
Chalazion
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is a Chalazion?
Section titled “1. What is a Chalazion?”A chalazion is a disease in which secretions obstruct and accumulate in the meibomian glands, the sebaceous glands of the tarsal plate, leading to a chronic granulomatous inflammation as a foreign body reaction to the degenerated contents. It is fundamentally different from a hordeolum (stye) in that it is a non-infectious inflammation.
Meibomian glands are sebaceous glands located within the tarsal plate that secrete meibum (lipid components), the main component of the tear film lipid layer. This secretion prevents tear evaporation and contributes to ocular surface stability. When the duct of a meibomian gland becomes obstructed, secretions accumulate within the gland duct, forming the basis for chalazion development.
Epidemiology
Section titled “Epidemiology”Chalazion occurs in both children and adults. In children, the eyelid skin (anterior lamella) is fragile, so the lesion tends to infiltrate and expand toward the skin side slightly more.
It is strongly associated with MGD (meibomian gland dysfunction), and chalazion can also be considered a localized form of MGD. In cases of multiple or recurrent chalazia, consider complications of seborrheic dermatitis or rosacea. Both are risk factors for MGD and contribute to chalazion recurrence.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”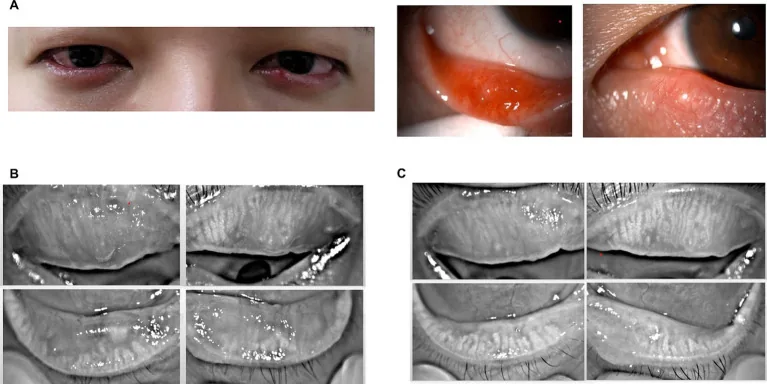
Chronic Phase (Typical Presentation)
Section titled “Chronic Phase (Typical Presentation)”In a typical chalazion, a round, hard mass about the size of a millet seed to a soybean is palpable under the eyelid skin. Localized redness and swelling are present, but there is no spontaneous pain. The mass is located within the tarsal plate, is immobile, and does not adhere to the skin.
Acute Phase
Section titled “Acute Phase”In the acute phase with concurrent infection, eyelid edema, swelling, redness, and lipid leakage occur, accompanied by pain. At this stage, clinical differentiation from internal hordeolum becomes difficult. If spontaneous absorption does not occur, swelling and redness decrease while a painless nodule (chronic granuloma) forms in the center of the eyelid.
Spontaneous Rupture Cases
Section titled “Spontaneous Rupture Cases”- Spontaneous rupture toward the conjunctiva: Polypoid granuloma protrudes from the conjunctival surface
- Spontaneous rupture toward the skin: Granulation tissue is exposed on the skin surface
Spontaneous rupture toward the skin is particularly common in children.
Complications
Section titled “Complications”If left untreated, a chalazion may cause significant swelling and deformity of the eyelid, leading to ptosis or entropion.
Special Considerations in Children
Section titled “Special Considerations in Children”In children, the eyelid skin (anterior lamella) is fragile, so granulomatous inflammation tends to infiltrate and spread toward the skin side. There is a risk of eyelid skin necrosis if removal of the mass is delayed, making it important to start treatment at the appropriate time.
A chalazion is a non-infectious chronic granulomatous inflammation caused by obstruction of the meibomian gland secretion. It forms a painless, hard lump under the eyelid skin and has a relatively slow course. In contrast, a stye is an acute purulent inflammation due to bacterial infection, which is painful and rapidly progresses with redness and swelling. Acute chalazion and internal hordeolum can be difficult to differentiate because symptoms are similar, but in the chronic phase, a painless, elastic lump is characteristic of chalazion.
3. Classification and Types
Section titled “3. Classification and Types”Chalazia are classified into the following four types based on pathology and course.
| Type | Main Features | Key Differentiating Points |
|---|---|---|
| Typical (chronic) chalazion | Painless, hard lump, no redness | Elastic, no adhesion to skin |
| Acute chalazion | Accompanied by pain, redness, and swelling | Difficult to differentiate from internal hordeolum |
| Auto-rupture type (conjunctival side) | Forms polypoid granuloma | Granulation protrusion from conjunctival surface |
| Auto-rupture type (skin side) | Granulation exposed on skin surface | Common in children |
Typical (chronic) chalazion is characterized by a hard, painless mass without redness or pain. On palpation, it is elastic and not adherent to the skin.
Acute chalazion is a condition where inflammation becomes acute due to concurrent infection, accompanied by pain, redness, and eyelid swelling. Clinical differentiation from internal hordeolum is often difficult. After the acute phase subsides, it transitions to a typical chalazion.
In the auto-rupture type, the contents spontaneously drain; when rupture occurs on the conjunctival side, a polypoid granuloma forms. Rupture to the skin side is especially common in children and may lead to eyelid deformity.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Inspection and Palpation
Section titled “Inspection and Palpation”A hard mass is palpable under the eyelid skin. It is elastic and not adherent to the skin. The mass is fixed to the tarsal plate and immobile, which is characteristic.
Eyelid Eversion
Section titled “Eyelid Eversion”Evert the eyelid to observe the conjunctival surface. Assess for conjunctival bulging, redness, and the presence of auto-rupture to the conjunctival side (polypoid granuloma).
Slit Lamp Examination
Section titled “Slit Lamp Examination”Evaluate the degree of astigmatism and corneal epithelial damage caused by corneal compression. Large chalazia can cause irregular astigmatism due to corneal compression.
Differential Diagnosis
Section titled “Differential Diagnosis”Differentiation from sebaceous gland carcinoma — most important
Sebaceous gland carcinoma is very difficult to differentiate from chalazion during short-term follow-up. Strongly suspect sebaceous gland carcinoma if the following findings are present:
- Irregular surface contour on the skin or conjunctival side with irregular proliferation pattern
- Variation in caliber or abnormal course of blood vessels
- More common in the upper eyelid (preferentially occurs in the upper eyelid over the lower eyelid)
- Yellowish-white color due to lipid content
- Contents at incision are not porridge-like but are yellowish-white small granular masses
Observe response to medication, and always perform histopathological examination upon excision.
Other differential diagnoses:
- Internal hordeolum: Symptoms similar to acute chalazion. Acute suppurative inflammation due to bacterial infection.
- Eyelid hemangioma (deep): Requires differentiation in children. Translucent, bluish mass.
- Dacryocystitis: Requires differentiation as a mass near the inner canthus in children.
For recurrent chalazia, consider complications of MGD (meibomian gland dysfunction), seborrheic dermatitis, and rosacea. These are risk factors for MGD and contribute to multiple and recurrent chalazia. In addition, for recurrent cases that are more common in the upper eyelid or those presenting with yellowish-white non-porridge-like contents, differentiation from sebaceous gland carcinoma is important, and histopathological examination should always be performed upon excision.
5. Standard Treatment
Section titled “5. Standard Treatment”5-1. Conservative Treatment
Section titled “5-1. Conservative Treatment”Warm Compress
Apply a towel warmed with hot water to the eyelid for about 10 minutes, then massage the eyelid. Additionally, cleaning the eyelid with eyelid shampoo not only removes abnormal secretions from the eyelid margin but also enhances the effect of warm compresses as the scrubbing acts as eyelid massage. Warm compresses are indicated for early and mild chalazia.
Local Steroid Injection
- Drug: Triamcinolone (triamcinolone acetonide)
- Dose: 0.25 to 0.1 mL
- Route: Injection into the subconjunctiva of the swollen eyelid area
- Effect evaluation: If reduction of the mass is observed 1 to 2 weeks after administration, repeat the injection.
For early and mild chalazia, steroid injection is performed in addition to warm compresses. The effect is limited for fibrotic masses. A meta-analysis (Aycinena et al. 2016, Ophthalmic Plast Reconstr Surg[³]) reported that the single-injection success rate of steroid injection is about 60%, and about 72% with 1-2 injections, while the single-procedure success rate of incision and curettage (I&C) is about 78%, and about 87% with 1-2 procedures, indicating that surgical treatment is superior in terms of response rate and recurrence prevention. On the other hand, a randomized controlled trial for primary chalazia (Ben Simon et al. 2011, Am J Ophthalmol[⁴]) reported no significant difference in efficacy between the two, so selection should be based on individual case characteristics.
5-2. Conservative Treatment in Children
Section titled “5-2. Conservative Treatment in Children”In children, general anesthesia is required, so the threshold for surgical procedures is high. Conservative treatment is often attempted first.
- Antibiotic eye drops may be tried.
- Steroid eye drops are effective, but use low concentrations while monitoring for increased intraocular pressure.
- In cases with multiple or recurrent chalazia, combine topical antibiotic eye drops and oral antibiotics (cephalosporins) from the acute phase.
5-3. Surgical Treatment (Chalazion Excision)
Section titled “5-3. Surgical Treatment (Chalazion Excision)”Surgical excision is indicated when conservative treatment fails, or when the mass is large and affects appearance or function.
Anesthesia
Infiltrate subconjunctival and subcutaneous eyelid tissue with 2% lidocaine hydrochloride (Xylocaine®).
Transconjunctival Approach (Standard Procedure)
This approach avoids skin incision, leaving no skin scar.
- Clamp the chalazion with a chalazion clamp.
- Evert the eyelid to expose the conjunctival surface.
- Identify the location of the chalazion.
- Make a 2–3 mm incision perpendicular to the eyelid margin at the center of the mass.
- The retained porridge-like material (mixture of fat and cellular debris) drains out.
- Scrape out the porridge-like material with gauze or a curette.
- Remove remaining collagen fibers thoroughly with forceps and scissors.
Transcutaneous Eyelid Approach
This approach is selected when there is strong infiltration toward the skin side or when extensive skin treatment is needed in cases of spontaneous rupture.
- Attach a lid speculum
- Make a skin incision approximately 1.5–2 cm near the chalazion, parallel to the eyelid margin
- Dissect the subcutaneous tissue and orbicularis oculi muscle
- Expose the anterior wall of the chalazion directly above the mass
- Incise parallel to the eyelid margin and drain the internal porridge-like contents
- Perform curettage of collagen fibers using a chalazion curette and scissors
5-4. Considerations for pediatric surgery
Section titled “5-4. Considerations for pediatric surgery”- In children, the eyelid skin (anterior lamella) is fragile, so granulomatous inflammation tends to infiltrate and spread to the skin side
- Delaying mass removal carries a risk of progressive necrosis of the eyelid skin
- In children, surgery is generally performed under general anesthesia
- For multiple or recurrent cases, start topical antibiotic eye drops and oral antibiotics (cephalosporins) from the acute phase
Pathological examination of the excised specimen
It is difficult to differentiate between chalazion and sebaceous gland carcinoma through short-term observation. Excised tissue must always be submitted for histopathological examination. Particularly in the following cases, consider the possibility of sebaceous gland carcinoma.
- Mass arising on the upper eyelid
- Recurrent cases
- Cases where incision reveals yellowish-white granular contents rather than porridge-like material
For early and mild chalazia, warm compresses and eyelid massage may improve the condition. The success rate of conservative therapy is reported to be about 80%. Apply a towel warmed with hot water to the eyelid for about 10 minutes, then massage the eyelid. Adding eyelid hygiene (lid scrubs) can enhance the effect. However, for fibrotic masses, conservative therapy has limited efficacy, and surgical excision is necessary.
The standard surgical approach is transconjunctival. Under infiltration anesthesia with 2% lidocaine hydrochloride, the eyelid is everted to expose the conjunctival surface, and a small incision of 2–3 mm perpendicular to the eyelid margin is made at the center of the mass. After curetting the porridge-like material with gauze or a sharp spoon, the remaining collagen fibers are thoroughly debrided with forceps and scissors. Since no skin incision is made, no skin scar remains. Pain during surgery is minimized by local anesthesia.
6. Pathophysiology and Detailed Mechanism
Section titled “6. Pathophysiology and Detailed Mechanism”Normal Function of Meibomian Glands
Section titled “Normal Function of Meibomian Glands”Meibomian glands are sebaceous glands (a type of sebaceous gland) located within the tarsal plate, secreting meibum (lipids), the main component of the tear film lipid layer. Meibum forms an oil layer on the tear surface, preventing tear evaporation and contributing to ocular surface stability. There are approximately 20–30 meibomian glands in each upper and lower eyelid, opening through small pores at the eyelid margin.
Pathogenesis of Chalazion
Section titled “Pathogenesis of Chalazion”- Obstruction of the meibomian gland duct (strongly associated with MGD)
- Accumulation of secretions within the duct. Meibomian gland secretions are a mixture of cellular debris containing fat and keratin.
- A foreign body reaction is triggered against the accumulated degenerative material.
- Chronic granulomatous inflammation with epithelioid cells, multinucleated giant cells, and lymphocyte infiltration occurs.
- Collagen fibers proliferate, fibrosis progresses, and a granuloma (chalazion) is formed.
A key feature of this disease is that bacterial infection is not involved in this pathogenesis.
Histopathology
Section titled “Histopathology”In the histopathology of a chalazion, granulation tissue consisting of neutrophil, lymphocyte, and plasma cell infiltration and capillary proliferation is predominant. Foamy macrophages and epithelioid cells are also partially observed. Connective tissue composed of collagenous tissue surrounds the granulation tissue. This forms the histological basis of the hard mass felt in chronic chalazia.
Relationship with MGD
Section titled “Relationship with MGD”A chalazion can be considered a localized MGD of the meibomian gland. The presence of generalized MGD increases the risk of infarction of multiple gland ducts, leading to multiple and recurrent chalazia. Seborrheic dermatitis and rosacea are important risk factors for MGD, and patients with these conditions are prone to recurrent chalazia. In cases of multiple or recurrent chalazia, management of the underlying disease is also important.
A prospective study using infrared meibography (Li et al. 2020, BMC Ophthalmol[⁵]) showed that even after chalazion healing, meibomian gland dropout persists at the affected site, and the extent depends on the size of the mass, regardless of treatment method (conservative vs. surgical). Additionally, Hanna et al. (2022, Int Ophthalmol[⁶]) reported that meibography showed improvement in meibomian gland parameters of the entire affected eyelid after chalazion excision, suggesting that surgical treatment may also contribute to MGD improvement.
7. Prognosis and Course
Section titled “7. Prognosis and Course”Prognosis of conservative treatment
The success rate of conservative treatment is often reported to be around 80% (Wu et al. 2018, Acta Ophthalmol[¹]). However, in cases where the mass has become fibrotic, the induration of the eyelid cannot be completely eliminated. Continued warm compresses and eyelid hygiene are also effective for preventing recurrence as part of MGD management (Tashbayev et al. 2024, Curr Eye Res[²]).
Prognosis of surgical treatment
The prognosis of surgical treatment is generally good. However, if the curettage of collagen fibers is insufficient, residual induration of the eyelid may persist postoperatively, often leading to patient complaints. Adequate curettage is key to good surgical outcomes.
About recurrence
If MGD is present, the risk of recurrence is high. Instructing patients to continue warm compresses and eyelid hygiene postoperatively is important for preventing recurrence. In cases of multiple or recurrent chalazia, management of seborrheic dermatitis and rosacea should also be performed concurrently.
Risk of missing sebaceous carcinoma
Failure to differentiate from sebaceous carcinoma leads to poor prognosis. It is important to submit all excised specimens for pathological examination. High vigilance is required especially in cases involving the upper eyelid, recurrent cases, and those with non-cheesy contents.
Pediatric considerations
Pay attention to the tendency of infiltration toward the skin side. Delaying surgery increases the risk of eyelid skin necrosis. Surgery under general anesthesia is necessary, but good prognosis can be expected with timely intervention.
8. References
Section titled “8. References”-
Wu AY, Gervasio KA, Gergoudis KN, Wei C, Oestreicher JH, Harvey JT. Conservative therapy for chalazia: is it really effective? Acta Ophthalmol. 2018;96(4):e503-e509. doi:10.1111/aos.13675. PMID: 29338124. PMCID: PMC6047938.
-
Tashbayev B, Chen X, Utheim TP. Chalazion Treatment: A Concise Review of Clinical Trials. Curr Eye Res. 2024;49(2):109-118. doi:10.1080/02713683.2023.2279014. PMID: 37937798.
-
Aycinena ARP, Achiron A, Paul M, Burgansky-Eliash Z. Incision and Curettage Versus Steroid Injection for the Treatment of Chalazia: A Meta-Analysis. Ophthalmic Plast Reconstr Surg. 2016;32(3):220-224. doi:10.1097/IOP.0000000000000483. PMID: 26035035.
-
Ben Simon GJ, Rosen N, Rosner M, Spierer A. Intralesional triamcinolone acetonide injection versus incision and curettage for primary chalazia: a prospective, randomized study. Am J Ophthalmol. 2011;151(4):714-718.e1. doi:10.1016/j.ajo.2010.10.026. PMID: 21257145.
-
Li J, Li D, Zhou N, Qi M, Luo Y, Wang Y. Effects of chalazion and its treatments on the meibomian glands: a nonrandomized, prospective observation clinical study. BMC Ophthalmol. 2020;20(1):278. doi:10.1186/s12886-020-01557-z. PMID: 32652956. PMCID: PMC7353760.
-
Hanna S, Hartstein M, Mukari A, Shor S, Habib G, Hamed Azzam S. Global improvement in meibomian glands after chalazion surgery demonstrated by meibography. Int Ophthalmol. 2022;42(8):2591-2598. doi:10.1007/s10792-022-02307-4. PMID: 35412124.