Dacryoadenitis is a general term for inflammation of the lacrimal gland. The lacrimal gland is an exocrine gland located in the lacrimal fossa on the lateral side of the superior orbital wall, secreting the aqueous layer of tears into the conjunctival sac. It consists of the orbital lobe (larger part) and the palpebral lobe (smaller part), and inflammation of both is collectively called dacryoadenitis.
Dacryoadenitis is broadly classified into two categories: acute dacryoadenitis and chronic dacryoadenitis. Acute dacryoadenitis is further subdivided into viral and bacterial types. In viral cases, mumps virus and Epstein-Barr virus are typical causative agents, often presenting bilaterally. In bacterial cases, staphylococci and gonococci are the main causative bacteria, and cases resulting from local infections such as hordeolum or trauma are often unilateral 12.
Chronic dacryoadenitis includes types associated with systemic diseases such as leukemia, Hodgkin disease, tuberculosis, syphilis, and sarcoidosis, as well as IgG4-related dacryoadenitis occurring as a subtype of IgG4-related ophthalmic disease34. IgG4-related dacryoadenitis commonly occurs after the age of 60 with no significant gender difference. When accompanied by swelling of the salivary glands (submandibular and parotid glands), it is known as Mikulicz disease and is considered a subtype of IgG4-related disease 3.
Acute dacryoadenitis increases during mumps epidemics. In periods of low mumps vaccination rates, mumps dacryoadenitis may increase in adults and schoolchildren. Dacryoadenitis associated with sarcoidosis is relatively common and may be discovered incidentally during an initial ophthalmologic examination.
QWhat is the difference between dacryoadenitis and dacryocystitis?
A
Dacryoadenitis is inflammation of the lacrimal gland (located in the lacrimal fossa on the lateral part of the superior orbital wall) that secretes tears, presenting as swelling and tenderness of the lateral upper eyelid. Dacryocystitis is inflammation of the lacrimal sac (near the inner canthus) in the tear drainage pathway, causing swelling and pain below the inner canthus. Because the anatomical location and the site of symptoms are clearly different, they can be distinguished by examination.
Acute dacryoadenitis often presents with sudden swelling of the lateral upper eyelid and severe pain. It may be accompanied by redness, warmth, and a sensation of eye protrusion. Severe inflammation may be associated with fever and general malaise.
Chronic dacryoadenitis primarily presents with painless eyelid swelling. It is often bilateral, and patients may complain that “both upper eyelids are swollen.” In IgG4-related cases, swelling of the cheeks or submandibular area (salivary gland sites) may also be noticed.
Viral: often bilateral / Bacterial: often unilateral
Often bilateral
Pain
Severe (lacrimal gland tenderness)
None in principle
Redness and swelling
Marked (lateral upper eyelid)
Mild to moderate
Proptosis
Present during severe inflammation
Usually absent
Palpable mass
Enlarged lacrimal gland on palpation
Elastic soft to hard mass
Salivary gland swelling
Absent
Complicated in IgG4-related disease
S-shaped ptosis is a characteristic finding of acute dacryoadenitis. Only the lateral part of the upper eyelid (the lacrimal gland area) is swollen, while the medial part is normal, so the upper eyelid margin appears to form an S-shaped curve. This shape is due to the lacrimal gland being located laterally in the eyelid.
In IgG4-related dacryoadenitis, in addition to bilateral symmetric lacrimal gland enlargement, painless swelling of the submandibular and parotid glands is often present simultaneously, which is a diagnostic clue (Mikulicz disease).
QIf the lacrimal gland is swollen, is it dacryoadenitis?
A
Causes of lacrimal gland enlargement include dacryoadenitis, lacrimal gland tumors (pleomorphic adenoma, adenoid cystic carcinoma), and malignant lymphoma. If accompanied by acute redness and pain, inflammation is suspected, but for chronic, painless enlargement, differentiation from a tumor is the top priority. Pathological confirmation by biopsy may be necessary.
Visual inspection of the eyelid is the basis of diagnosis. Swelling and redness of the outer upper eyelid (acute cases) or diffuse hard swelling (chronic cases) are confirmed. Palpation assesses tenderness, hardness, and mobility of the mass. Acute dacryoadenitis shows marked tenderness, while chronic dacryoadenitis presents with an elastic soft to hard mass.
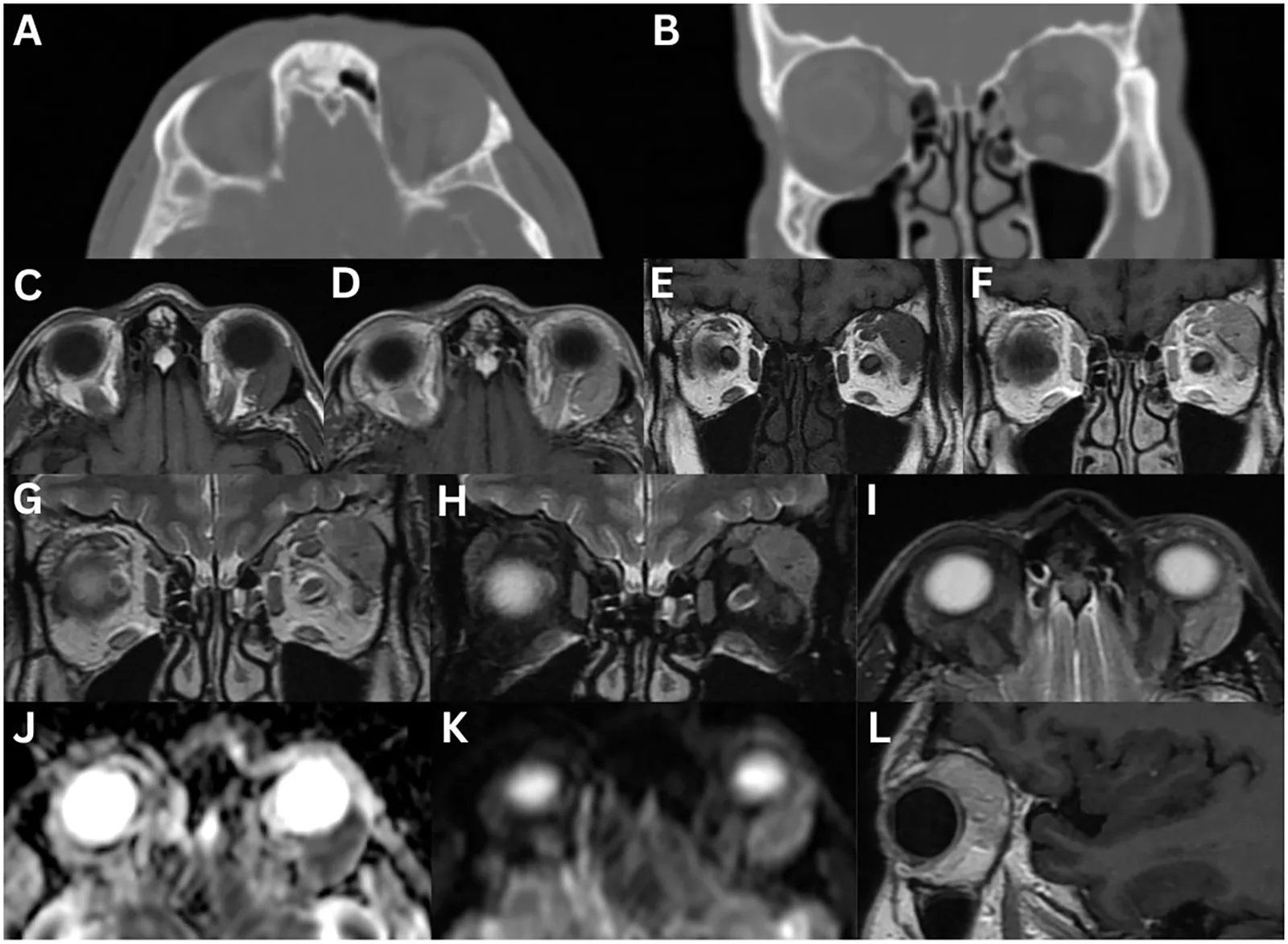
Caltabiano C, Rana K, Buckby A, Patel S, Selva D. Imaging features of lacrimal gland disease. Front Ophthalmol. 2025;5:1724513. Figure 7. DOI: 10.3389/fopht.2025.1724513. License: CC BY 4.0.
Isolated enlargement of the left lacrimal gland in a patient with IgG4-related dacryoadenitis: CT (A, B) shows no bone erosion; MRI sequences show well-defined enlargement, mild contrast enhancement, and diffusion restriction of the lacrimal gland. Corresponds to CT and MRI findings (diffuse enlargement, presence of bone destruction, enhancement pattern) discussed in the “Diagnosis and examination methods” section.
CT scan is the main test to evaluate lacrimal gland enlargement and morphology. It differentiates diffuse from nodular enlargement and checks for bone destruction. Bone destruction strongly suggests adenoid cystic carcinoma. MRI has higher soft tissue resolution than CT and can assess signal changes on T2-weighted images. IgG4-related dacryoadenitis often shows homogeneous low T2 signal.
In chronic dacryoadenitis, biopsy may be necessary to differentiate from malignant tumors. Biopsy allows histopathological confirmation of the density of IgG4-positive plasma cell infiltration (IgG4-positive cells ≥50/HPF, IgG4+/IgG+ plasma cell ratio ≥40%) and the presence or absence of malignant lymphoma or adenoid cystic carcinoma. The diagnostic criteria for IgG4-related dacryoadenitis and sialadenitis revised in 2023 adjusted the thresholds to an IgG4+/IgG+ ratio of 0.4 or higher and IgG4-positive cells >10/HPF, and also approved the use of labial gland biopsy 5.
Even with symptoms resembling chronic dacryoadenitis, lacrimal gland tumors must be ruled out. If there is a painless, solitary, hard mass, bone destruction, rapid enlargement, or no response to antibiotics or steroids, perform an early biopsy. For malignant lymphoma or adenoid cystic carcinoma, prompt referral to the appropriate treatment department is necessary after histological confirmation.
The recommended initial dose of prednisolone is 0.6 mg/kg/day (typically 30 mg/day). After 2–4 weeks, assess the response; if swelling has reduced, taper by 10% every 2 weeks. Long-term continuation is often necessary even after reaching a maintenance dose (5–10 mg/day), and regular follow-up is essential to monitor for relapse during tapering. During long-term steroid use, monitor for the development or worsening of diabetes, osteoporosis, peptic ulcer, cataracts, and glaucoma.
In steroid-resistant or steroid-dependent cases, addition of an immunosuppressant (e.g., azathioprine) may be considered. There are also reports of remission induction and maintenance with anti-CD20 antibody (rituximab), but insurance coverage must be confirmed.
QCan IgG4-related dacryoadenitis be cured?
A
Steroid therapy often achieves a good response such as reduction of swelling, but relapse is common during tapering. Long-term follow-up and careful dose reduction are necessary. In steroid-resistant cases, addition of an immunosuppressant may be considered. Some patients achieve complete remission, but maintenance therapy is often prolonged.
QDoes acute dacryoadenitis resolve on its own?
A
Viral acute dacryoadenitis (mumps, EB virus) often resolves spontaneously within 2–4 weeks. However, bacterial cases require antibiotic treatment, and incision and drainage may be considered if an abscess forms. The decision to wait for spontaneous recovery depends on clinical judgment of whether the cause is viral or bacterial.
Pathogens such as mumps virus and EB virus infiltrate the lacrimal gland parenchyma via hematogenous or local routes. Direct infection of lacrimal gland epithelial cells and migration of neutrophils and lymphocytes induced by inflammatory cytokines occur, leading to interstitial edema. Swelling of the glandular tissue due to edema causes bulging of the lateral upper eyelid (S-shaped ptosis). In cases of spontaneous recovery, inflammation subsides within 2–4 weeks, and the glandular structure recovers.
In bacterial dacryoadenitis, bacteria spread from nearby infectious foci such as hordeolum, trauma, or sinusitis, causing acute suppurative inflammation. In severe cases, abscess formation occurs, requiring incision and drainage.
Persistent infiltration of lymphocytes and plasma cells occurs in the gland parenchyma, leading to fibrosis and hardening of the gland tissue. It has aspects of an inflammatory pseudotumor and can be difficult to distinguish from a tumor.
IgG4-related disease is a systemic disease concept in which IgG4-positive plasma cells and regulatory T cells infiltrate various organs, causing fibrosis and hardening. In the lacrimal gland, the following pathological processes progress.
High-density infiltration of IgG4-positive plasma cells in lacrimal gland tissue (≥50 cells/HPF)
Storiform fibrosis (whorled fibrous proliferation) forms in the gland parenchyma
Obliterative phlebitis (inflammatory cell infiltration around veins and luminal occlusion) is a histological feature
Progression from gland enlargement to fibrosis to hardening, leading to gland dysfunction (decreased tear secretion, dry eye)
Mikulicz disease is a condition in which the lacrimal glands and major salivary glands (submandibular and parotid glands) are simultaneously affected, and is positioned as a subtype of IgG4-related disease3
In sarcoidosis, non-caseating epithelioid cell granulomas form in the lacrimal gland tissue. T cells and activated macrophages (epithelioid cells) aggregate to form granulomas containing multinucleated giant cells. Lacrimal gland sarcoidosis often begins unilaterally and eventually becomes bilateral4.
Diagnostic criteria for IgG4-related disease are being internationally standardized. In addition to the 2019 International Classification Criteria for IgG4-related disease (ACR/EULAR scoring system), the 2023 revised diagnostic criteria for IgG4-related dacryoadenitis and sialadenitis now include asymmetric lesions and cases involving two or fewer glands, broadening the diagnostic scope 5.
The efficacy of rituximab (anti-CD20 antibody) for steroid-resistant or steroid-dependent IgG4-related dacryoadenitis has been reported in multiple case reports and case series, and it is attracting attention as a future treatment option 3.
Management of lacrimal secretion dysfunction (dry eye) after dacryoadenitis is a clinical challenge. When fibrosis of the gland parenchyma has progressed, tear secretion may not recover despite improvement in gland swelling with steroids, requiring long-term tear replacement therapy.
As minimally invasive diagnostic methods that do not require biopsy, research on MRI biomarkers (ADC values, dynamic contrast patterns) and serum biomarkers is progressing. In the future, it may be possible to differentiate IgG4-related disease from tumors without tissue diagnosis.
Wai KM, Wolkow N, Yoon MK. Infectious Dacryoadenitis: A Comprehensive Review. Int Ophthalmol Clin. 2022;62(2):71-86. doi:10.1097/IIO.0000000000000412. PMID: 35325911. https://pubmed.ncbi.nlm.nih.gov/35325911/↩
Maehara T, Pillai S, Stone JH, Nakamura S. Clinical features and mechanistic insights regarding IgG4-related dacryoadenitis and sialoadenitis: a review. Int J Oral Maxillofac Surg. 2019;48(7):908-916. doi:10.1016/j.ijom.2019.01.006. PMID: 30686634. https://pubmed.ncbi.nlm.nih.gov/30686634/↩↩2↩3↩4
Yanardag H, Pamuk ON. Lacrimal gland involvement in sarcoidosis. The clinical features of 9 patients. Swiss Med Wkly. 2003;133(27-28):388-391. doi:10.4414/smw.2003.10125. PMID: 12947527. https://pubmed.ncbi.nlm.nih.gov/12947527/↩↩2
Kanda M, Nagahata K, Moriyama M, et al. The 2023 revised diagnostic criteria for IgG4-related dacryoadenitis and sialadenitis. Mod Rheumatol. 2025;35(3):542-547. doi:10.1093/mr/roae096. PMID: 39441008. https://pubmed.ncbi.nlm.nih.gov/39441008/↩↩2
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.