Hordeolum is an acute bacterial infection of the eyelid glandular tissue. Acute suppurative inflammation occurs in the sebaceous glands, sweat glands, or meibomian glands of the eyelid, with main symptoms of eyelid redness, swelling, and pain. It is a common and frequent ophthalmic disease, commonly known as a “stye.”
Hordeolum (stye) is broadly classified into external and internal types depending on the infected gland.
Severe pain and difficult spontaneous drainage of pus
External hordeolum is a purulent inflammation of the Zeis gland or Moll gland at the base of the eyelashes, with the pus point observed on the skin side. Spontaneous drainage of pus is relatively common. In contrast, internal hordeolum is an acute purulent inflammation of the Meibomian glands that run vertically within the tarsal plate, and the pus point forms on the palpebral conjunctival side. Pain is severe and spontaneous drainage tends to be difficult, so incision and drainage are often indicated.
For differentiation from chalazion, it is important that hordeolum is an acute infectious inflammation with marked redness and pain. Chalazion is a painless chronic granulomatous inflammation and generally lacks inflammatory findings. However, the symptoms of early acute chalazion and hordeolum are similar, and differentiation may not be easy.
QWhat is the difference between hordeolum (stye) and chalazion?
A
Hordeolum is an acute bacterial infection, often caused by Staphylococcus aureus, characterized by redness, pain, and pus formation. In contrast, chalazion is a painless chronic granulomatous inflammation due to retention of meibomian gland secretions, with usually mild inflammatory signs. However, acute chalazion (acute chalazion) may present symptoms similar to hordeolum, making differentiation difficult. If pain persists and the lesion is localized to the eyelid margin, internal hordeolum should be suspected.
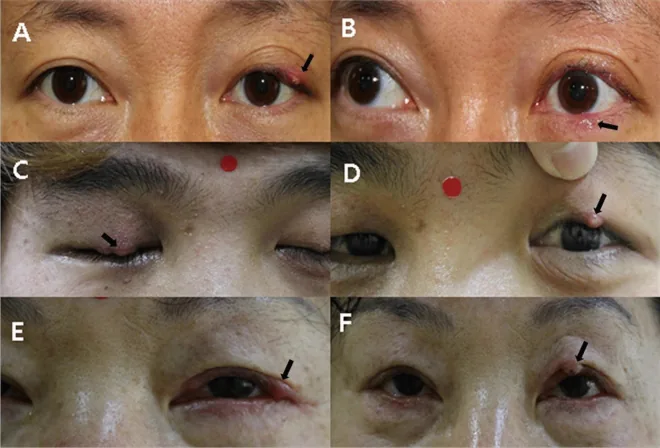
Jun SY, et al. Clinical characteristics of Demodex-associated recurrent hordeola: an observational, comparative study. Sci Rep. 2021;11:21398. DOI: 10.1038/s41598-021-00599-7. Figure 1. PMCID: PMC8560857. License: CC BY 4.0.
Clinical photographs of external hordeolum (arrows) in three cases: a 54-year-old male (A, B), a 21-year-old male (C, D), and a 63-year-old female (E, F), showing localized redness and swelling at the eyelid margin. These correspond to the skin-side pus point, eyelid redness, and swelling of external hordeolum discussed in the section “Main symptoms and clinical findings.”
The symptoms of hordeolum change over the course of the disease. In the early stage, a small induration and a papule with erythematous swelling appear at a localized area of the eyelid, accompanied by redness, swelling, tenderness, and spontaneous pain. In mild cases, pain with blinking is often the main complaint.
Appearance: Localized redness and swelling on the eyelid skin; a pus point is observed on the skin side
Spontaneous drainage: Tends to drain from the skin side
Findings of internal hordeolum
Infection site: Meibomian gland
Pus point location: Conjunctival side
Appearance: Swelling and redness of the eyelid; upon eyelid eversion, a pus point is observed on the conjunctival side
Pain: Stronger than external hordeolum. Pain tends to persist because spontaneous drainage is difficult.
As it progresses, an abscess with a pus plug forms at the apex of the infected area. External and internal hordeola are distinguished by the location of the pus point: in external hordeolum, the pus point is observed on the skin side; in internal hordeolum, it is observed on the palpebral conjunctival side.
In children, the eyelid becomes swollen and red, and as the swelling subsides, a small bean- to soybean-sized induration (abscess) is often palpable. In infants, because the immune system is immature, a hordeolum can rapidly progress to eyelid abscess or orbital cellulitis. Therefore, frequent follow-up is necessary for hordeolum in infants.
Rapid expansion of swelling and redness, fever, proptosis, and ophthalmoplegia suggest progression to orbital cellulitis and require prompt management.
The main causative organism of hordeolum is Staphylococcus aureus. Other organisms detected include coagulase-negative staphylococci (CNS), Propionibacterium acnes, and Corynebacterium species, which are normal flora of the conjunctival sac. In cases with purulent discharge, bacterial culture and antibiotic susceptibility testing are desirable; the detection rate is about 70%.
Diagnosis of hordeolum is based on visual inspection and palpation. Confirm localized eyelid redness, swelling, induration, and purulent point. In cases with discharge, bacterial culture and drug sensitivity testing are recommended, with a detection rate of approximately 70%.
Examination procedure:
Visual inspection: Check the location of eyelid redness, swelling, and purulent point (skin side vs. conjunctival side)
Palpation: Confirm localized induration and tenderness
Eyelid eversion: Performed to confirm purulent point on the conjunctival side in internal hordeolum
Culture test: Bacterial culture and drug sensitivity testing in cases with discharge
QIs imaging necessary for the diagnosis of hordeolum?
A
Imaging tests (MRI, CT, etc.) are not necessary for the diagnosis of ordinary hordeolum. Diagnosis can be made by confirming localized redness, swelling, and purulent point through visual inspection and palpation. However, contrast-enhanced CT is necessary if progression to orbital cellulitis is suspected (proptosis, ophthalmoplegia, high fever, etc.).
The symptoms of early-stage hordeolum and acute chalazion are similar, and differentiation may not be easy. It is important to distinguish from the following diseases.
Inflammation of the entire eyelid or bulbar conjunctiva. Lacks localized induration or purulent point.
In internal hordeolum, persistent pain and localization of the lesion to the eyelid margin help differentiate it from acute chalazion. If recurrent masses are difficult to treat, consider histopathological examination to differentiate from eyelid tumors (e.g., sebaceous gland carcinoma).
This is a useful option for cases where the causative bacteria are deeply involved in the meibomian glands, such as internal hordeolum. For details, refer to the section “Positioning of Azithromycin Eye Drops” in this article.
Oral antibiotics (for severe swelling/redness):
Combined use of oral cephem antibiotics
Anti-inflammatory drugs:
Combined use of anti-inflammatory agents (NSAID eye drops/oral) is also common
Surgical Therapy
Indications for incision and drainage:
When abscess formation occurs and spontaneous drainage is not observed
Especially for internal hordeolum (actively performed due to persistent severe pain)
Since it is a bacterial infection, antibiotic administration is the mainstay of treatment. In many cases, empirical antibiotics and anti-inflammatory drugs are prescribed. Instill Bestron® ophthalmic solution 0.5% (cefmenoxime) or Cravit® ophthalmic solution 0.5% (levofloxacin) 4 times daily. For severe swelling and redness, add oral cephem antibiotics.
Azithromycin hydrate ophthalmic solution 1% (Azimycin® ophthalmic solution 1%) is a 15-membered macrolide antibiotic eye drop approved in Japan for conjunctivitis, blepharitis, hordeolum, and dacryocystitis caused by susceptible pathogens. It distributes well into meibomian glands and lipid-rich tissues, and its long tissue half-life (about 7 days) allows a low-burden regimen: twice daily from day 1 to day 2, then once daily from day 3 onward for a total of 14 days.
Usefulness in internal hordeolum and meibomianitis:
Shimodaira reported that in a study of 3 cases of internal hordeolum and 16 cases of meibomianitis, azithromycin hydrate ophthalmic solution (twice daily on day 1–2, then once daily for 14 days) was effective in improving inflammatory findings. 8) Particularly good responses were obtained in cases where Cutibacterium acnes (formerly Propionibacterium acnes) was isolated, and it was also useful for internal hordeolum complicated by phlyctenular keratoconjunctivitis. 8)
Characteristics of mechanism of action:
Azithromycin is active against Gram-positive cocci (Staphylococcus aureus, coagulase-negative staphylococci) as well as anaerobic meibomian gland commensals such as Cutibacterium acnes, offering an advantage in covering pathogens deep in the meibomian glands that are less accessible to new quinolones and cephems. Additionally, it possesses anti-inflammatory effects (inhibition of matrix metalloproteinases and cytokine production) and lipid metabolism-improving effects independent of its antibacterial action, which may act on the pathophysiology of internal hordeolum and recurrent hordeolum associated with meibomian gland dysfunction (MGD). 9,10)
Positioning:
It is an option to be considered preferentially in internal hordeolum that does not respond to cefmenoxime or levofloxacin eye drops, recurrent hordeolum, and cases with MGD. The lower frequency of instillation and ease of maintaining adherence are advantageous in children and the elderly.
If an abscess forms and spontaneous drainage does not occur, especially in internal hordeolum where severe spontaneous pain persists if left untreated, incision and drainage should be performed.
Anesthesia: Perform infiltration anesthesia of the eyelid skin and conjunctiva. Apply a lid speculum.
For internal hordeolum with a clear pus point, outpatient puncture drainage is effective. Puncture with a 21–25G needle, drain with a cotton swab, and prescribe antibiotics. Compared to incision, it is less invasive and can be completed on an outpatient basis.
QDoes a stye heal on its own?
A
External hordeolum tends to drain spontaneously, and mild cases may heal on their own. However, internal hordeolum is often painful and does not drain easily, so antibiotic eye drops or incision and drainage are often necessary. Delayed treatment carries a risk of progression to eyelid abscess or orbital abscess, so we recommend seeing an ophthalmologist as soon as possible.
External hordeolum develops when acute purulent inflammation occurs in the Zeis glands (sebaceous glands) and Moll glands (sweat glands) that open at the base of the eyelashes. Obstruction of the gland ducts or stagnation of secretions allows resident bacteria (mainly Staphylococcus aureus) to proliferate, triggering acute inflammation. As inflammation progresses, an abscess forms, and a pus point appears on the skin side.
Internal hordeolum develops when acute purulent inflammation occurs in the meibomian glands that run vertically within the tarsal plate. When meibomian gland dysfunction (MGD) is present locally, duct obstruction and changes in secretion properties occur, creating a favorable environment for bacterial infection. Compared to external hordeolum, internal hordeolum is located deeper anatomically, causing more severe pain and making spontaneous drainage difficult.
The causative bacteria of hordeolum are mainly resident bacteria of the conjunctival sac. Staphylococcus aureus is the most common, and its pathogenicity (toxin production and tissue invasiveness) contributes to the severity of acute inflammation. CNS (coagulase-negative staphylococci), Propionibacterium acnes, and Corynebacterium species are less pathogenic but can cause significant infection in immunocompromised hosts.
If treatment is delayed or inappropriate, or in immunocompromised states, inflammation may extend from within the eyelid beyond the orbital septum, forming eyelid abscess or orbital abscess. In infants, because the orbital septum is not fully developed, inflammation can rapidly spread into the orbit. If orbital cellulitis develops, there is a risk of visual impairment, eye movement disorders, and intracranial complications, requiring early systemic antibiotic administration and hospital management.
When a meibomian gland cyst (intratarsal keratinous cyst of the meibomian gland) is complicated by bacterial infection, it may present a clinical picture similar to internal hordeolum.
In cases where severe inflammation persists or recurs, redness and a mass may remain on the eyelid margin. Repeated infections can lead to fibrosis and scarring of the tarsal plate, potentially causing eyelid deformity. Additionally, after acute inflammation subsides, granulomatous changes may persist and transition to a chalazion.
Most cases respond well to antibiotic therapy or surgical treatment and heal without sequelae. In cases where severe inflammation persists or recurs, redness and a mass may remain on the eyelid margin. If treatment is delayed or appropriate treatment is not provided, there is a possibility of progression to eyelid abscess or orbital abscess.
Infants and young children: Frequent follow-up is necessary. Aim for visits every 3–5 days, and respond immediately to enlargement of swelling, fever, or proptosis.
Recurrent or refractory cases: Prioritize investigation for systemic diseases and provide systemic management according to the cause.
Cases with abscess formation: After incision and drainage, continue antibiotic eye drops and follow up until inflammation subsides.
QWhat should I do if I have recurrent styes?
A
Recurrent styes (recurrent hordeolum) may be associated with systemic diseases that affect immune function, such as diabetes or leukemia. It is recommended to undergo blood glucose testing and blood tests during an ophthalmology visit. Daily eyelid cleansing, warm compresses, and thorough hand hygiene are effective in preventing recurrence. Contact lens users should ensure proper care. In refractory cases, specialized treatment for meibomian gland dysfunction (MGD) may be necessary. Additionally, some reports suggest involvement of Demodex (follicle mites), and in recurrent cases, epilation of eyelashes to detect Demodex may be considered.
Alsoudi AF, Ton L, Ashraf DC, Idowu OO, Kong AW, Wang L, Kersten RC, Winn BJ, Grob SR, Vagefi MR. Efficacy of Care and Antibiotic Use for Chalazia and Hordeola. Eye Contact Lens. 2022;48(4):162-168. doi:10.1097/ICL.0000000000000859. PMID: 35296627. PMCID: PMC8931268.
Jun SY, Choi YJ, Lee BR, Lee SU, Kim SC. Clinical characteristics of Demodex-associated recurrent hordeola: an observational, comparative study. Sci Rep. 2021;11(1):21398. doi:10.1038/s41598-021-00599-7. PMID: 34725365. PMCID: PMC8560857.
Yang S, Wu BC, Cheng Z, Li L, Zhang YP, Zhao H, Zeng HM, Qi DF, Ma ZY, Li JG, Han R, Qu FZ, Luo Y, Liu Y, Chen XL, Dai HM. The Microbiome of Meibomian Gland Secretions from Patients with Internal Hordeolum Treated with Hypochlorous Acid Eyelid Wipes. Dis Markers. 2022;2022:7550090. doi:10.1155/2022/7550090. PMID: 35251376. PMCID: PMC8894068.
Rossetto JD, Forno EA, Morales MC, Moreira JC, Ferrari PV, Herrerias BT, Hirai FE, Gracitelli CPB. Upper Eyelid Necrosis Secondary to Hordeolum: A Case Report. Case Rep Ophthalmol. 2021;12(1):270-276. doi:10.1159/000513958. PMID: 34054469. PMCID: PMC8138243.
Knop E, Knop N, Millar T, Obata H, Sullivan DA. The International Workshop on Meibomian Gland Dysfunction: Report of the Subcommittee on Anatomy, Physiology, and Pathophysiology of the Meibomian Gland. Invest Ophthalmol Vis Sci. 2011;52(4):1938-1978. doi:10.1167/iovs.10-6997c. PMID: 21450915. PMCID: PMC3072159.
Takahashi Y, Watanabe A, Matsuda H, Nakamura Y, Nakano T, Asamoto K, Ikeda H, Kakizaki H. Anatomy of secretory glands in the eyelid and conjunctiva: a photographic review. Ophthalmic Plast Reconstr Surg. 2013;29(3):215-219. doi:10.1097/IOP.0b013e3182833dee. PMID: 23381567.
Shimizu Y, Shinji K, Mitoma K, Kiuchi Y, Chikama T. Efficacy of azithromycin hydrate ophthalmic solution for treatment of internal hordeolum and meibomitis with or without phlyctenular keratitis. Jpn J Ophthalmol. 2023;67(5):565-569. doi:10.1007/s10384-023-01010-w. PMID: 37453929.
Foulks GN, Borchman D, Yappert M, Kim SH, McKay JW. Topical azithromycin therapy for meibomian gland dysfunction: clinical response and lipid alterations. Cornea. 2010;29(7):781-788. doi:10.1097/ICO.0b013e3181cda38f. PMID: 20489573. PMCID: PMC2893269.
Luchs J. Efficacy of topical azithromycin ophthalmic solution 1% in the treatment of posterior blepharitis. Adv Ther. 2008;25(9):858-870. doi:10.1007/s12325-008-0096-9. PMID: 18781287.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.