Eye pain and foreign body sensation (grittiness) are among the most common complaints in ophthalmology clinics. The causes range from everyday mild conditions such as dry eye or minor corneal abrasions to vision-threatening ophthalmic emergencies like acute angle-closure glaucoma attack, endophthalmitis, and posterior scleritis.
The eye is composed of tissues with different sensitivities, including the cornea, sclera, uvea, and optic nerve. The nature of the pain sharply reflects the site of the lesion. Superficial (corneal or conjunctival) disorders cause a gritty or foreign body sensation, inflammation of the sclera or iris produces a dull ache or tenderness, and a rapid rise in intraocular pressure is characterized by throbbing severe pain with headache and nausea. By combining the nature of the pain with accompanying symptoms, high-urgency diseases can be identified without being missed.
Eye pain is a leading complaint in ophthalmic emergencies, and eye pain accompanied by vision loss is particularly urgent 1). Dry eye has a high prevalence of 25–30% and is one of the most common causes of eye pain and foreign body sensation. Meanwhile, acute angle-closure glaucoma is an emergency common in East Asian women, and delay in treatment leads to irreversible optic nerve damage. Necrotizing scleritis has a blindness rate of about 40% and is the most severe category of scleritis.
Comprehensive evaluation of the nature, location, onset pattern, accompanying symptoms, contact lens use history, and systemic disease background is the first step for appropriate consultation behavior and treatment selection.
2. Anatomical Classification of Eye Pain and Foreign Body Sensation
Classifying eye pain and foreign body sensation from an anatomical perspective—based on which tissue it originates from—facilitates determination of consultation urgency and narrowing of differential diagnoses.
Superficial (ocular surface, conjunctiva, cornea)
Main symptoms: Gritty sensation, foreign body sensation, feeling of sand in the eye
Pain originating from the cornea, conjunctiva, or ocular surface epithelium is often perceived as a foreign body sensation or gritty feeling. The corneal epithelium is densely innervated by trigeminal nerve endings, so even minor injury can cause intense discomfort 6). If symptoms temporarily improve with blinking, dry eye is suspected; if persistent, foreign body or epithelial damage should be considered.
Main symptoms: Deep dull pain, tenderness, irritation, burning sensation
Inflammation of the sclera, episclera, or anterior uvea typically presents with a dull ache or pressure sensation felt throughout the eye. Episcleritis is characterized by transient irritation, burning, or mild foreign body sensation without significant pain or tenderness, whereas scleritis often presents with hyperemia and eye pain, and many patients report tenderness or throbbing severe pain. Iridocyclitis (anterior uveitis) is accompanied by ciliary injection and photophobia.
Representative diseases: Episcleritis (irritation, burning, often painless), anterior scleritis (diffuse or nodular: throbbing pain), iridocyclitis
Deep (elevated intraocular pressure, posterior segment, orbit)
Main symptoms: Severe eye pain, headache, nausea, pain with eye movement
Rapid elevation of intraocular pressure or inflammation of the posterior globe or orbit can cause severe pain around the eye, headache, and nausea. In acute angle-closure glaucoma attacks, intraocular pressure reaches 40–80 mmHg, and headache and vomiting may lead to misdiagnosis as gastrointestinal or cerebrovascular disease. Pain with eye movement is an important sign of posterior scleritis, optic neuritis, and orbital cellulitis.
Representative diseases: Acute angle-closure glaucoma attack (emergency), endophthalmitis (postoperative or post-traumatic: severe pain + vision loss), posterior scleritis (pain with eye movement), optic neuritis, orbital cellulitis3)
3. Main causes of eye pain (differential diagnosis table)
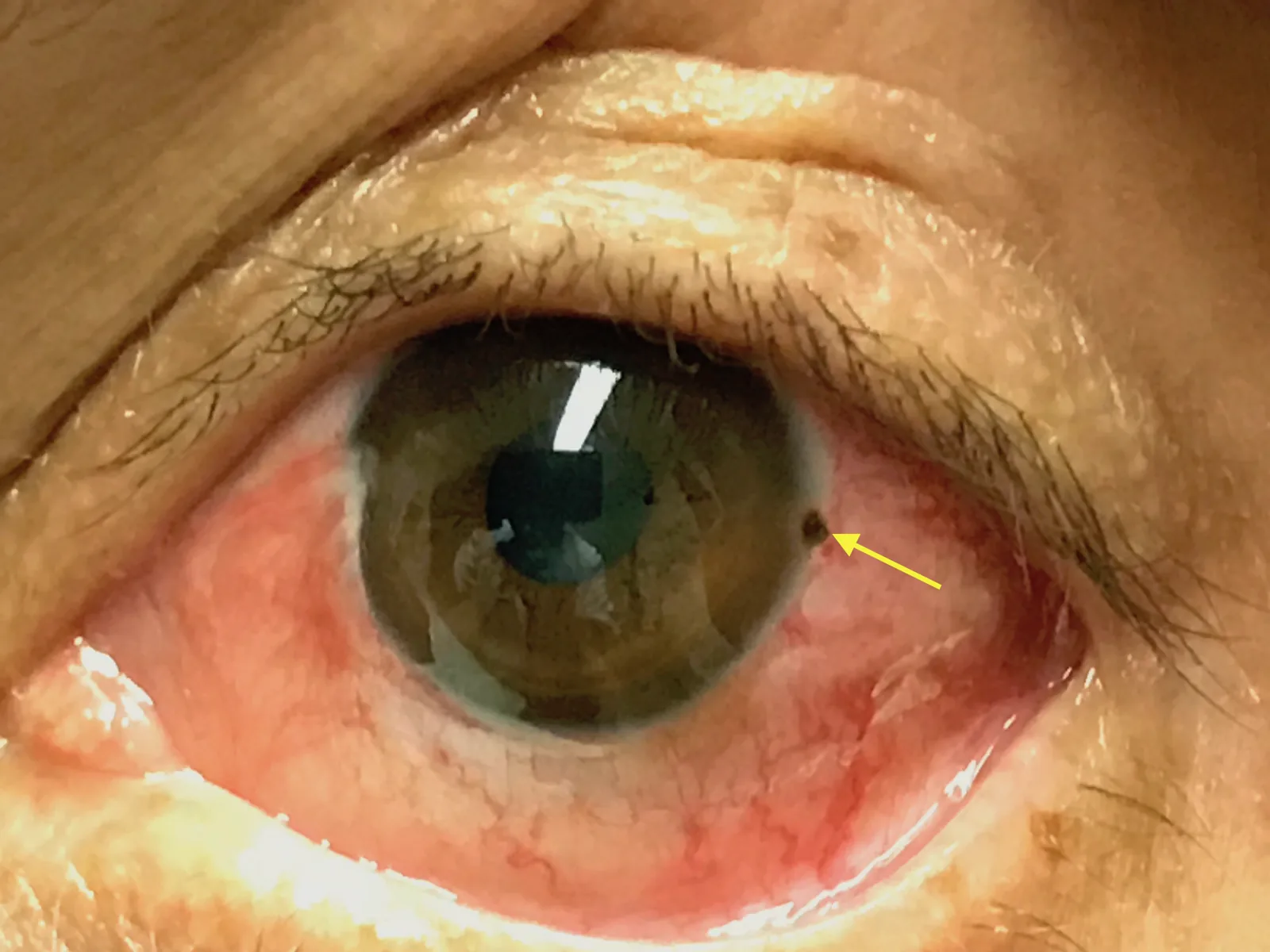
Zakaria J, Peña J. Corneal Rust Ring. JETem. 2018;3(4). DOI: 10.21980/J8X067. Figure 1. Source ID: JETem2018-corneal-rust-ring. License: CC BY 4.0.
Slit-lamp photograph of a metallic foreign body embedded in the cornea at the 3 o’clock position of the left eye, with a surrounding rust ring (arrow). This corresponds to the corneal foreign body discussed in section “3. Main causes of eye pain (differential diagnosis table).”
The main differential diagnoses are organized by the combination of pain characteristics, accompanying symptoms, and urgency.
Dry eye – The ocular surface epithelium is damaged due to quantitative or qualitative instability of the tear film. Impairment of the mucin, aqueous, or lipid layer causes foreign body sensation, dryness, and eye fatigue. A characteristic feature is temporary relief of foreign body sensation after blinking; symptoms worsen with prolonged VDT (computer/smartphone) use and dry air conditioning environments. The prevalence is 25–30%, making it one of the most common causes of eye pain.
Corneal foreign body – Metal fragments, sand grains, etc., may become embedded in the cornea during metalworking, woodworking, or outdoor activities in windy conditions. The foreign body is identified using a slit lamp. Iron fragments may form a rust ring due to iron oxide, and incomplete removal delays healing. Self-removal of a corneal foreign body carries a risk of corneal perforation; therefore, removal by an ophthalmologist is always necessary 5).
Contact lens (CL)-related keratitis Eye pain and foreign body sensation in CL wearers may indicate infectious keratitis and should not be underestimated. In particular, Acanthamoeba keratitis can develop from wearing CLs in tap water or swimming pools, and severe cases may require corneal transplantation 2). If eye pain occurs while wearing CLs, it is advisable not only to remove them and observe but also to see an ophthalmologist within the next day.
Episcleritis Inflammation of the episcleral tissue (the scleral surface within 3 mm of the corneal limbus). There are diffuse and nodular types. Differentiation from conjunctivitis can be problematic and is determined by the number and mobility of nodules, presence of pain and tenderness, and response to epinephrine eye drops. Most cases are benign and resolve spontaneously within days to weeks without treatment.
Scleritis Inflammation of the full thickness of the sclera, primarily involving autoimmune mechanisms. It often accompanies systemic autoimmune diseases such as rheumatoid arthritis, SLE, and HLA-B27-related conditions. The redness is dark red, and observation under natural light is important. The fact that redness does not subside with epinephrine eye drops is useful for differentiating from episcleritis. Necrotizing scleritis is severe, with a blindness rate of about 40%, and requires systemic evaluation and aggressive treatment 8).
Acute angle-closure glaucoma attack An ophthalmic emergency in which the angle (the boundary between the iris and cornea) rapidly closes, obstructing aqueous humor outflow and causing a sudden rise in intraocular pressure. Intraocular pressure reaches 40 mmHg or higher (60–80 mmHg in severe cases), causing severe eye pain, redness, blurred vision due to corneal edema, headache, nausea, and vomiting. Because headache and vomiting are prominent, it may be misdiagnosed as gastrointestinal or cerebrovascular disease, so caution is needed. More common in East Asian women.
QHow can we differentiate between the foreign body sensation of dry eye and that of a corneal foreign body?
A
The foreign body sensation due to dry eye is temporarily relieved by blinking, is relatively mild in the morning, and tends to worsen after prolonged reading or computer use. It often occurs in both eyes and is associated with dry environments and prolonged VDT use.
In contrast, the foreign body sensation from a corneal foreign body is constant and does not improve with blinking. It is accompanied by redness, tearing, and photophobia (sensitivity to light), and the timing of the foreign body entry (contact with sand, metal fragments, wood chips, etc.) can often be identified.
If you are unsure or if symptoms persist the next day, we strongly recommend seeing an ophthalmologist. Leaving a corneal foreign body untreated can lead to infection and scar formation.
The following history-taking items are important for narrowing down the cause of eye pain and foreign body sensation. Please use them as a reference when organizing your own or your family’s symptoms.
Onset pattern: Sudden (acute) or gradual (chronic). Acute onset of eye pain suggests a high likelihood of an emergency condition.
Unilateral or bilateral: Bilateral gritty sensation and dryness suggest dry eye or eye drop toxicity. Unilateral severe pain suggests glaucoma attack, scleritis, or endophthalmitis.
Contact lens (CL) use: Type of CL, daily wearing time, care method, history of exposure to tap water.
Occupation and trauma history: Metalworking, woodworking, welding, sports, etc. Essential for assessing the possibility of foreign body entry.
Presence of systemic diseases: Rheumatoid arthritis, SLE, HLA-B27-related (ankylosing spondylitis, Behçet’s disease, etc.), thyroid disease, tuberculosis, etc. Closely associated with scleritis and uveitis.
Surgery and trauma history: Worsening eye pain after intraocular surgery such as cataract surgery or vitrectomy suggests endophthalmitis.
History of using over-the-counter and prescription eye drops: Preservatives (e.g., benzalkonium chloride) in OTC eye drops can cause corneal epithelial damage, leading to foreign body sensation and eye pain4).
Presence of photophobia (sensitivity to light): An important sign of iridocyclitis, keratitis, and glaucoma attack.
Changes in vision: Eye pain accompanied by vision loss significantly increases urgency1).
Mild foreign body sensation (improves with blinking)
See an ophthalmologist if not improved in a few days
QI feel like something is in my eye but cannot find it. Should I see a doctor?
A
It is common to have a foreign body sensation without visible debris. Minor corneal epithelial damage (e.g., punctate epithelial erosions) may not be visible to the naked eye but can be detected with a slit lamp and fluorescein staining.
Contact lens wearers should remove the lens immediately. If symptoms do not improve by the next day, an eye exam is recommended. If accompanied by redness, photophobia, or vision loss, seek care the same day. Persistent foreign body sensation lasting more than a week may be due to dry eye; artificial tears and lifestyle changes can be effective.
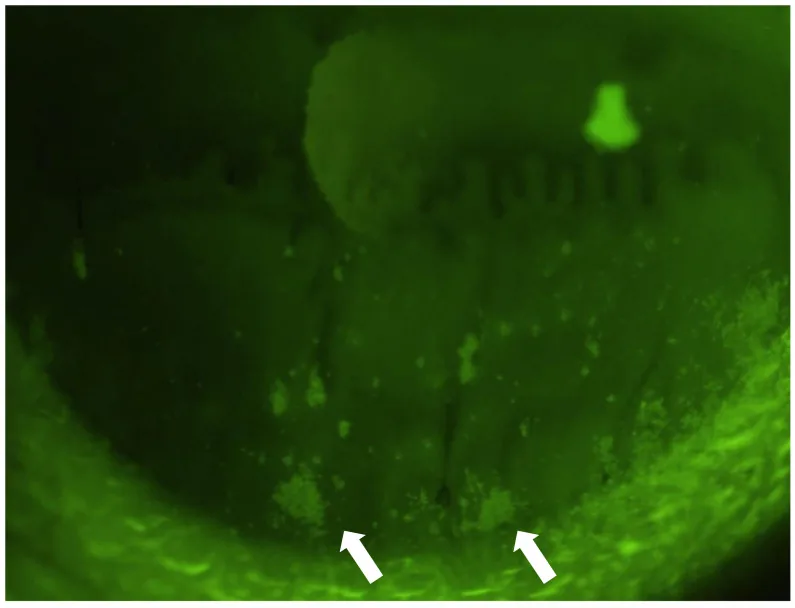
Komai S, Yokoi N, Kato H, et al. Clinical Implication of Patchy Pattern Corneal Staining in Dry Eye Disease. Diagnostics (Basel). 2021;11(2):232. Figure 1. PMCID: PMC7913618. License: CC BY.
Slit-lamp photograph of a dry eye patient showing punctate and patchy fluorescein staining (white arrows) on the inferior cornea, a pattern distinct from typical punctate keratopathy. Corresponds to dry eye discussed in section “6. Pathophysiology of Eye Pain.”
The mechanisms of eye pain and foreign body sensation vary by disease. Representative pathologies are summarized below.
Corneal innervation and pain sensitivity The cornea is one of the most densely innervated tissues in the body, receiving rich innervation from the trigeminal nerve (ophthalmic branch). Due to this high nerve density, even minor epithelial injury, dryness, or foreign bodies can cause intense foreign body sensation and pain 6). The TFOS DEWS II Pain and Sensation Report organizes the concept of neuropathic ocular pain in dry eye and shows that neuronal sensitization contributes to chronic foreign body sensation and eye pain 6).
Dry eye – Quantitative or qualitative instability of the tear film damages the ocular surface epithelium. The tear film has a three-layer structure: lipid, aqueous, and mucin layers. Abnormalities in any layer shorten tear break-up time (BUT) and cause ocular surface dryness. As epithelial damage progresses, punctate superficial keratopathy (SPK) develops, lowering the corneal sensitivity threshold and intensifying foreign body sensation and eye pain, creating a vicious cycle.
Episcleritis – Histopathologically, it is non-granulomatous, mainly involving vasodilation and lymphocytic infiltration. Because inflammation is confined to the episcleral tissue, symptoms are milder than in deep scleritis, and it tends to resolve spontaneously.
Scleritis – Inflammation of the full thickness of the sclera, primarily driven by autoimmune mechanisms. The sclera is an avascular dense connective tissue; once inflammation occurs, it can lead to necrosis and perforation. Approximately 50% of cases are associated with systemic autoimmune diseases such as rheumatoid arthritis, SLE, HLA-B27-related diseases, and granulomatosis with polyangiitis (GPA). Necrotizing scleritis causes the sclera to thin and appear bluish-black, and the visual prognosis is particularly poor8).
Acute angle-closure glaucoma attack – Pupillary block (adhesion between the posterior iris and anterior lens) increases posterior chamber pressure, causing the iris to bulge forward (iris bombé) and rapidly occlude the peripheral angle. Inability to drain aqueous humor leads to a sharp rise in intraocular pressure (≥40 mmHg), impairing blood flow to the optic nerve head. Persistent optic nerve ischemia due to high intraocular pressure results in irreversible optic nerve damage and visual field loss. It is more common in East Asian women, with hyperopia, shallow anterior chamber, and small cornea as anatomical risk factors.
Ocular surface damage from preservatives in over-the-counter eye drops – Preservatives such as benzalkonium chloride (BAC) in over-the-counter eye drops, when used frequently, reduce mucin expression in the corneal epithelium and impair epithelial barrier function. Long-term use of multiple medications can cause toxic keratopathy, leading to chronic foreign body sensation and eye pain4).
New treatments for dry eye – Diquafosol sodium (3%, 6 times daily) and rebamipide (2%, 4 times daily) are becoming widely used as dry eye treatments with novel mechanisms of action, in addition to conventional artificial tears and hyaluronic acid eye drops. Diquafosol promotes tear secretion and mucin secretion from goblet cells via P2Y2 receptors, and its correspondence with a new dry eye classification based on fluorescein staining patterns is being investigated7).
Epidemiological changes in contact lens-related infections With the increase in CL use and generalization of long-term wear, the incidence of Acanthamoeba keratitis is on the rise. In particular, it has been clarified that CL care (storage and cleaning) using tap water significantly increases the risk 2), and the importance of appropriate CL care guidance and regular checkups is being reaffirmed.
Biologics for scleritis For refractory scleritis associated with autoimmune diseases such as rheumatoid arthritis and vasculitis, the efficacy of biologics such as TNF-α inhibitors (infliximab, adalimumab) and IL-6 receptor antagonists (tocilizumab) has been reported 8). They have become positioned as an option for cases difficult to control with systemic steroid administration.
Standardization of ocular pain assessment scales To objectively quantify chronic ocular surface pain and foreign body sensation, reliability and validity verification of patient-reported outcome (PRO) measures such as the Ocular Pain Assessment Survey (OPAS) is progressing 9). Elucidation of the neuropathic mechanisms of ocular pain and identification of therapeutic targets are expected to lead to improved treatment of refractory dry eye-related pain.
Galor A, Levitt RC, Felix ER, Martin ER, Sarantopoulos CD. Neuropathic ocular pain: an important yet underevaluated feature of dry eye. Eye (London, England). 2015;29(3):301-12. doi:10.1038/eye.2014.263. PMID:25376119; PMCID:PMC4366454.
Carnt N, Stapleton F. Strategies for the prevention of contact lens-related Acanthamoeba keratitis: a review. Ophthalmic Physiol Opt. 2016;36(2):109-124.
Theodora Tsirouki, Anna I. Dastiridou, Nuria Ibánez flores, Johnny Castellar Cerpa, Marilita M. Moschos, Periklis Brazitikos, Sofia Androudi. Orbital cellulitis. Survey of Ophthalmology. 2018;63(4):534-553. doi:10.1016/j.survophthal.2017.12.001.
Baudouin C, Labbé A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Progress in retinal and eye research. 2010;29(4):312-34. doi:10.1016/j.preteyeres.2010.03.001. PMID:20302969.
Ahmed F, House RJ, Feldman BH. Corneal Abrasions and Corneal Foreign Bodies. Primary care. 2015;42(3):363-75. doi:10.1016/j.pop.2015.05.004. PMID:26319343.
Belmonte C, Nichols JJ, Cox SM, Brock JA, Begley CG, Bereiter DA, et al. TFOS DEWS II pain and sensation report. The ocular surface. 2017;15(3):404-437. doi:10.1016/j.jtos.2017.05.002. PMID:28736339; PMCID:PMC5706540.
Yokoi N, Georgiev GA, Kato H, Komuro A, Sonomura Y, Sotozono C, et al. Classification of Fluorescein Breakup Patterns: A Novel Method of Differential Diagnosis for Dry Eye. American journal of ophthalmology. 2017;180:72-85. doi:10.1016/j.ajo.2017.05.022. PMID:28579061.
Sims J. Scleritis: presentations, disease associations and management. Postgrad Med J. 2012;88(1046):713-718. doi:10.1136/postgradmedj-2011-130282.
Qazi Y, Hurwitz S, Khan S, Jurkunas UV, Dana R, Hamrah P. Validity and Reliability of a Novel Ocular Pain Assessment Survey (OPAS) in Quantifying and Monitoring Corneal and Ocular Surface Pain. Ophthalmology. 2016;123(7):1458-68. doi:10.1016/j.ophtha.2016.03.006. PMID:27089999; PMCID:PMC5512896.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.