CRAO
Central Retinal Artery Occlusion (CRAO): Occlusion of the central retinal artery. This is the most severe type, and vision often decreases to hand motion or light perception.
Incidence: 1 per 100,000 per year, 1 per 10,000 outpatients8).

Retinal artery occlusion is a disease that causes severe visual impairment due to retinal ischemia and necrosis from occlusion of the retinal artery. Irreversible retinal changes begin approximately 100 minutes after arterial occlusion, so visual outcomes are often poor even with treatment. It is classified into the following three types based on the occlusion site.
CRAO
Central Retinal Artery Occlusion (CRAO): Occlusion of the central retinal artery. This is the most severe type, and vision often decreases to hand motion or light perception.
Incidence: 1 per 100,000 per year, 1 per 10,000 outpatients8).
BRAO
Branch Retinal Artery Occlusion: occlusion of a branch. Visual prognosis varies greatly depending on the occlusion site.
Features: 80% eventually maintain corrected visual acuity of 0.5 or better. Visual acuity does not decrease if the macula is not affected.
Cilioretinal Artery Occlusion
Cilioretinal Artery Occlusion: occlusion of the cilioretinal artery. It is a branch of the short posterior ciliary artery and is present in about 32% of all eyes. It supplies the retina near the papillomacular bundle.
Features: It may occur in combination with CRAO or alone.
CRAO is further classified into non-arteritic and arteritic types. Non-arteritic CRAO accounts for over 90% of all cases and has the following three subtypes:
Arteritic CRAO is secondary to giant cell arteritis (GCA) and accounts for about 4% of CRAO patients. It has the worst prognosis among the four types, and vision loss is almost irreversible. It is more likely to occur in patients aged 70 years or older and is often accompanied by GCA-related symptoms such as headache, scalp tenderness, jaw claudication, malaise, and weight loss. The most important step in all CRAO patients aged 50 years or older is to rule out arteritic CRAO, by rapid measurement of ESR and CRP and, if necessary, temporal artery biopsy. If GCA is strongly suspected, systemic steroid therapy should be started immediately without waiting for a definitive diagnosis 8). Delay in treatment increases the risk of contralateral eye blindness.
The incidence of CRAO is estimated at about 1 per 100,000 population per year, or 1 per 10,000 outpatients. The average age of onset is in the early 60s, and the incidence increases with age 8). It is more common in men and usually occurs in one eye, but 1-2% occur in both eyes. Bilateral involvement should raise suspicion of giant cell arteritis 8). The incidence in Japan is lower than in Western countries, making it a relatively rare disease, but it is a highly urgent condition where very early response determines visual prognosis.
The retina is a tissue that differentiates from the brain during embryonic development and is considered part of the central nervous system. Its relationship with stroke is close; in 2013, the AHA/ASA (American Heart Association/American Stroke Association) revised the definition of stroke to explicitly include retinal ischemia as a type of CNS (central nervous system) infarction 8). 15–20% of CRAO patients develop a stroke within 30 days, and as an “eye stroke,” emergency systemic evaluation at a stroke center is recommended 8).
CRAO shares the same risk factors as stroke (arteriosclerosis, atrial fibrillation, embolism, etc.) and has a high risk of stroke within 30 days after onset, at 15–20% 8). The AHA/ASA defines retinal ischemia as CNS infarction, and after CRAO onset, emergency systemic evaluation in collaboration with neurology and cardiology is essential.
Sudden onset of painless severe vision loss is the most characteristic feature.
In CRAO, some patients experience repeated transient vision loss before onset. This is called amaurosis fugax and is an important warning sign as a precursor symptom of stroke (TIA). Vision loss lasts a few minutes and then recovers spontaneously, but it often precedes the main attack.
A case of COVID-19-related CRAO in a 6-year-old girl has been reported, presenting with sudden bilateral vision loss, indicating that (though rare) onset can occur in children 1).
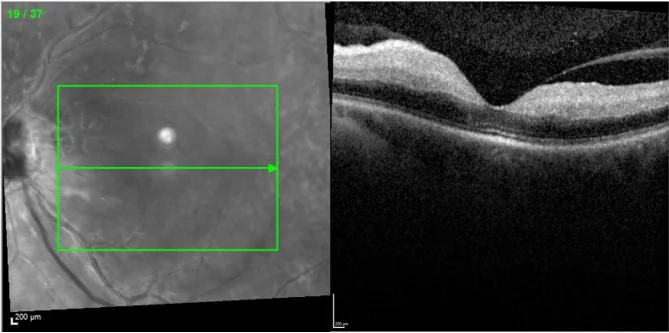
Characteristic findings appear in the acute phase but change over time. In the hyperacute phase within 2 hours of onset, fundus findings may be normal or show only slight macular opacity.
In a 6-year-old girl with COVID-19-associated CRAO, thinning of the RNFL (retinal nerve fiber layer) persisted even 5 months after onset1). In the chronic phase, OCT shows retinal thinning, and retrograde atrophy occurs not only in the inner layers but also in the outer layers, making the layered structure difficult to identify.
In CRAO, the entire inner retinal layer becomes milky white due to ischemic intracellular edema. However, the fovea, which consists only of the outer retinal layer and receives nutrition from the choriocapillaris, does not become opaque. The mechanism of cherry-red spot is that the red color of the choroid becomes visible against the surrounding white opacity. For detailed vascular anatomy, refer to the “Pathophysiology” section.
The main cause of CRAO is embolism, accounting for approximately 95% of all cases8). The distribution of causes varies by age and underlying disease.
| Age Group | Main Cause | Conditions to Investigate |
|---|---|---|
| 50 years and older | Arteriosclerotic embolism/thrombus | Carotid artery stenosis, atrial fibrillation, hypertension |
| Under 50 years | Coagulation abnormality, PFO, vasculitis | Paradoxical embolism, autoimmune disease |
Modifiable risk factors include smoking, hypertension, high BMI, dyslipidemia, diabetes, coagulation disorders, and heart disease (including atrial fibrillation) 8). Approximately 60% of CRAO patients have at least one undiagnosed vascular risk factor, with dyslipidemia being the most common. Low HDL cholesterol has also been reported as an independent risk factor 8).
Systemic risk factors are listed below.
CRAO can often be diagnosed by fundus findings, but systemic evaluation to search for the cause is essential. Management of CRAO is divided into three stages: first, restoration of blood flow in the acute phase; second, prevention of secondary complications in the subacute phase; and third, systemic control and prevention of future vascular ischemic events.
The main findings obtained from each examination are shown below.
| Examination Method | Main Findings |
|---|---|
| OCT | Acute phase: inner layer hyperreflectivity and thickening → Chronic phase: inner layer thinning |
| FA | Delayed filling, arm-to-retina circulation time ≥30 seconds |
| ERG | Normal a-wave, reduced b-wave (negative-type ERG) |
Acute CRAO requires immediate referral to a stroke center for urgent systemic evaluation 8). The stroke risk in symptomatic RAO patients is highest from 2 weeks before to 1 month after onset 8).
Exclusion of arteritic CRAO due to giant cell arteritis (GCA) is most important. GCA-related CRAO accounts for about 4% of all CRAO cases and has the worst prognosis. If GCA is suspected, start systemic steroids immediately without waiting for definitive diagnosis (temporal artery biopsy) 8). Untreated, there is a risk of contralateral eye blindness.
CRAO is an ophthalmic emergency, and prompt management in the hyperacute phase is essential to improve visual prognosis. Treatment immediately after onset is preferable, and active treatment should be considered for cases within one day of onset.
Severe retinal damage begins approximately 100 minutes after arterial occlusion. Treatment is most favorable immediately after onset, and within about 4 hours is considered the target for acute-phase treatment 6). The longer the time from onset to consultation, the worse the prognosis, but active treatment should be considered for cases within one day of onset. For BRAO with early visual impairment, the same treatment strategy as for CRAO is followed.
Zokri MF et al. (2024) emphasized in a case series of acute RAO that time to treatment initiation is the most important factor determining visual outcome 6). Many cases lose the opportunity for therapeutic intervention due to delayed consultation.
The following treatments are used depending on symptoms.
Vasodilators
Amyl nitrite: Crush a 0.25 mL vial, absorb into a covering, and inhale through the nostrils (caution for blood pressure drop; off-label use).
Isosorbide dinitrate sublingual: Promotes vasodilation.
Carbogen inhalation: Inhalation of a 95% oxygen + 5% CO₂ gas mixture. Promotes blood flow but carries a risk of systemic hypotension.
Pentoxifylline: A peripheral circulation-improving drug. Enhances retinal blood flow by improving red blood cell deformability.
Pharmacotherapy
Diamox injection: 500 mg intravenously once daily (off-label use). As a carbonic anhydrase inhibitor, it lowers intraocular pressure and promotes retinal artery dilation.
Urokinase: Initial daily dose of 60,000 to 240,000 units, then gradually reduced over about 7 days. Caution for cerebral hemorrhage and systemic bleeding.
Obalmon tablets: 5 μg × 6 tablets, divided into three doses after meals. As a prostaglandin E₁ derivative, it aims to improve peripheral blood flow.
Procedures and Systemic Management
Ocular massage: Lowers intraocular pressure and moves the embolus peripherally. It is a procedure that can be performed immediately.
Anterior chamber paracentesis: Aspirates aqueous humor to rapidly lower intraocular pressure, relatively increasing arterial perfusion pressure.
Stellate ganglion block: May be performed to improve ocular blood flow.
However, conservative treatments (ocular massage, anterior chamber paracentesis, carbogen inhalation) have not been proven to have significant efficacy8). These procedures are theoretically meaningful only in the very early stage after onset, but there is no solid evidence that they improve prognosis compared to the natural course.
Acute CRAO should be urgently referred to a stroke center, and evaluation and treatment should be performed according to the “Eye stroke protocol”8). At stroke centers, CRAO is treated as an emergency equivalent to cerebral infarction, and systems are being established to centrally manage tPA administration eligibility assessment, systemic vascular evaluation, and secondary prevention.
Use the following as appropriate depending on symptoms.
A case has been reported in which visual acuity dramatically improved from 20/2000 to 20/33.3 after intra-arterial administration of 300,000 units of urokinase4).
The spontaneous visual recovery rate in CRAO is approximately 18%, but early thrombolytic therapy is reported to increase it to around 40%. However, the EAGLE trial (RCT) found no significant difference in visual improvement between intra-arterial (IA) tPA and conservative treatment, and safety concerns regarding intracranial hemorrhage (ICH) were noted7). Currently, evidence for intra-arterial and intravenous fibrinolytic therapy for CRAO is considered insufficient8).
If arteritic CRAO is suspected, systemic steroid administration should be initiated immediately without waiting for a definitive diagnosis. Delay in treatment carries a risk of contralateral eye blindness8).
Some small retrospective studies suggest a mild effect, but a Cochrane review concluded that the evidence is uncertain8).
In the subacute phase after CRAO, chronic retinal ischemia due to reperfusion failure may cause ocular neovascularization. The prevalence of neovascularization is reported to be 2.5–31.6%, and the mean time to observation of neovascularization is 8.5 weeks. Iris neovascularization has been reported in 18% of CRAO cases, and regular ophthalmologic examinations are important for about 4 months after onset. When iris or retinal neovascularization occurs, panretinal photocoagulation (PRP) is indicated 8).
Patients with CRAO have an increased risk of systemic ischemic events, and collaboration with internists, stroke specialists, and cardiologists is important for long-term complication prevention. Approximately 60% of CRAO patients have at least one undiagnosed vascular risk factor, and systemic evaluation triggered by CRAO onset is the first step in secondary prevention.
The visual outcome of CRAO is poor, often resulting in counting fingers or worse. Without treatment, the chance of visual recovery is only about 18%. At initial presentation, 61% have visual acuity of 20/400 or worse 8). Retinal opacity resolves 4–6 weeks after onset, and the retina returns to a normal color, but visual function does not recover unless early treatment is effective. Neovascular glaucoma may develop 4–10 weeks after onset.
On the other hand, in CRAO with preserved cilioretinal artery, the perfusion area of the cilioretinal artery is preserved, so central vision may be maintained. In transient CRAO, the occlusion resolves spontaneously, so the visual prognosis is best. In BRAO, 80% maintain a corrected visual acuity of 0.5 or better, but if the branch to the macula is occluded, the visual prognosis is poor.
After CRAO, attention must also be paid to complications associated with reperfusion failure. Iris neovascularization occurs in about 18% of CRAO cases and may progress to neovascular glaucoma 4–10 weeks after onset. If neovascularization occurs, panretinal photocoagulation (PRP) should be performed promptly 8).
Irreversible retinal damage begins approximately 100 minutes after occlusion. Active treatment is recommended within 1 day of onset, and earlier treatment leads to better prognosis. Intravenous tPA is indicated within 4.5 hours of onset 8). In any case, as an “ocular stroke,” emergency consultation at a stroke center is essential.
The central retinal artery, a branch of the ophthalmic artery (first branch of the internal carotid artery), enters the retina at the optic disc and supplies oxygen and nutrients to the inner two-thirds of the retina (from the nerve fiber layer to the inner nuclear layer). Photoreceptors in the outer retina receive nutrition from the choroidal vessels, so the outer layer is relatively preserved in CRAO.
The cilioretinal artery, a branch of the short posterior ciliary arteries, is present in about 32% of all eyes and supplies the area near the papillomacular bundle. Since the cilioretinal artery branches off before the ophthalmic artery becomes the central retinal artery, it is not affected by CRAO. Therefore, if this artery is preserved, central foveal vision may be maintained.
The mechanism of cherry-red spot formation is as follows. In CRAO, the inner retinal layers supplied by the retinal artery undergo acute ischemia, leading to cellular swelling (intracellular edema) and ischemic necrosis, resulting in a milky-white opacity centered on the posterior pole. This opacity differs in mechanism from ordinary retinal edema (extracellular edema). In ordinary retinal edema, extracellular fluid accumulation causes low reflectivity on OCT, whereas in CRAO, ischemic intracellular edema (cellular swelling) causes high reflectivity in the inner retinal layers. OCT shows the inner retinal layers as hyperreflective and thickened.
The fovea is composed only of the outer retinal layers and is nourished by the choroid, so it does not become opaque. In the fovea, the inner layers (ganglion cell layer, inner plexiform layer, inner nuclear layer) are almost absent, and only the outer layer (photoreceptor layer) exists. Therefore, the normal red color (color of the choroidal capillaries) appears to stand out within the surrounding milky-white opacity. This is the cause of the cherry-red spot.
In ophthalmic artery occlusion (OAO), the main trunk of the ophthalmic artery is occluded, impairing both retinal and choroidal circulation. Due to choroidal ischemia, a cherry-red spot does not appear 8).
The most common cause of CRAO is thromboembolism, with occlusion occurring at the narrowest part of the central retinal artery lumen (where it penetrates the dural sheath of the optic nerve). Emboli originate from plaques in the carotid artery or heart.
Retinal ganglion cells are extremely vulnerable to ischemia, with functional impairment beginning within minutes of blood flow cessation. Irreversible damage is thought to occur from approximately 100 to 105 minutes 8). This is the basis for the urgency of this disease.
Tissue changes according to the time course of ischemia are as follows.
In chronic hypertension, it has been reported that the time until irreversible changes occur may be extended up to 240 minutes6).
In a 6-year-old girl with COVID-19-associated CRAO, low molecular weight heparin (LMWH) 100 mg/kg and methylprednisolone 30 mg/kg were used, and RNFL thinning persisted at the 5-month follow-up1).
Sano et al. (2025) retrospectively examined the effect of early PGE₁ administration in CRAO patients within 24 hours of onset at Tokushima Red Cross Hospital9). In the PGE₁ group (n=4), alprostadil alfadex 40 μg was dissolved in 250 mL saline and infused intravenously at 125 mL/h twice daily (80 μg/day) for 5 days, followed by oral limaprost alfadex 10 μg three times daily (30 μg/day) for at least 1 month. Compared to the conventional treatment group (n=6), the best-corrected visual acuity (BCVA) at 1 month was significantly better in the PGE₁ group. In the PGE₁ group, baseline maximum retinal thickness (MRT) showed a negative correlation with BCVA at 1 month. No adverse events were observed in either group9).
PGE₁ is thought to have neuroprotective effects through vasodilation as well as reduction of oxidative stress and inflammation. Although the sample size is small and a prospective RCT is needed, these findings are noteworthy given the lack of proven efficacy of existing treatments.
The “Eye stroke protocol,” which treats CRAO as an equivalent of cerebral stroke and involves stroke centers collaborating with ophthalmology for acute evaluation and treatment, is becoming more widespread8). This protocol is expected to improve tPA administration rates and enable early detection and secondary prevention of stroke.
Selective intra-ophthalmic artery infusion of urokinase/tPA is performed at some institutions, but evidence from randomized controlled trials is limited. The EAGLE trial showed no significant difference in visual improvement between IA tPA and conservative treatment, and safety concerns regarding ICH (intracranial hemorrhage) were raised7).
In a case of CRAO, intra-arterial administration of 300,000 units of urokinase resulted in dramatic visual improvement from 20/2000 to 20/33.34). However, IA tPA carries risks of vascular dissection and intracranial hemorrhage7), and accumulation of cases and establishment of indication criteria remain future challenges.
This is a non-invasive treatment that mimics intra-aortic balloon pumping by compressing the lower limbs during diastole to increase ocular perfusion pressure.
A case has been reported of a 40-year-old woman with RAO after HA injection and concomitant PFO who underwent ECP, with visual acuity improving from CF 30 cm to 20/1332). However, evidence for ECP in RAO is limited to case reports and small studies.
When PFO is identified as the cause in young patients with CRAO, percutaneous PFO closure to prevent paradoxical embolism may be considered.
Wieder MS et al. (2021) concluded in a literature review of 7 cases of CRAO with PFO that appropriate anticoagulation/antiplatelet therapy or PFO closure is recommended3). However, no randomized trial of PFO closure specifically for CRAO has been conducted.
PGE₁ Therapy
Report from Japan: In CRAO, PGE₁ (alprostadil 80 μg/day IV for 5 days followed by limaprost 30 μg/day orally) significantly improved BCVA at 1 month9).
Mechanism: Vasodilation + neuroprotection (reduction of oxidative stress and inflammation). No adverse events.
Current Status of tPA
EAGLE trial: IA tPA showed no visual improvement benefit compared to conservative treatment and carried a risk of ICH7).
IV tPA: May improve outcomes within 4.5 hours of onset (meta-analysis), but RCT evidence is insufficient8).