Trichiasis is a condition where eyelashes, which normally grow outward, grow inward toward the ocular surface. The eyelid and the position of the eyelash roots are normal, but the lashes grow toward the eye, causing erosion of the cornea and conjunctiva, leading to foreign body sensation, discharge, and tearing.
This differs from entropion, where the entire eyelid turns inward. However, entropion is often accompanied by trichiasis. Trichiasis is generally localized, characterized by the presence of misdirected lashes among normally oriented lashes.
Epiblepharon is a condition in infants where congenital excess skin and weak adhesion of subcutaneous tissue cause the eyelid and eyelashes to contact the cornea. Redundancy of the anterior lamella (skin and orbicularis muscle) pushes the entire lash line toward the eyeball. It differs essentially from trichiasis in that the direction of the lashes themselves is not abnormal; rather, the overlying skin is the cause.
Trichiasis is an abnormality in the direction of the eyelashes (often acquired, regardless of the presence of entropion), while epiblepharon is a congenital condition due to excess anterior lamella. Both can coexist, complicating treatment decisions. Additionally, marginal entropion (subtle inward turning of the posterior lid margin) as the essence of trichiasis may present findings similar to epiblepharon.
A condition where eyelashes grow from near the meibomian gland openings (where lashes are normally absent) and the entire lash line turns inward is called distichiasis. It is included in the broad sense of trichiasis and requires a specific surgical technique for treatment.
The exact prevalence of trichiasis is unknown. Globally, trachoma is the leading cause of infectious blindness, affecting about 10 million people. WHO estimates approximately 3.2 million surgeries are pending. Women are affected four times more often than men. Although it can occur in children, it is more common after the 40s. After trachoma declined significantly, age-related changes and chronic blepharitis-associated trichiasis became the main conditions.
Epiblepharon is frequently seen in East Asia (China, Japan, Korea), with the nasal side of the lower eyelid being the typical site.
QWhat is the difference between trichiasis and entropion?
A
Trichiasis is an abnormality in the direction of eyelash growth itself, while the eyelid margin position is normal. In contrast, entropion is a condition where the entire eyelid turns inward, causing the eyelid skin including lashes to contact the ocular surface. Both often coexist, but differentiation is important because treatment strategies differ. Trichiasis is localized, with misdirected lashes among normally oriented ones. Entropion requires surgery to correct the entire eyelid position, whereas trichiasis primarily involves removal or redirection of the lashes.
QHow do epiblepharon and trichiasis differ?
A
Epiblepharon is a congenital condition where excess skin pushes the entire lash line toward the cornea, common in East Asian children. Trichiasis is a condition where individual lashes are misdirected, often due to acquired causes (scarring, inflammation). Both can coexist, but epiblepharon may improve spontaneously with growth, while trichiasis requires electrolysis or surgery for definitive treatment.
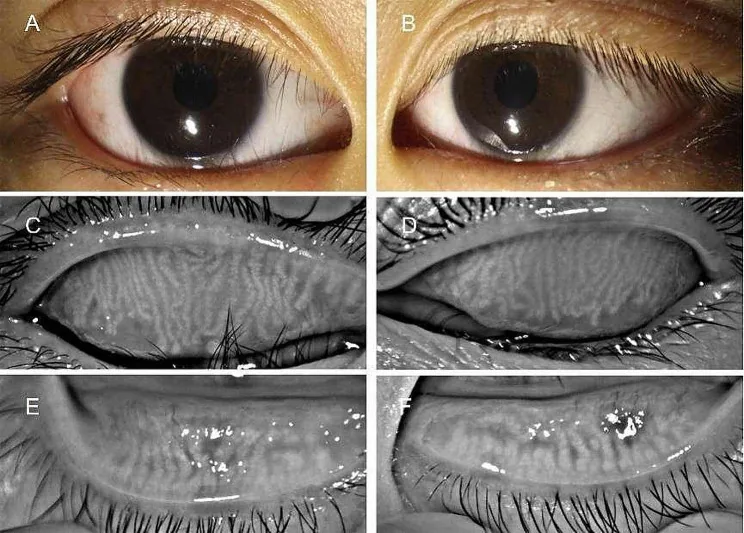
Li J, et al. Morphological and functional characteristics of the meibomian gland in pediatric patients with epiblepharon. BMC Ophthalmol. 2024;24:84. DOI: 10.1186/s12886-024-03345-5. Figure 2. PMCID: PMC10885463. License: CC BY 4.0.
External eye photographs (A, B) showing eyelashes contacting the ocular surface on the nasal side of the lower eyelid in a patient with entropion, and meibography (C–F) showing thinning, dilation, and tortuosity of the upper eyelid meibomian glands. This corresponds to the eyelash-ocular contact and corneal damage discussed in the section “Main Symptoms and Clinical Findings.”
Abnormal eyelash direction: Eyelashes pointing inward are found among normally directed lashes. A habit of observing the entire eyelid at low magnification helps prevent oversight.
Corneal erosion and punctate keratopathy: Fluorescein staining reveals punctate keratopathy at the site of eyelash contact.
Corneal thinning and opacity: Long-standing cases may develop corneal thinning and opacity.
In epiblepharon, the skin overhangs on the nasal side of the lower eyelid, giving the appearance that the entire lash line contacts the cornea. In infants, symptoms become apparent when crying or looking downward. Fluorescein staining can reveal punctate keratopathy in the lower cornea.
Trauma or inflammatory scarring can also cause trichiasis. In trachoma, conjunctival scarring from repeated infections is the main cause of trichiasis1). After Stevens-Johnson syndrome (SJS), the eyelash loss phase transitions to a disorganized growth phase, requiring long-term epilation.
Long-term use of prostaglandin analog eye drops can cause eyelashes to grow longer, curl, and lead to symptoms of trichiasis. In patients using PG analogs for glaucoma treatment, regular eyelid examination is important.
Chemotherapeutic agents such as docetaxel (taxane) and trastuzumab have been reported to cause cicatricial entropion and trichiasis3). Histopathology shows chronic inflammation, dermal fibrosis, and squamous metaplasia 3).
Childhood epiblepharon is common in East Asia. Overall, trichiasis increases after the age of 40, with age-related eyelid laxity and chronic blepharitis being major causes in Japan.
QCan chemotherapy cause trichiasis?
A
Cases of cicatricial entropion and trichiasis caused by docetaxel (taxane anticancer drug) and trastuzumab (anti-HER2 monoclonal antibody) have been reported 3). After administration, chronic inflammation of the upper eyelid occurs, and squamous metaplasia of the meibomian glands leads to trichiasis and cicatricial entropion3). Histopathology shows chronic inflammation, dermal fibrosis, and abnormal epithelial differentiation 3). It is refractory and recurs even after multiple surgeries, so early management through collaboration between oncologists and ophthalmologists is recommended 3).
Slit-lamp examination: Observe the entire eyelid at low magnification to check for abnormal eyelash direction. Using a diffuser makes findings easier to detect.
Fluorescein staining: Reveals punctate keratopathy and corneal erosion at the contact area of the eyelashes. It is important to perform this simultaneously with examination of the ocular surface.
Patient history: Ask about the frequency of foreign body sensation. The eyelash growth cycle (approximately one month) can guide the timing of follow-up visits. Also check whether the patient has pulled out eyelashes themselves.
Differential Diagnosis and Precautions
Differentiation from entropion: Trichiasis is localized and the eyelid position is normal. In some cases, entropion becomes apparent only after forced eyelid closure followed by opening, so observe in conjunction with corneal and conjunctival findings.
Blink test: Pull the lower eyelid downward to correct entropion, then ask the patient to blink. If entropion occurs with blinking, it is involutional entropion; if it returns to entropion regardless of blinking, it is cicatricial entropion.
Exclusion of malignancy: Trichiasis may be the initial symptom of a malignant eyelid margin tumor. Caution is needed if accompanied by eyelash loss.
Eyelash epilation: The simplest management method. Remove with forceps under a slit lamp microscope. Since eyelashes regrow after 1–2 months, regular removal is required. Surgery is needed for a permanent cure.
Artificial tears and eye ointment: Prescribed as adjunctive treatment for corneal epithelial damage. If corneal erosion is present, use hyaluronic acid eye drops.
Therapeutic contact lenses: May be used for corneal protection.
Surgical treatment
Electrolysis of eyelashes: The procedure itself is simple, but since the hair root is not coagulated under direct visualization, the recurrence rate is high. Not suitable for many misdirected lashes. Contraindicated in patients with cardiac pacemakers; consider photocoagulation or cryocoagulation.
Hair root resection: There are methods to remove one hair at a time or multiple hairs at once. Ensure removal of the hair root just above the tarsal plate.
Lash migration surgery: Machek method (moving the abnormal eyelash area with Z-plasty) and Spencer-Watson method.
Tarsal rotation surgery: For trachomatous trichiasis, BLTR (bilamellar tarsal rotation) and PLTR (posterior lamellar tarsal rotation) are recommended 1).
Eyelash epilation is performed with the patient seated, observed under a slit lamp microscope. Anesthetic eye drops are generally not required, but they can be effective for patients who complain of pain or dislike having their eyelids touched. Gently remove the lashes, taking care not to break them midway.
Insurance billing is done as J089 Eyelash epilation. It is classified as an ophthalmic procedure, not surgery. It can be billed once per day: up to 4 lashes is billed as “1”, and 5 or more as “2”. It cannot be billed simultaneously with other procedures. The eyelash growth cycle is approximately one month, so regular visits aligned with this cycle are desirable.
In surgeries that involve skin incisions, there are partial resection of the lash line and eyelid splitting. In eyelid splitting, the anterior lamella containing the lash roots is separated from the tarsal plate, the lash line is excised along with the roots, and the remaining anterior lamella is shifted posteriorly and fixed. This is chosen when there are many misdirected lashes or when electrolysis causes repeated recurrence.
Eyelash electrolysis is unsuitable for treating many misdirected lashes because of pain with insufficient anesthesia and high recurrence rates due to inability to coagulate the hair root under direct visualization. It is positioned as an adjunctive option for localized, few misdirected lashes.
In trachomatous trichiasis, a single postoperative oral dose of azithromycin reduces the risk of recurrence by 18% compared to six weeks of tetracycline eye ointment (OR 0.82, 95% CI 0.69–0.99) 1).
For localized cicatricial entropion and trichiasis, the buccal plug technique using a buccal mucosal graft has been reported 2). It avoids conjunctival incision and mechanically separates the anterior and posterior lamellae to eliminate corneal contact of lashes 2). No recurrence was observed in all 4 cases during a mean follow-up of 5.16 months 2).
Observation: Many cases improve spontaneously with growth, so observation is chosen for mild cases. If corneal epithelial damage is minimal and there is no effect on visual development, artificial tears and regular follow-up are used.
Surgical indications: Surgery is considered when corneal epithelial damage persists and there is concern about effects on visual development. Generally, intervention is performed if the condition does not improve by school age (around 4–6 years old) or if corneal damage progresses.
Hotz modification: This is a representative surgical technique that excises and shortens the anterior lamella (skin and orbicularis oculi muscle) to correct the direction of the eyelashes. Excess skin is removed through a skin incision, and the eyelashes are adjusted to point outward.
QWhat is the recurrence rate of trichiasis after surgery?
A
In a systematic review and meta-analysis of trachomatous trichiasis, the pooled postoperative recurrence rate was 19% (range 18–21%) 1). Risk factors for recurrence included older age (OR 0.63 for younger age group indicating lower risk), higher preoperative severity (major trichiasis associated with higher risk), and use of tetracycline eye ointment postoperatively (single-dose azithromycin associated with lower recurrence, OR 0.82) 1). Although WHO recommends a rate below 10%, many studies report recurrence rates exceeding this threshold 1).
QWhat is the buccal plug technique?
A
The buccal plug technique is a minimally invasive surgical approach for localized cicatricial entropion and trichiasis2). After separating the anterior and posterior lamellae, a square portion of the anterior lamella containing the problematic eyelash follicles is excised, and a buccal mucosal graft harvested from the lower lip is inserted as a “plug” to mechanically separate the lamellae 2). Advantages include avoiding a conjunctival incision and minimal impact on the aesthetic contour of the eyelid 2). However, it is not indicated for extensive cicatricial lesions and is positioned as an adjunctive option for localized lesions 2).
The pathology of trichiasis is a condition in which the mucocutaneous junction of the eyelid is displaced anteriorly due to many cases of blepharitis or blepharoconjunctivitis, and slight entropion of the posterior lid margin (marginal entropion) affects the hard fibrous tissue at the hair root, changing the direction of eyelash growth. This subtle inversion of the eyelid margin is difficult to notice on routine visual inspection but manifests clinically as abnormal eyelash direction.
When eyelashes contact the cornea, repeated micro-damage to the corneal epithelium occurs. Chronic irritation can progress to corneal epithelial keratinization, thinning, and perforation. Formation of pseudopterygium and induction of corneal astigmatism are understood as tissue reactions of the ocular surface due to long-term eyelash contact. Ultimately, corneal opacity leads to vision loss.
In trichiasis caused by chemotherapy drugs (docetaxel, trastuzumab), the drugs induce chronic inflammation and interstitial fibrosis in the eyelid tissue 3). Decreased conjunctival goblet cells cause severe dry eye, and squamous metaplasia of the mucosa progresses 3). Abnormal differentiation from non-keratinized stratified epithelium to non-secretory keratinized epithelium leads to meibomian gland degeneration, trichiasis, and cicatricial entropion3).
Trachomatous trichiasis results from conjunctival scarring due to repeated infection with C. trachomatis. Contraction of scar tissue causes the eyelid margin and lashes to turn inward, contacting the cornea1). Postoperative recurrence is associated with persistent active conjunctival inflammation, age-related degenerative changes in eyelid tissue, and the severity of preoperative trichiasis1).
The essence of epiblepharon is excess skin and weak attachment of subcutaneous tissue. The excess anterior lamella pushes the entire lash line toward the eyeball. As the child grows, the orbital volume expands and facial bones develop, relatively resolving the skin excess, causing the lashes to turn outward, leading to spontaneous improvement. This is why many cases of epiblepharon in East Asian children resolve naturally by school age.
If the eyelash root is surgically removed, the prognosis is good. If surgery is not performed, regular epilation of lashes is necessary. If corneal opacity has occurred, the visual prognosis depends on the degree of corneal pathology rather than the trichiasis itself.
Many cases improve spontaneously with growth, and in most cases, symptoms of trichiasis disappear around school age. In mild cases, observation with artificial tears is sufficient for most patients. If corneal epithelial damage persists and there is concern about visual development, surgery such as the Hotz procedure can improve symptoms.
After Stevens-Johnson syndrome, the eyelashes transition from the shedding phase to the disorganized growth phase, requiring long-term epilation. Even after inflammation subsides, disorganized growth often persists, and surgical treatment may be necessary.
A meta-analysis integrating 18 studies revealed that the pooled postoperative recurrence rate of trachomatous trichiasis is 19% 1). Postoperative administration of a single dose of azithromycin significantly reduced the recurrence rate (OR 0.82) 1). Regular surgical skills training, close postoperative follow-up, and patient education are considered essential for preventing recurrence 1).
The buccal plug technique has been reported as a minimally invasive approach that avoids conjunctival incision 2). Compared to conventional tarsal rotation surgery, it has less aesthetic impact and may be a useful option for localized cicatricial entropion and trichiasis2).
Multiple cases of cicatricial entropion and trichiasis caused by docetaxel and trastuzumab have been reported 3). As long as the chronic inflammatory process persists, recurrence occurs even after surgery, so an approach prioritizing conservative management and waiting for the inflammatory process to subside has been proposed 3). Early intervention through collaboration between oncologists and ophthalmologists is important 3).
Adimassu NF, Assem AS, Fekadu SA. Postoperative trachomatous trichiasis: a systematic review and meta-analysis study. International health. 2023;15(6):623-629. doi:10.1093/inthealth/ihad014. PMID:36852770; PMCID:PMC10629961.
Saffari PS, Roelofs KA, Rootman DB. The buccal plug: A technique for management of focal cicatricial entropion and trichiasis. Indian J Ophthalmol. 2025;73:305-306.
Galindo-Ferreiro A, de Prado Otero DS, Marquez PIG, Schellini S. Recurrent and recalcitrant upper lid cicatricial entropion following combined chemotherapy: Clinical and pathology correlation. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2021;35(4):347-349. doi:10.4103/1319-4534.347308. PMID:35814986; PMCID:PMC9266477.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.