seasonal allergic conjunctivitis, 0.25% reproxalap ophthalmic solution significantly improved itching score (mean difference −0.50, p < 0.001) and conjunctival hyperemia score (mean difference −0.14, p < 0.001) compared to vehicle1). Reproxalap is a drug with a novel mechanism of action that chemically captures reactive aldehyde species (RASP) and indirectly modulates upstream inflammatory cascades including NF-κB and the inflammasome1). Given that 45% of FDA adverse event reports for existing antihistamines cite “treatment failure,” it is expected as a new therapeutic option1).
Neonatal gonococcal conjunctivitis caused by fluoroquinolone-resistant Neisseria gonorrhoeae (levofloxacin MIC 12 μg/mL) has been reported from Japan2). It developed despite prophylactic levofloxacin eye drops and was cured with intravenous cefotaxime and oral azithromycin2). Whole-genome analysis confirmed missense mutations in the gyrA and parC genes2). Some European countries have reported no increase in gonococcal conjunctivitis after discontinuing routine neonatal ocular prophylaxis2), prompting recommendations for enhanced maternal screening and reconstruction of prevention strategies.
A meta-analysis of 11 studies involving 2,308 patients showed that the incidence of conjunctivitis was significantly higher in patients with severe COVID-19 (OR 2.4, 95% CI 1.4–4.0, p = 0.002)4). This association was confirmed in both Asian (OR 2.5) and European/Mediterranean (OR 2.3) populations4). Further prospective studies are needed to determine whether conjunctivitis can serve as a severity marker for COVID-19.
Treatment Developments for Ligneous Conjunctivitis
In a patient with late-onset ligneous conjunctivitis complicated by congenital hydrocephalus, temporary symptom resolution has been reported following a combination of tacrolimus 0.01% eye drops, 20% autologous serum, fresh frozen plasma (FFP) eye drops, and surgical excision5). Plasminogen eye drops and intravenous administration are available in some regions and are considered promising future treatment options5).
Starr CE, Nichols KK, Lang JR, Brady TC. The Phase 3 INVIGORATE Trial of Reproxalap in Patients with Seasonal Allergic Conjunctivitis. Clinical ophthalmology (Auckland, N.Z.). 2023;17:3867-3875. doi:10.2147/OPTH.S441009. PMID:38105911; PMCID:PMC10725700.
Mizushima H, Komori M, Yoshida CA, Miyairi I. Neonatal Gonococcal Conjunctivitis Caused by Fluoroquinolone-Resistant Neisseria gonorrhoeae. Emerging infectious diseases. 2025;31(10):2043-2045. doi:10.3201/eid3110.250895. PMID:41017068; PMCID:PMC12483108.
Ozturker ZK. Conjunctivitis as sole symptom of COVID-19: A case report and review of literature. Eur J Ophthalmol. 2020. doi:10.1177/1120672120946287.
Loffredo L, Fallarino A, Paraninfi A, Pacella F, Pacella E, Oliva A, et al. Different rates of conjunctivitis in COVID-19 eastern and western hospitalized patients: a meta-analysis. Internal and emergency medicine. 2022;17(3):925-928. doi:10.1007/s11739-021-02880-z. PMID:34750658; PMCID:PMC8575664.
Ghassemi H, Atighehchian M, Amoli FA. Delayed-onset ligneous conjunctivitis as a rare association with congenital hydrocephalous: a case report and review of the literature. Digital journal of ophthalmology : DJO. 2022;28(4):110-115. doi:10.5693/djo.02.2022.08.005. PMID:36660187; PMCID:PMC9838180.
Zou H, Zhang K, Chen X, Sha S. Vogt-Koyanagi-Harada disease after SARS-CoV-2 infection: Case report and literature review. Immunity, inflammation and disease. 2024;12(4):e1250. doi:10.1002/iid3.1250. PMID:38661242; PMCID:PMC11044218.
Wang W, Wang H, Wang H, Cheng J. Kawasaki disease with shock as the primary manifestation: How to distinguish from toxic shock syndrome?: A case report and literature review. Medicine. 2024;103(31):e39199. doi:10.1097/MD.0000000000039199. PMID:39093792; PMCID:PMC11296402.