Epidemic keratoconjunctivitis (EKC) is a highly contagious acute conjunctivitis caused by adenovirus (AdV) infection. It is commonly called “pink eye” or “hayari-me” in Japanese. In Japan, it is the most common epidemic disease in the field of ophthalmology, and it is also a public health concern in Asian countries1).
EKC was first reported by Fuchs in 1889 as “punctate superficial keratitis,” and the name “epidemic keratoconjunctivitis” came into use in 1938. In 1955, Jawetz et al. established a direct etiological relationship with adenovirus1). In Japan, at the 1959 symposium of the Japanese Ophthalmological Society, it was decided to use the term “epidemic keratoconjunctivitis” for epidemic keratoconjunctivitis1).
Initially, typical EKC was a clinical diagnosis when the triad of acute follicular conjunctivitis, corneal subepithelial opacities, and preauricular lymphadenopathy was present, and the cause was limited to AdV type 8. Subsequently, EKC caused by AdV types 19 and 37 of species D was also reported, and in recent years, epidemics caused by new types AdV 53, 54, 56, 64, and 85 have been confirmed1).
In Japan, the Infectious Disease Surveillance has been ongoing since 1981. EKC is a Category V infectious disease under the Infectious Diseases Law, reported from approximately 690 ophthalmology sentinel medical institutions nationwide1). Pharyngoconjunctival fever (PCF), also an adenoviral conjunctivitis, is reported from approximately 3,100 pediatric sentinel sites nationwide1).
According to the 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines, it is estimated that approximately 700,000 to 1.3 million people in Japan contract EKC annually1).
Due to general infection prevention measures such as hand hygiene and mask wearing associated with COVID-19 countermeasures, both EKC and PCF markedly decreased during the pandemic period from 2020 to 2022 1,2). In 2023, PCF resurged at approximately twice the normal scale, and EKC has also approached pre-pandemic levels 1).
A similar trend was confirmed in the Korean ophthalmology sentinel surveillance (2013–2022), where the annual incidence of EKC peaked at 22.5 per 1,000 people in 2018 and decreased to 4.0 in 2022 2). The weekly maximum incidence dropped from 49.7 in 2016 to 9.0 in 2022, but the seasonal pattern concentrated in August–September was maintained 2).
Globally, AdV8 is the main causative type of EKC, but detection of AdV8 has decreased since 1997, and AdV54 became the most frequently detected type from 2015 to 2019 1,18). AdV54 is a serotype with few international reports; AdV53, 56, and 64 have also been continuously detected, and a new type, AdV85, was discovered and reported after 2015 1,17).
By age, the highest rate is in children aged 0–6 years, decreasing in those aged 7–19 years and 20 years or older. Under the School Health and Safety Act Enforcement Regulations, it is classified as a Category 3 “other infectious disease” , and students are required to stay home until a physician determines there is no risk of infection. Although there is no clear regulation on the number of days, approximately two weeks is generally considered the guideline.
QHow contagious is pink eye?
A
It is highly contagious. Adenovirus can remain infectious for more than 10 days even in dry environments, and can cause nosocomial infections via healthcare workers’ hands, tonometer tips, or contaminated eye drop bottles. Intrafamilial infection is also common, and the 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines includes a history of intrafamilial infection as one of the auxiliary findings for clinical diagnostic criteria. Since infectivity persists for about two weeks after onset, i.e., until clinical findings resolve, it is necessary to refrain from attending school or work until eye discharge and redness disappear.
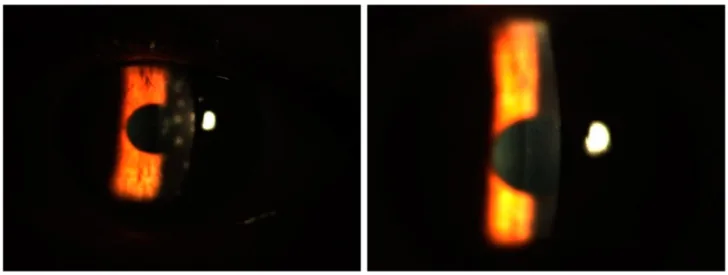
Karaca EE, Çelik G, İdacı Koç Ş, Evren Kemer Ö. Evaluating the Efficacy of Topical Tacrolimus Alone and in Combination with Prednisolone for Treating Subepithelial Infiltrates in Epidemic Keratoconjunctivitis. Biomedicines. 2025;13(4):895. Figure 5. doi:10.3390/biomedicines13040895. PMCID: PMC12024548. License: CC BY 4.0.
Before treatment (left), multiple subepithelial infiltrates (SEI) are scattered in the cornea; after three months of tacrolimus monotherapy (right), they have resolved. This corresponds to the course of corneal lesions in adenoviral keratoconjunctivitis discussed in section “2. Main symptoms and clinical findings.”
The incubation period is 7–14 days1). Typically, it first develops in one eye, and after a few days, the other eye becomes infected, often resulting in bilateral involvement. Simultaneous bilateral onset occurs in about 10–20% of cases 1).
Serofibrinous discharge (watery, giving the appearance of “conjunctivitis with little discharge”)
Foreign body sensation
Photophobia and decreased vision after the appearance of MSI
A characteristic feature is more severe eyelid swelling compared to bacterial conjunctivitis. The discharge is serofibrinous, which helps differentiate it from bacterial conjunctivitis that presents with mucopurulent discharge1). Clinical symptoms peak around 5 to 8 days after onset and then subside.
Clinical Findings (Findings Confirmed by Physician Examination)
EKC is characterized by the following three major features1).
Follicular conjunctivitis: Follicles form on the lower palpebral conjunctiva and fornix
Multiple subepithelial infiltrates (MSI) appearing around one week after onset
Swelling and tenderness of the preauricular lymph nodes
However, these three signs do not always appear simultaneously. In many cases, AdV conjunctivitis is suspected based on relatively severe follicular conjunctivitis, and typical findings accumulate during the course, leading to a diagnosis of EKC1).
Marked hyperemia is observed in the palpebral and bulbar conjunctiva. Follicles on the palpebral conjunctiva are the most important finding for diagnosing “follicular conjunctivitis,” but severe conjunctival hyperemia and edema may make it difficult to detect follicles1). In the early stage, petechiae (small hemorrhages) may be seen on the upper palpebral conjunctiva, which has high diagnostic value1).
Pseudomembranous conjunctivitis and severe disease
In severe cases, a pseudomembrane may form on the palpebral conjunctiva several days after onset, a condition called pseudomembranous conjunctivitis1). When a pseudomembrane forms, the discharge takes on a mucopurulent appearance. Histologically, it is an inflammatory product containing fibrin, neutrophils, macrophages, lymphocytes, and dendritic cells1).
Conjunctivitis usually resolves within 2–3 weeks, but in cases with pseudomembrane formation, eyelid swelling, conjunctival injection, and edema may persist. After inflammation subsides, superficial scarring of the conjunctiva may remain, and in severe cases, conjunctival prolapse may occur1).
Multiple subepithelial infiltrates (MSI) and staging
After 4–5 days from onset, punctate epithelial keratitis that stains with fluorescein appears, gradually progressing to punctate to small round subepithelial infiltrates with mild intraepithelial infiltration around them1). This is MSI. Without appropriate steroid treatment, MSI can persist as small round to patchy subepithelial opacities for several years or more, causing visual impairment (irregular astigmatism, photophobia)1).
The 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines presents the following staging for the progression of MSI1).
MSI Stage 0–II (acute phase)
Stage 0 (day 2): Epithelial microvesicles, 25–30 μm in size. Barely observable with slit-lamp microscopy.
Stage I (around day 4–5): Punctate epithelial keratitis (superficial epithelium). Punctate elevated lesions observed as small dark spots in the green tear film on fluorescein staining.
Stage II (days 6–9): Punctate epithelial keratitis (deep epithelium). Stage I lesions coalesce and changes extend to the deep epithelium. Stains with fluorescein as larger punctate superficial keratopathy.
MSI Stage III–V (subacute to chronic)
Stage III (week 1–2): Subepithelial infiltrates. In addition to stage II lesions, mild subepithelial haze is present.
Stage IV (week 3 to months): Small round subepithelial opacities. Not stained by fluorescein.
Stage V (weeks to months): Granular, small round subepithelial opacities. Not stained by fluorescein. Cause of visual impairment.
Findings from stage III onward correspond to so-called MSI1).
Clinical presentation varies depending on the causative AdV type 1).
AdV8 (classic type): Historically the main type of EKC worldwide, but detection has decreased since 1997. Pseudomembrane formation is common.
AdV54: Conjunctivitis at onset is moderate; pseudomembrane complication rate is low, but MSI complication rate is 70–80%, and many cases leave subepithelial opacities after healing. Preauricular lymph node swelling occurs in about 50% 1,18).
AdV85: Severe conjunctivitis with eyelid swelling, conjunctival petechiae, and preauricular lymph node swelling in about 70% of cases. Corneal complications such as punctate epithelial keratitis and MSI are also common 1,17).
AdV4 (mild EKC): Presents as mild conjunctivitis, with keratitis complication rate of about 30% 1).
Infant/young child type: Due to underdeveloped adenoid tissue, follicle formation is poor; marked hyperemia, edema, and pseudomembrane are predominant. Preauricular lymph node swelling is less likely. More than half have systemic symptoms such as fever, pharyngitis, bronchitis, otitis media, diarrhea, and vomiting. Severe epithelial keratitis or corneal erosion may occur, and bacterial superinfection can lead to corneal ulcer1).
Chronic papillary conjunctivitis: A type in which foreign body sensation and discharge persist for more than one month after onset of AdV conjunctivitis. Mild hyperemia and papillary hypertrophy are seen on the palpebral conjunctiva, sometimes with a velvety appearance. Caused by AdV3, 5, 7, 8, 19, etc. 1).
AdV urethritis-associated type: AdV37, 53, and 56 can also cause male urethritis. About half of patients with AdV urethritis reportedly develop conjunctivitis at the same time, suggesting a sexually transmitted infection route 1).
QWhen do corneal subepithelial infiltrates (MSI) appear?
A
Punctate epithelial keratitis appears on the corneal surface 4–5 days after onset, progresses to deep punctate keratitis stainable with fluorescein at 6–9 days, and subepithelial infiltrates form from day 7 to week 2. After 3 weeks, they become small round to granular subepithelial opacities. MSI is thought to be a delayed-type hypersensitivity reaction to adenovirus antigens and responds well to steroid eye drops, but early discontinuation may cause recurrence, requiring gradual tapering or stepwise change to a weaker steroid. Decreased vision and photophobia may persist for months to years.
Adenoviridae are non-enveloped icosahedral viruses (diameter 70–90 nm) with double-stranded DNA. They are classified into seven species, A through G. Previously, they were classified into serotypes based on neutralization reactions, but types AdV52 and later are numbered as genotypes based on gene sequences1). Currently, the type is determined by the sequences of the variable regions of the adenovirus genome: penton, hexon, and fiber1).
In 2012, Zhou et al. revealed that the standard strain of AdV19 does not cause EKC, and it is a mutant strain of AdV19 that causes EKC12). This mutant strain is a chimera with the penton region from AdV22 and the fiber region from AdV37, and was redefined as AdV641,12).
Since 2015, a newly identified AdV from Japanese EKC patients has been reported as AdV8517). AdV85 is classified as a recombinant novel human mastadenovirus D, and has also been detected in overseas EKC cases1,17).
The most important transmission route is contact infection via hands1). Adenoviruses have very strong biological properties and multiple transmission routes.
Healthcare workers’ hands: main cause of nosocomial infection through examination and treatment
Tonometer tips: high infection risk due to direct contact with the eyeball
Contaminated eye drop bottles: treatment eye drops used for multiple patients can become a source of infection if used improperly
Environmental surfaces: doorknobs, counters, chairs, etc. Adenovirus suspension maintains infectivity for more than 10 days even under natural drying conditions
Intrafamilial infection is also common, and the 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines adopts a history of intrafamilial infection as a supportive finding for clinical diagnostic criteria1).
AdV conjunctivitis causes nosocomial infections due to its strong infectivity, so prompt and accurate diagnosis is required1). It is important for receptionists, orthoptists, and nurses to interview patients about conjunctival hyperemia and discomfort, and to promptly attempt a definitive diagnosis using a rapid diagnostic kit for patients suspected of infection1). If two or more patients occur in a ward, it is considered a nosocomial infection, and measures such as restricting new admissions and closing the ward for at least one week should be taken1).
Diagnosis of AdV conjunctivitis is made by combining findings of acute follicular conjunctivitis with virological testing, or characteristic clinical findings1).
Category
Item
A. Microbiological testing
A-1. AdV antigen positive by rapid antigen detection kit A-2. AdV gene detection by PCR
Definitive diagnosis: Meets any one of A and shows B-1
Clinical diagnosis: Meets both B-1 and B-2, and additionally any one of B-3, B-4, C, D, or E is positive
Because some facilities cannot perform microbiological testing or cases with negative microbiological results still strongly suggest EKC, a clinical diagnostic criterion combining conjunctival petechiae, conjunctival pseudomembrane, and household transmission—clinical findings strongly correlated with virological testing—has been established1).
The AdV rapid antigen detection kit using immunochromatography (IC) is called an antigen detection kit and is the only test method that allows rapid and simple identification of AdV antigen1). It is an essential test for diagnosing AdV conjunctivitis in clinical settings and should be kept available in ophthalmology outpatient clinics.
Test method
Sensitivity
Specificity
Time to result
Features
Immunochromatography (conjunctival swab)
Approximately 70–80%
Nearly 100%
5–15 minutes
Positive result confirms diagnosis. Requires conjunctival swab with cotton swab.
Immunochromatography (tear collection)
Approximately 70–80%
Nearly 100%
5–15 minutes
Filter paper 5×5 mm placed on lower eyelid; minimally invasive, useful in children3)
Silver amplification automated IC method
Increased
Nearly 100%
Approximately 15 minutes
Labeled gold colloid amplified approximately 100-fold with silver; currently highest sensitivity 4)
For conjunctival scraping specimens, after topical anesthesia, the palpebral conjunctiva is firmly scraped several times with a cotton swab. Insufficient specimen volume can reduce detection sensitivity, so adequate scraping is necessary1). The collected swab is stirred in an extraction tube and rubbed thoroughly against the inner wall to release the virus from the swab into the extraction fluid1).
Tear fluid collection is a method introduced after 2018, in which the attached filter paper is placed against the lower eyelid to collect tears containing conjunctival exudate1,3). Since it does not require scraping the conjunctiva, it is minimally invasive and useful for pediatric cases. As of April 2024, the antigen detection kits compatible with tear fluid collection are the three kits: “QuickChaser® Adeno Eye”, “QuickChaser® Auto Adeno Eye”, and “Fuji Dri-Chem IMMUNO AG Cartridge Adeno OPH”1).
The specificity is nearly 100%, so a positive result confirms AdV infection. On the other hand, the detection sensitivity is approximately 70–80%, so a negative result does not completely rule out AdV infection1).
Even when specimens were collected by ophthalmologists skilled in managing infectious conjunctivitis, AdV-DNA was detected by PCR in only about half of cases1). Furthermore, since the detection sensitivity is about 80%, not all PCR-positive specimens are positive by the immunochromatography method. In clinical practice, antigen detection kits are positive in only about 10–20% of cases, with most results being negative1). However, a positive result confirms AdV infection, so performing the test is of great significance.
PCR is a genetic testing method that amplifies a target DNA region millions of times using sequence-specific primers and DNA polymerase, allowing identification of AdV with higher sensitivity than antigen detection kits1). It is not covered by insurance and must be outsourced to testing laboratories or specialized institutions such as local public health institutes.
Serotype identification is possible from the base sequence of the hexon region, and the type is determined by the sequences of the penton, hexon, and fiber regions1). In clinical practice, infection control strategies do not differ significantly by type, but since the severity of conjunctivitis and the frequency of corneal complications vary by type, knowing the type is helpful for treatment and follow-up1).
In patients clinically suspected of having AdV conjunctivitis, a Giemsa-stained smear of eye discharge showing a predominance of mononuclear cells (lymphocytes) suggests viral infection and serves as an auxiliary diagnostic method indicating viral conjunctivitis, including AdV1).
Differentiation from infectious diseases presenting with acute follicular conjunctivitis is necessary. The 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines includes a flowchart for differential diagnosis of conjunctivitis, which diagnoses based on the presence or absence of follicles and papillae on the palpebral conjunctiva, the nature of eye discharge, associated findings of the cornea and eyelids, and the presence or absence of systemic symptoms1).
Differentiation from HSV conjunctivitis is particularly difficult. HSV conjunctivitis is often unilateral and resolves in a relatively short period of about 7 days, but it rarely presents typical findings such as dendritic keratitis, and it is thought that a certain number of cases are included among those negative for the AdV rapid antigen detection kit1). Since eyelid and skin lesions may be present, attention should also be paid to skin findings.
EKC is a Category V infectious disease under the Infectious Diseases Law, and designated ophthalmology sentinel medical institutions report on a weekly basis. Under the School Health and Safety Act Enforcement Regulations, it is classified as a Type 3 “Other infectious disease”, and students are required to stay home until a physician determines that there is no risk of infection. Although there is no clear regulation on the number of days, approximately 2 weeks is generally considered the guideline based on the clinical course.
QIf the rapid test is negative, does that mean it is not epidemic keratoconjunctivitis?
A
No, it does not. According to the 2025 edition of the Viral Conjunctivitis Clinical Practice Guidelines, the sensitivity of rapid antigen detection kits is approximately 70–80%, and a negative result cannot completely rule out AdV infection. Even in specimens collected by ophthalmologists skilled in infectious conjunctivitis treatment, AdV-DNA can be detected by PCR in only about half of cases, and not all PCR-positive specimens are positive by the immunochromatography method. If EKC is strongly suspected based on clinical findings and course despite a negative result, diagnosis is made by combining clinical diagnostic criteria such as conjunctival hemorrhagic spots, pseudomembrane, and intrafamilial infection.
Currently, there is no specific antiviral drug against adenovirus, and there is no curative treatment for EKC1). Treatment targets are anti-inflammatory therapy in the acute phase and treatment of MSI, and steroid eye drops, iodine preparations, and immunosuppressive eye drops should be carefully considered according to the disease stage and severity1).
Concomitant use of iodine-based eye drops (OTC) for about 3 days to 1 week is also an option
At follow-up (around day 7)
If MSI appears: start topical steroids (consider adding iodine-based drops in severe cases)
Chronic phase (when MSI persists)
For cases that relapse with steroid tapering, steroid-resistant MSI, or steroid-induced intraocular pressure elevation: consider topical immunosuppressants (OTC)
Topical antibiotics are generally ineffective for viral conjunctivitis and should only be used in the early stage when there is severe corneal epithelial damage 1). In severe EKC such as type D, bacterial co-infection is observed at a certain frequency, so topical antibiotics may be necessary.
Given the rapid increase in quinolone-resistant Corynebacterium in Japan, cefmenoxime eye drops are recommended as the first choice 1). Aminoglycoside eye drops should be avoided as they tend to cause corneal epithelial damage 1). Any antibiotic should be used for a short period with appropriate use in mind.
Topical steroids are not essential in mild cases, but are useful when severe inflammation causes pseudomembrane formation, filamentary keratitis, or corneal epithelial defects, or for early symptom relief 1).
However, in addition to the side effects of glaucoma and cataracts caused by steroid eye drops, delayed viral clearance has been reported1). Therefore, during the acute phase of active viral proliferation, it is desirable to use steroid eye drops in combination with iodine preparations1).
Steroid eye drops when MSI appears are useful for cell infiltration caused by a delayed-type hypersensitivity reaction to AdV antigens. As a typical prescription example, using a stronger steroid such as 0.1% betamethasone sodium phosphate (Sanbetazone®) can alleviate or eliminate even fairly severe opacities. If eye drops are stopped early, opacities may increase again, so measures such as gradually reducing the frequency of instillation or switching to a weaker steroid are necessary. Intraocular pressure monitoring is essential during long-term use.
For severe inflammation in children aged 3 years or younger who have difficulty with eye drops, oral steroids may also be considered1,9).
Iodine preparations exert a bactericidal effect by oxidizing and denaturing surface proteins of microorganisms through free iodine1). Povidone-iodine (PVP-I) has been shown to be effective against many AdV types within 1 to 5 minutes in in vitro studies, with efficacy confirmed against AdV-1, -2, -3, -4, -5, -6, -7, -8, -11, -37, -53, -54, -56, -64, -81, and -851).
However, PVP-I is generally not recommended for use on the ocular mucosa; in Japan, a diluted solution of iodine-polyvinyl alcohol (PVA-I), which has a similar inactivating effect, is used1).
PA·Iodine eye drops and eye wash solution: Used after diluting 4 to 8 times with physiological saline. Safety and efficacy for the ocular surface have been recognized for corneal herpes and eye wash sterilization.
Saniod® eye drops: An OTC drug launched in 2022. Not covered by insurance, full patient payment, limited use within 3 days after opening, and may cause irritation.
In a study of patients within one week of EKC onset, the combination of 6-fold diluted PVA-I and 0.1% fluorometholone eye drops (Flumetholon® 0.1%) was shown to suppress the development of MSI compared to the combination of levofloxacin hydrate and 0.1% fluorometholone eye drops6). There is also a report that a single administration at the time of visit was effective in suppressing early symptoms5).
As non-steroidal immunosuppressants, cyclosporine and tacrolimus are used. Both inhibit calcineurin and suppress IL-2 production necessary for T-cell proliferation1).
Cyclosporine eye drops 0.05% / 0.5% / 1% / 2%: Reported to be effective in preventing and improving the acute onset of MSI and in reducing chronic prolongation1,7). Compared to steroids, they have the advantage of less recurrence after discontinuation1). In animal models, they are known to suppress MSI while increasing viral titers1)
Tacrolimus eye drops 0.03%: In chronic cases of prolonged MSI, they reduce the size and number of MSI, leading to improved visual prognosis1,8). They are also effective against steroid-resistant MSI and can be expected to allow steroid tapering. Side effects occur in 17.8% (mainly burning sensation, redness, foreign body sensation), and a major advantage is that they do not cause increased intraocular pressure1)
These should be considered for use in cases of steroid-resistant MSI or MSI that recurs upon steroid tapering, as well as in cases where steroid eye drops have caused increased intraocular pressure1).
Histologically, pseudomembranes are inflammatory products containing fibrin, neutrophils, macrophages, lymphocytes, and dendritic cells. They must be removed early to prevent conjunctival fibrosis and adhesion/scarring due to keratinization1). When removing them, take sufficient infection control measures and be careful not to forcibly peel them off.
To prevent worsening of keratoconjunctival damage and transmission of the virus due to AdV conjunctivitis, instruct patients to discontinue contact lens use. Considering the viral shedding period, discontinuation should last approximately 2 weeks after onset, i.e., until clinical findings have resolved1). Thereafter, the decision is based on the presence of prolonged MSI.
Since the main route of infection is via hands, hand washing and wearing gloves are important1).
Healthcare workers’ hands: After physically removing the virus with running water, apply disinfectant ethanol or alcohol-based hand rub to the hands and allow to dry. Use disposable gloves for patients suspected of viral infection
Ophthalmic examination instruments (slit lamp, indirect ophthalmoscope, non-contact lens, trial frame, trial lenses): Wipe with 80% alcohol after use
Instruments that come into complete contact with the eye (contact lenses, lid speculum, tonometer tip): After thorough washing with water, immerse in 80% alcohol for 5 minutes
Strongest disinfectant: 0.1% sodium hypochlorite (however, it causes skin damage and metal corrosion, so cannot be used on hands or medical instruments)
Multipurpose disinfectant (MPD): Rubista® (Virkon®) can be used as an alternative to 80% alcohol wiping and is highly effective in inactivating various viruses and bacteria1)
If two or more patients in the ward develop the infection, it is considered a nosocomial outbreak, and new admissions are restricted while the ward is closed for at least one week 1).
Steroid eye drops are not used in all cases; they are considered when there is severe inflammation, pseudomembrane formation, filamentary keratitis, corneal epithelial defects, or multiple subepithelial infiltrates (MSI). Since viral clearance is delayed with acute-phase use, concomitant use with iodine preparations is recommended. Strong steroids such as 0.1% betamethasone are effective for MSI, but early discontinuation may lead to recurrence, so gradual tapering or stepwise switching to weaker steroids is necessary, and intraocular pressure monitoring is essential during long-term use. In steroid-resistant cases or cases with elevated intraocular pressure, cyclosporine or tacrolimus eye drops may be considered, although they are not covered by insurance.
6. Pathophysiology and Detailed Mechanisms of Onset
Adenoviridae are non-enveloped, icosahedral viruses (diameter 70–90 nm) with double-stranded DNA, and a molecular weight of 20–25 × 10⁶. Infection begins when the adenovirus fiber, which has affinity for receptors on conjunctival epithelial cells, attaches. Receptors differ by type, and the difference in clinical presentation between EKC type, which has strong conjunctivitis symptoms, and PCF type, which presents with systemic symptoms, is determined by the relationship between the receptor and the viral fiber.
Changes in Type Classification and Prevalent Types in Japan
Previously, AdV types were determined as serotypes by neutralization reactions using cultured viruses1). However, because the available neutralizing antisera were limited in type, it was difficult to determine all types.
Subsequently, advances in genetic testing made it possible to identify serotypes from the base sequence of the hexon region, the gene responsible for neutralization. Furthermore, the structure of the AdV genome was elucidated, revealing the existence of recombinant viruses between types1). AdV1–51 are serotypes determined by neutralization, but AdV52 and later are numbered as genotypes based on base sequences1). Currently, types are determined by the sequences of the penton, hexon, and fiber regions.
In 2012, Zhou et al. clarified that the standard strain of AdV19 does not cause EKC, and that the cause of EKC is a chimeric AdV19 mutant with penton region type 22 and fiber region type 37, which was redefined as AdV6412).
A study of AdV conjunctivitis clinical findings in southern Kyushu, Japan from 2011 to 2014 reported that AdV8, 37, and 54 caused corneal complications significantly more frequently and had longer infection periods than AdV53 and 5616). This suggests that accurately knowing the type is clinically and epidemiologically meaningful.
Kaneko et al., through molecular epidemiological analysis of AdV54, showed that AdV54 is evolutionarily closely related to AdV8 and that it became prevalent in Japan after 1997, replacing the decreasing detection of AdV8 18). AdV54 has rarely been reported outside Japan and is a unique epidemic type in Japan 1,18).
Pathophysiology of MSI (delayed-type hypersensitivity)
MSI is thought to be a cellular infiltration caused by a delayed-type hypersensitivity reaction to AdV antigens in the outermost layer of the corneal stroma, and not due to viral proliferation 1). This concept has been established since the classic study by Seiji Sugiura in 1959. However, the possibility of latent adenovirus infection has not been completely ruled out.
Approximately 10 days after onset, type-specific neutralizing antibody titers rise, coinciding with the improvement of clinical symptoms. Neutralizing antibodies are type-specific; for example, infection with AdV8 does not confer neutralizing antibodies against AdV3, so clinical reinfection is possible. On the other hand, because there is cross-reactivity within the same species, patients with a history of AdV37 infection are less susceptible to AdV8.
However, it has been suggested that neutralizing antibodies may not be maintained throughout life, and the possibility of reinfection with the same type in adulthood after childhood infection cannot be ruled out.
Arici et al. (2022) studied 66 eyes of 33 patients with subepithelial corneal infiltrates (SEI) and reported that the central corneal thickness (CCT) of the initially affected eye was significantly thinner at 526.1±28.1 μm compared to the control group (557.0±38.1 μm) (p=0.003) 13). The best-corrected visual acuity (logMAR) of the initially affected eye was significantly worse at 0.20±0.29 compared to the control group (−0.01±0.05), and a negative correlation was found between SEI density and IOPg/IOPcc (r=−0.479, p=0.006) 13). It should be noted that the decrease in central corneal thickness in SEI-affected eyes may lead to underestimation of intraocular pressure measurements during steroid treatment.
According to the 2025 Guidelines for the Management of Viral Conjunctivitis, the number of reported EKC cases per sentinel site decreased to about one-third of pre-pandemic levels during the COVID-19 pandemic, but recovered to nearly normal levels by 2023 1). PCF resurged to about twice the normal level in 2023, and it is necessary to be aware that EKC may also experience outbreaks exceeding pre-pandemic levels in the future 1,2).
Monitoring trends in age groups that previously showed high incidence rates, such as in nursery schools, kindergartens, and schools, is particularly important 2).
Development of specific antiviral drugs is ongoing. Ganciclovir gel and povidone-iodine have been reported to shorten the duration of acute EKC and reduce the risk of subepithelial infiltrates, but optimal concentrations and doses have not been established 5,10,11). A Cochrane review (Liu 2022) concluded that current evidence for topical pharmacological interventions for EKC is limited, and no drug has demonstrated a clinically robust benefit compared to control groups 15).
Cyclosporine and tacrolimus eye drops are considered promising for the treatment of MSI, especially in steroid-resistant cases or those that relapse during steroid tapering 1,7,8).
Among antiviral agents under investigation, cidofovir eye drops inhibit viral DNA polymerase intracellularly, but randomized controlled trials have not shown significant improvement in clinical course, and side effects such as lacrimal duct stenosis and conjunctival inflammation have been reported. Trifluridine eye drops reduce viral load of AdV8, 19, and 13 in vitro, but no reduction in treatment duration has been observed in human clinical trials. Oral famciclovir is a candidate for phase II trials as a potent inhibitor of AdV.
Minimally invasive and highly sensitive rapid diagnostic kits, such as immunochromatography using tear samples and silver-enhanced automated IC methods, have been introduced 1,3,4). These are expected to reduce the burden, especially in pediatric cases, and improve detection rates in cases where conventional sensitivity was low, such as in the second eye.
Acute dacryoadenitis secondary to EKC is an extremely rare complication in adults. Takahashi et al. (2022) reported adult acute dacryoadenitis associated with EKC, with serum testing confirming adenovirus type 3 IgM positivity 14). The mechanism is thought to involve direct invasion of the lacrimal gland or secondary spread from keratoconjunctival lesions, and only 4–5 adult cases have been reported 14).
Since 2015, a new virus, AdV85, has been identified in Japan, including reports of five cases in Fukushima Prefecture 17). AdV85 is a recombinant human mastadenovirus D that presents with typical clinical features of EKC (severe conjunctivitis, petechiae, preauricular lymphadenopathy, MSI) 1,17). Attention to future epidemic trends is necessary.
Seo Y, Kim I, Cha J, Kang S, Gwack J. [Ophthalmologic Sentinel Surveillance Results, 2013-2022]. Public Health Wkly Rep. 2023;16(29):992-1004. doi:10.56786/PHWR.2023.16.29.2. PMID:41333894; PMCID:PMC12551754.
Migita H, Ueno T, Tsukahara-Kawamura T, Saeki Y, Hanaoka N, Fujimoto T, et al. Evaluation of adenovirus amplified detection of immunochromatographic test using tears including conjunctival exudate in patients with adenoviral keratoconjunctivitis. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2019;257(4):815-820. doi:10.1007/s00417-019-04281-7. PMID:30826875.
Fujimoto T, Hanaoka N, Konagaya M, Kobayashi M, Nakagawa H, Hatano H, et al. Evaluation of a silver-amplified immunochromatography kit for adenoviral conjunctivitis. Journal of medical virology. 2019;91(6):1030-1035. doi:10.1002/jmv.25404. PMID:30659635.
Than T, Morettin CE, Harthan JS, Hartwick ATE, Huecker JB, Johnson SD, et al. Efficacy of a Single Administration of 5% Povidone-Iodine in the Treatment of Adenoviral Conjunctivitis. American journal of ophthalmology. 2021;231:28-38. doi:10.1016/j.ajo.2021.05.018. PMID:34102153; PMCID:PMC11460794.
Matsuura K, Terasaka Y, Miyazaki D, Shimizu Y, Inoue Y. Comparative study of topical regimen for adenoviral kearoconjunctivitis by 0.1% fluorometholone with and without polyvinyl alcohol iodine. Jpn J Ophthalmol. 2021;65(1):107-114. doi:10.1007/s10384-020-00788-3. PMID:33241466.
Gouider D, Khallouli A, Maalej A, Yousfi MA, Ksiaa I, Bouguerra C, et al. Corticosteroids Versus Cyclosporine for Subepithelial Infiltrates Secondary to Epidemic Keratoconjunctivitis: A Prospective Randomized Double-Blind Study. Cornea. 2021;40(6):726-732. doi:10.1097/ICO.0000000000002589. PMID:33201059.
Arici C, Mergen B. Late-term topical tacrolimus for subepithelial infiltrates resistant to topical steroids and ciclosporin secondary to adenoviral keratoconjunctivitis. The British journal of ophthalmology. 2021;105(5):614-618. doi:10.1136/bjophthalmol-2020-316196. PMID:32563992.
Kim SY, Chang YK, Lee YC, Kim SY. Oral steroid therapy as an adjuvant treatment for severe epidemic keratoconjunctivitis in patients younger than 3 years. Cornea. 2015;34(2):182-187. doi:10.1097/ico.0000000000000332.
Huang J, Kadonosono K, Uchio E. Antiadenoviral effects of ganciclovir in types inducing keratoconjunctivitis by quantitative polymerase chain reaction methods. Clinical ophthalmology (Auckland, N.Z.). 2014;8:315-20. doi:10.2147/OPTH.S55284. PMID:24511226; PMCID:PMC3915018.
Ozen S, Ozer MA. Ganciclovir ophthalmic gel treatment shortens the recovery time and prevents complications in the adenoviral eye infection. International ophthalmology. 2017;37(1):245-249. doi:10.1007/s10792-016-0260-1. PMID:27221265.
Zhou X, Robinson CM, Rajaiya J, Dehghan S, Seto D, Jones MS, et al. Analysis of human adenovirus type 19 associated with epidemic keratoconjunctivitis and its reclassification as adenovirus type 64. Invest Ophthalmol Vis Sci. 2012;53(6):2804-2811. doi:10.1167/iovs.12-9656.
Arici C, Sultan P, Mergen B. Evaluation of the impact of subepithelial corneal infiltrates on corneal biomechanics after epidemic keratoconjunctivitis. Arquivos brasileiros de oftalmologia. 2022;85(5):478-484. doi:10.5935/0004-2749.20220061. PMID:34852057; PMCID:PMC11826794.
Takahashi Y, Vaidya A, Kono S, Yokoyama T, Kakizaki H. Epidemic Keratoconjunctivitis-Associated Acute Dacryoadenitis in an Adult. Cureus. 2022;14(7):e27003. doi:10.7759/cureus.27003. PMID:35989856; PMCID:PMC9386646.
Liu SH, Hawkins BS, Ren M, Ng SM, Leslie L, Han G, et al. Topical Pharmacologic Interventions Versus Active Control, Placebo, or No Treatment for Epidemic Keratoconjunctivitis: Findings From a Cochrane Systematic Review. American journal of ophthalmology. 2022;240:265-275. doi:10.1016/j.ajo.2022.03.018. PMID:35331686; PMCID:PMC9808666.
Aoki K, Gonzalez G, Hinokuma R, Yawata N, Tsutsumi M, Ohno S, et al. Assessment of clinical signs associated with adenoviral epidemic keratoconjunctivitis cases in southern Japan between 2011 and 2014. Diagn Microbiol Infect Dis. 2019;95(4):114885.
Hashimoto S, Gonzalez G, Harada S, Oosako H, Hanaoka N, Hinokuma R, et al. Recombinant type Human mastadenovirus D85 associated with epidemic keratoconjunctivitis since 2015 in Japan. J Med Virol. 2018;90(5):881-889. doi:10.1002/jmv.25041. PMID:29396992.
Kaneko H, Suzutani T, Aoki K, Kitaichi N, Ishida S, Ishiko H, et al. Epidemiological and virological features of epidemic keratoconjunctivitis due to new human adenovirus type 54 in Japan. The British journal of ophthalmology. 2011;95(1):32-6. doi:10.1136/bjo.2009.178772. PMID:20530657.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.