Herpes zoster ophthalmicus (HZO) is a viral disease caused by reactivation of varicella-zoster virus (VZV) in the area supplied by the first division of the trigeminal nerve (ophthalmic nerve). It is characterized by unilateral painful vesicular rash and causes various complications in the eye and ocular adnexa.
VZV, like herpes simplex virus (HSV), belongs to the Alphaherpesvirinae subfamily. Primary infection occurs as chickenpox, after which the virus becomes latent in the dorsal root ganglia and trigeminal ganglia. Over years, with declining immune function, the virus reactivates and reaches the skin and ocular tissues via nerve axons. Since VZV is rapidly inactivated outside cells, the rash is limited to the innervated area and shows a dermatomal distribution. Unlike HSV, VZV reactivation usually occurs only once in a lifetime, but complications are diverse and tend to be severe.
Among reactivated herpes zoster, cases occurring in the first division of the trigeminal nerve are called “herpes zoster ophthalmicus,” which can be complicated by various types of keratitis, conjunctivitis, scleritis, uveitis, secondary glaucoma, ocular muscle palsy, retinitis, and other ocular complications.
The global incidence of herpes zoster increases with age: 5.15 per 1,000 person-years at age 50–54 and 11.27 per 1,000 person-years at age 85 and older 1). Among patients with herpes zoster, HZO occurs in 4–20%1). In the United States, the incidence of HZO in adults aged 50 years and older is 54.6–131.6 per 100,000 person-years, increasing by 3.6% annually 1). Women have a higher incidence of HZO than men (44.5 vs. 33.1 per 100,000 person-years) 1).
Herpes zoster is said to occur in people aged 50 and older, particularly the elderly, patients with diabetes, cancer patients, and those with reduced immunity due to long-term use of steroids or immunosuppressants. It also frequently occurs as an opportunistic infection in HIV infection, but can also occur in completely healthy individuals. The Japanese Infectious Keratitis Clinical Practice Guidelines, 3rd edition, also indicate that although it can occur in young people, the frequency increases with age and tends to become more severe 5).
The incidence of HZO in children is low: 4.8 per 100,000 in those aged 0–10 years and 7.8 per 100,000 in those aged 11–20 years 2). The main risk factors are intrauterine exposure to varicella-zoster virus and varicella infection in infancy, and most reported cases were immunocompetent children 2).
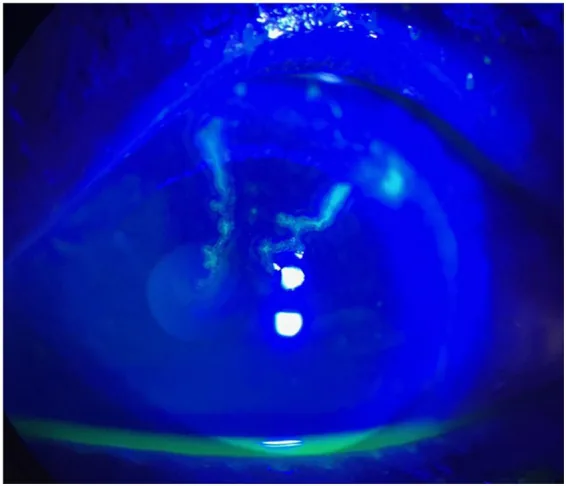
Tsai-Wei Lin, Wen-Chien Huang Initial diagnosis of herpes zoster ophthalmicus complicated by central retinal artery occlusion and subsequent varicella-zoster virus encephalitis: a case report 2026 Jan 14 Front Neurol.; 16:1751103 Figure 1. PMCID: PMC12847045. License: CC BY.
In fluorescein staining of the left cornea, a pseudodendritic corneal lesion suggestive of varicella-zoster virus keratitis is observed. This complements the clinical features of the cornea described in the section “Main Symptoms and Clinical Findings.”
Several days to one week before the appearance of the rash, prodromal symptoms such as sensory abnormalities and neuralgic pain in the first division of the trigeminal nerve appear. Fever, headache, and malaise often accompany. Subsequently, edematous erythema and small vesicles cluster in a dermatomal pattern on the unilateral eyelid, forehead, scalp, and nose, demarcated at the midline. The vesicles gradually progress to pustules, erosions, and crusting, healing with mild scarring. Ocular symptoms include eye pain, redness, tearing, photophobia, and blurred vision.
Approximately 50% of HZO patients develop ocular complications, and up to 25% of these become chronic or recur 1). Ocular complications often occur later than the peak of the rash, and even if no ocular findings are present at the initial examination, continued follow-up is necessary, even when referred from dermatology.
Hutchinson’s sign: Rash on the dorsum, tip, or ala of the nose indicates involvement of the nasociliary nerve, which branches from the first division of the trigeminal nerve (ophthalmic nerve). Since the nasociliary nerve also supplies the cornea and iris, the frequency of ocular complications is significantly higher in patients with this sign 5). The Infectious Keratitis Clinical Practice Guidelines also state that “when a rash is seen on the dorsum or tip of the nose, ocular complications are significantly more frequent” 5). However, the severity of the rash does not necessarily correlate with the incidence of ocular complications; if herpes zoster appears in the first division of the trigeminal nerve, an ophthalmological examination is necessary even if the rash is mild.
Corneal Complications
Pseudodendritic keratitis: Thin, small, and takes a caput Medusae-like shape with extensions from a single center. No terminal bulbs, and fluorescein staining is weak. It resolves 4–6 days after infection but may progress to stromal keratitis 5).
Multiple corneal infiltrates / nummular keratitis: Lesions similar to SEI of adenoviral conjunctivitis appear in the peripheral cornea. Small round opacities are scattered.
Deep stromal keratitis / disciform keratitis: Disciform stromal infiltration similar to HSV appears 1–3 months after infection. Chronic course may lead to corneal opacity, lipid deposition, neovascularization, and immune ring, sometimes requiring corneal transplantation 5)
Neurotrophic keratopathy: Persistent corneal ulcer due to decreased corneal sensation
Uvea / Intraocular pressure
Anterior uveitis: Granulomatous iritis with mutton-fat keratic precipitates
Sector iris atrophy: HSV causes localized round atrophy, whereas VZV is characterized by more extensive sectoral (segmental) iris atrophy
Paralytic mydriasis: In VZV iridocyclitis, the pupil may not recover even after uveitis subsides, leaving paralytic mydriasis
Secondary glaucoma: Mainly due to trabeculitis-induced intraocular pressure elevation, and may be complicated by pupillary block from posterior synechiae
Nervous system / Other
Postherpetic neuralgia (PHN): Chronic pain occurring in 36.6% of patients aged 60 years or older 1)
Cranial nerve palsy: Oculomotor nerve palsy is most common; trochlear and abducens nerve palsies also occur
Optic neuritis / retrobulbar neuritis: Rare, but in immunocompromised patients it develops on average 14.1 days after rash onset, with poor visual prognosis 4)
Acute retinal necrosis (ARN): Particularly high risk in immunocompromised patients, with danger of blindness
The frequency data above are compiled from multiple studies1). Herpes zoster conjunctivitis may present as catarrhal conjunctivitis with mucopurulent discharge, follicular formation, and preauricular lymphadenopathy. Small pustules similar to skin rash may appear on the conjunctiva, and episcleritis or pseudodendritic corneal lesions may also occur.
It is important to differentiate between HSV dendritic keratitis and VZV pseudodendritic keratitis. Pseudodendritic keratitis consists of elevated lesions on the corneal epithelial surface, without a central groove, with weak fluorescein staining, and no terminal bulbs5). HSV dendritic keratitis has terminal bulbs, a certain width, and marginal infiltration.
Months after the rash resolves, pale white, slightly elevated, linear, stellate, or pseudodendritic lesions may appear on the corneal epithelium, known as delayed herpes zoster pseudodendrite / mucous plaque keratitis. Previously thought to be an immune reaction, it is now considered to be caused by viral proliferation.
Varicella-zoster virus vasculopathy can cause cerebral infarction due to inflammation of cerebral arteries. In HZO patients, the hazard ratio for stroke is increased to 1.313). In VZV vasculopathy cases, 97% have abnormal CT/MRI findings, and detection of anti-VZV IgG antibody in cerebrospinal fluid has the highest diagnostic sensitivity at 93%3).
QWhat is Hutchinson's sign?
A
Hutchinson’s sign is the presence of herpes zoster rash on the tip, side, or root of the nose. Because the nasociliary nerve also innervates the cornea and iris, this sign is a strong predictor of ocular complications. The Japanese guidelines for infectious keratitis also state that ocular complications are significantly more frequent when rash is present on the nasal dorsum or tip. However, ocular complications can occur even when Hutchinson’s sign is negative, so if herpes zoster appears in the first division of the trigeminal nerve, an ophthalmology consultation is necessary.
Varicella-zoster virus (double-stranded DNA virus, alphaherpesvirus subfamily) latently infects the trigeminal ganglion and reactivates with aging or immunosuppression. Unlike HSV, VZV latently infects satellite cells of the ganglion, so upon reactivation, infection spreads to adjacent neurons, resulting in a wider lesion area than HSV. VZV is rapidly inactivated outside cells, so the rash is limited to the innervated area and is unilateral.
About 90% of herpes zoster cases occur in immunocompetent individuals 1). It is particularly common in older adults aged 50 and over, patients with diabetes, cancer patients, and those with reduced immunity due to long-term use of steroids or immunosuppressants. It also frequently occurs as an opportunistic infection in HIV infection, but can also occur in completely healthy people.
Meta-analyses have shown the strongest associations with immunosuppression (HIV/AIDS, hematologic malignancies, organ transplantation), family history, trauma, and aging 1). Use of disease-modifying drugs such as JAK inhibitors also increases risk 1). In HIV-positive individuals, the risk of herpes zoster increases 15-fold, and the frequency of HZO reaches 22.1% 1).
There are reports that the risk of herpes zoster increases by 14–15% after COVID-19 illness 1). On the other hand, large database studies have not found a significant increase in HZO risk after COVID-19 vaccination 1).
HZO is primarily a clinical diagnosis; in typical cases, confirmatory tests are not required. Unilateral vesicular rash and neuralgia along the dermatome of the first branch of the trigeminal nerve, along with associated ocular findings, strongly suggest HZO. A history of rash with ocular neuralgia is very useful for diagnosis, and even if no rash is present at the initial visit, a history of herpes zoster several months or more earlier may be elicited.
The third edition of the Japanese Infectious Keratitis Clinical Practice Guidelines recommends comprehensive assessment of the following findings for the diagnosis of herpes zoster keratitis 5):
Rash and neuralgia in the trigeminal nerve distribution area
Four-fold or greater rise in serum antibody titer (complement fixation reaction)
Detection of multinucleated giant cells or viral antigens from the rash
Proof of VZV-DNA by PCR from aqueous humor or corneal lesions
Corneal epithelial defect and decreased corneal sensation, along with inflammation in any intraocular structure, support the diagnosis. Uveitis associated with HZO often presents with elevated intraocular pressure.
Corneal sensation test: Decreased corneal sensation is frequently observed in HZO. Measure with a Cochet-Bonnet esthesiometer before instilling anesthetic drops.
PCR test: When the diagnosis is uncertain (e.g., zoster sine herpete without rash, recurrent anterior uveitis), VZV-DNA is detected in scrapings of skin or ocular lesions or in aqueous humor5). Unlike HSV, VZV is not thought to undergo spontaneous shedding, so even detection of DNA alone strongly suggests etiology. However, VZV-DNA may be detected in tears for months after herpes zoster ophthalmicus.
Serum antibody titer: A fourfold or greater rise in complement-fixing antibody titer suggests recent infection 5). Unlike HSV, an increase in serum antibody titer is useful for diagnosing VZV.
Viral antigen detection: Multinucleated giant cells on Giemsa staining of skin scrapings, and viral antigen detection by fluorescent antibody or enzyme antibody methods are also performed.
Zoster sine herpete: Herpes zoster that presents with neuralgia alone without rash. Aqueous humor PCR is useful for diagnosis.
Zosteriform herpes simplex: A condition in which HSV presents with extensive rash resembling herpes zoster, especially in patients with atopic dermatitis. It differs from herpes zoster in that it is not accompanied by neuralgia and the rash heals without scarring.
HSV dendritic keratitis: Differentiate from pseudodendritic keratitis by the presence of terminal bulbs and strong fluorescein staining.
Systemic antiviral therapy within 72 hours of onset is important for preventing ocular complications 1). In the antiviral-treated group, chronic ocular complications occurred in only 30%, significantly lower than the 50% in the untreated group 1). Antiviral therapy also significantly reduces the incidence of neurotrophic keratopathy within 6 months 1).
The Japanese Infectious Keratitis Clinical Practice Guidelines, 3rd edition, recommend that for herpes zoster, systemic antiviral therapy (acyclovir, valacyclovir hydrochloride, famciclovir, amenamevir) be initiated as early as possible, primarily by dermatologists. For severe cases, intravenous acyclovir is recommended; for moderate cases, oral valacyclovir hydrochloride, famciclovir, or amenamevir is recommended 5).
Drug
Dosage
Route of administration
Acyclovir
800 mg 5 times daily
Oral
Valacyclovir hydrochloride (Valtrex®)
1,000 mg 3 times daily (total 3,000 mg/day)
Oral
Famciclovir (Famvir®)
500 mg 3 times daily
Oral
Amenamevir (Amenalief®)
400 mg once daily
Oral
Acyclovir
5–10 mg/kg every 8 hours
Intravenous infusion
The treatment duration is 7–10 days1). Valacyclovir and famciclovir require fewer doses, offering better adherence, and both show efficacy equivalent to acyclovir1). Amenamevir 400 mg once daily (helicase–primase inhibitor) is also available as an option. For severe cases or immunocompromised patients, acyclovir 5–10 mg/kg intravenously every 8 hours is used.
For pseudodendritic keratitis, acyclovir ophthalmic ointment (Zovirax® 3%) is used. In Japan, the use of ophthalmic ointment for keratitis is not covered by insurance, but it is recommended as standard treatment in the 3rd edition of the Infectious Keratitis Guidelines5). Administration is discontinued once epithelial lesions resolve. Unlike HSV, concomitant use of steroid eye drops from the pseudodendritic keratitis stage is considered safe.
When stromal keratitis develops, acyclovir ophthalmic ointment and steroid eye drops are used together. Compared to HSV-induced stromal herpes keratitis, higher concentrations of steroid eye drops are often required5). Abrupt discontinuation of steroids after a short period can cause recurrence, so they must be tapered gradually over a relatively long period. The frequency of ACV ophthalmic ointment can be low, but it must always be used concomitantly. It is warned that inadequate treatment with steroid eye drops may lead to serious sequelae such as corneal scarring, posterior synechiae, and secondary glaucoma5).
Prescription example (combination therapy for stromal keratitis):
Sanbetazone ophthalmic/otologic solution (0.1%) 5 times daily, eye drops
Zovirax ophthalmic ointment (3%) 5 times daily, instillation
For anterior uveitis, 1% prednisolone acetate eye drops and mydriatics (atropine or tropicamide) are used. For elevated intraocular pressure due to trabeculitis, aqueous humor suppressants such as beta-blockers, carbonic anhydrase inhibitors, and alpha-2 agonists are administered. Prostaglandin-related drugs are not first-line because they may worsen inflammation.
PHN is chronic pain that occurs in 36.6% of HZO patients aged 60 years or older1). Amitriptyline 25 mg at bedtime reduces the incidence of PHN1). Pregabalin 150 mg/day in divided doses is also effective for acute pain relief1). Gabapentin, tricyclic antidepressants, and lidocaine patches are also options.
In herpes zoster keratitis, unlike HSV epithelial keratitis, steroid eye drops can be used in combination from the stage of pseudodendritic keratitis. However, be sure to use antiviral drugs concurrently. For stromal keratitis and uveitis, aggressive steroid administration is necessary, but gradual tapering over a long period is important. The Japanese Infectious Keratitis Guidelines, 3rd edition, also warn that higher concentrations of steroids are often required than for HSV, and inadequate treatment can lead to severe sequelae such as corneal scarring, posterior synechiae, and secondary glaucoma.
After primary infection (chickenpox), varicella-zoster virus establishes latent infection in the satellite cells of the dorsal root ganglia and trigeminal ganglia. Unlike HSV, which latently infects neurons themselves, VZV latently infects satellite cells, so upon reactivation, infection spreads to adjacent neurons, forming more extensive lesions.
Cell-mediated immunity (especially VZV-specific T-cell responses) plays a central role in suppressing the virus. When VZV-specific cell-mediated immunity declines due to aging, immunosuppressive drugs, HIV infection, malignancy, psychological stress, etc., the virus reactivates.
Reactivated VZV travels anterogradely along the axons of the first division of the trigeminal nerve to reach the skin, cornea, and conjunctiva. In affected tissues, local immune responses cause vesicle formation and intraocular inflammation. Perineuritis causes severe pain along the innervation area. Since VZV is rapidly inactivated extracellularly, lateral spread on the skin surface is limited, and the rash is confined to the innervation area.
VZV spreads transaxonally from nerve axons to surrounding blood vessels and infects the arterial wall 3). This leads to vascular remodeling, thrombus formation, arterial dissection, and aneurysm 3). VZV vasculopathy presents with a variety of clinical manifestations including cerebral infarction, cerebral hemorrhage, and giant cell arteritis-like features. In immunocompetent individuals, skin rash and detection of anti-VZV antibodies are common, while in immunocompromised individuals, VZV-DNA and pleocytosis in cerebrospinal fluid are more frequent 3). A report that the hazard ratio for stroke in HZO patients increases to 1.31 reflects this vascular mechanism 3).
Retrobulbar optic neuritis is a rare complication of HZO, reported especially in immunocompromised individuals 4). It develops on average 14.1 days after the onset of rash, and visual prognosis is often poor 4).
Unlike HSV, VZV is rapidly inactivated outside cells, so its spread on the skin surface is limited. Recurrence usually occurs only once in a lifetime (whereas HSV recurs frequently), but the lesion area is extensive, and complications are diverse and often severe. On the other hand, recurrence of keratitis is rare compared to HSV keratitis, and the relatively active use of steroids is another important difference between the two.
Two types of herpes zoster vaccines are approved. The recombinant subunit adjuvant vaccine (RZV: Shingrix) prevents herpes zoster by 97.2% in individuals aged 50 and older, and by 91.3% in those aged 70 and older 1). Its efficacy against HZO is reported as 88% in a meta-analysis 1). In a real-world study, the incidence of HZO was 11.9 per 100,000 person-years in the vaccinated group and 72.1 per 100,000 person-years in the unvaccinated group 1). In Japan, Shingrix was approved in 2020 for individuals aged 50 and older and for immunocompromised patients aged 18 and older.
The live vaccine (ZVL: Zostavax) has a 10-year HZO prevention efficacy of only 37% and cannot be used in immunocompromised individuals 1). Currently, RZV is recommended.
Vaccination of patients with a history of HZO has been reported to possibly slightly increase the risk of recurrence or exacerbation within 56 days after vaccination 1). The American Academy of Ophthalmology (AAO) recommends that patients with a history of HZO undergo ophthalmic examination several weeks before and after vaccination 1).
A large-scale randomized trial (NCT03134196) is underway to evaluate whether one year of valacyclovir 1,000 mg/day reduces ocular complications (recurrence of keratitis and uveitis) in patients with HZO 1). It is expected to clarify the efficacy of long-term low-dose antiviral therapy for chronic and recurrent HZO.
Systematic epidemiological data on pediatric HZO are lacking, and establishing diagnostic and treatment protocols remains a future challenge 2). Further research is needed on long-term prognosis and the association with COVID-19 2).
QCan the herpes zoster vaccine prevent HZO?
A
Yes, the recombinant subunit vaccine (Shingrix) has been reported to be approximately 88% effective in preventing HZO. Vaccination is recommended for adults aged 50 years and older, and for immunocompromised adults aged 18 years and older, and it is approved in Japan. Vaccination is also recommended for those who have previously had HZO, but it is advised to receive the vaccine after the eye disease is well controlled and to have an ophthalmology consultation before and after vaccination according to the American Academy of Ophthalmology guidelines.
Litt J, Cunningham AL, Arnalich-Montiel F, Parikh R. Herpes Zoster Ophthalmicus: Presentation, Complications, Treatment, and Prevention. Infectious diseases and therapy. 2024;13(7):1439-1459. doi:10.1007/s40121-024-00990-7. PMID:38834857; PMCID:PMC11219696.
Hakim FE, Riaz K, Farooq A. Pediatric herpes zoster ophthalmicus: a systematic review. Graefes Arch Clin Exp Ophthalmol. 2023. doi:10.1007/s00417-023-06033-0.
Philip AM, George LJ, N A, Nayar J. Varicella Zoster Virus Vasculopathy: An Under-Recognized Entity. Cureus. 2024;16(5):e61419. doi:10.7759/cureus.61419. PMID:38947631; PMCID:PMC11214726.
Phang DSK, Ettikan JV, Abd Aziz H, Vendargon FM, Sonny Teo KS. A Rare Complication of Herpes Zoster Ophthalmicus (HZO). Cureus. 2023;15(3):e35693. doi:10.7759/cureus.35693. PMID:37012964; PMCID:PMC10066721.