Central retinal vein occlusion (CRVO) is a disease in which the central retinal vein is occluded at the level of the lamina cribrosa within the optic nerve. The occlusion causes increased venous pressure, leading to blood stasis, ischemia, and exudation within the retina, resulting in flame-shaped hemorrhages, optic disc edema, and macular edema in all four quadrants.
Retinal vein occlusion overall is the second most common retinal vascular disease after diabetic retinopathy9, 10). As of 2015, the global prevalence was approximately 0.77%, with an estimated 28 million affected individuals aged 30–89 years 10). The prevalence of CRVO in people aged 40 years and older is reported to be about 0.2%, which is one-sixth to one-seventh the frequency of branch retinal vein occlusion (BRVO) 10). It most commonly occurs in the 60s and 70s and is relatively rare under age 40 9, 10).
CRVO is broadly classified into perfused (non-ischemic) type and non-perfused (ischemic) type. Non-ischemic type accounts for approximately 75–80% of all CRVO. There is also hemi-central retinal vein occlusion (hemi-CRVO), which affects only the superior or inferior two quadrants, and its clinical course is similar to CRVO 9, 10). Hemi-CRVO occurs when one of two independent hemi-central veins is occluded at the lamina cribrosa level, and unlike BRVO, an arteriovenous crossing is often not visible. About 90% affect the superior or inferior hemifield 10). Note that, like CRVO, there is a high risk of neovascular glaucoma10).
Important complications of CRVO are macular edema and neovascularization. Macular edema occurs in both non-ischemic and ischemic types and is the main cause of visual loss. Neovascularization (iris neovascularization, retinal neovascularization) occurs mainly in the ischemic type; about 25% of CRVO cases develop iris neovascularization, which can lead to blindness due to neovascular glaucoma10). It has been reported that patients with CRVO have an increased risk of cardiovascular events and all-cause mortality compared to the general population 10), and collaboration with internal medicine is important from the perspective of systemic management.
QWhat is the difference between central retinal vein occlusion and branch retinal vein occlusion?
A
CRVO is an occlusion of the main trunk vein within the optic nerve, causing hemorrhage throughout the entire retina (4 quadrants). BRVO is an occlusion of a branch vein at an arteriovenous crossing, and the damage is limited to 1-2 quadrants. BRVO is 6-7 times more common than CRVO 10). Compared to BRVO, CRVO has a higher risk of neovascular glaucoma and tends to require more frequent anti-VEGF treatments.
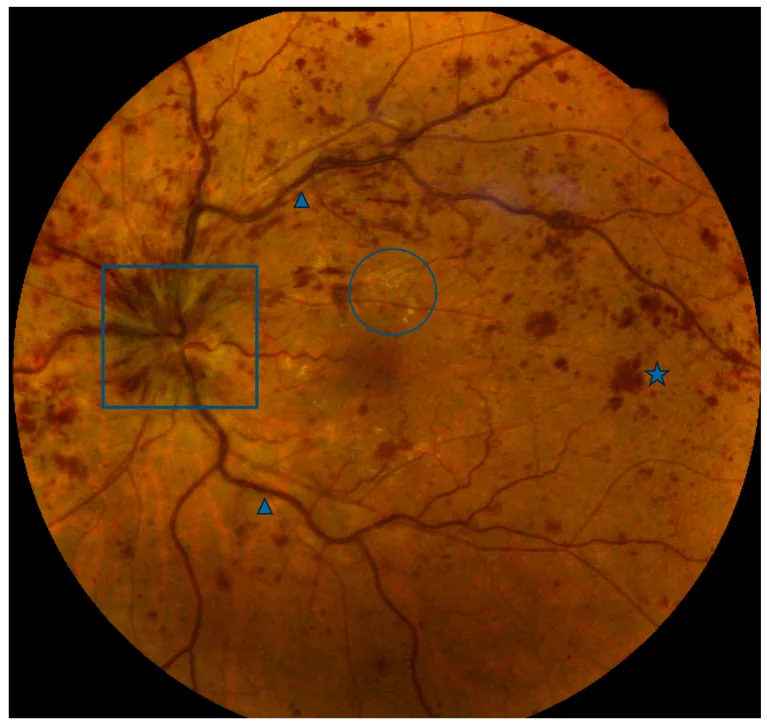
Colcombe J, et al. Retinal Findings and Cardiovascular Risk: Prognostic Conditions, Novel Biomarkers, and Emerging Image Analysis Techniques. J Pers Med. 2023. Figure 1. PMCID: PMC10672409. License: CC BY.
Multiple intraretinal hemorrhages throughout the fundus, along with dilation and tortuosity of the veins. Swelling of the optic disc and white spots around the macula are also seen. This image shows representative clinical findings of central retinal vein occlusion.
Symptoms of CRVO vary depending on the type of occlusion.
Non-ischemic type: May be discovered incidentally without subjective symptoms, but many cases present with visual loss due to macular edema. Acute onset may be limited to relatively mild blurred vision.
Ischemic type: Presents with sudden and severe visual impairment, often with profound visual loss of less than 20/200. Vitreous hemorrhage can cause rapid vision loss. Neovascular glaucoma may cause eye pain and headache.
Both types are characteristically painless.
Clinical findings (findings confirmed by physician examination)
Flame-shaped hemorrhages in all four quadrants: Unlike the sectoral distribution of BRVO, the spread to all quadrants is important for differentiation.
Dilation and tortuosity of retinal veins: Reflects increased venous pressure due to occlusion.
Papilledema: Often accompanied by edema around the optic disc.
Macular edema: The main cause of vision loss; quantitative assessment by OCT is essential.
Soft exudates (cotton-wool spots): Findings reflecting ischemia, prominently seen in the ischemic type.
Hard exudates: May be observed around the macula in long-standing cases.
The diagnosis itself is not difficult based on characteristic retinal hemorrhages, but detailed examinations beyond funduscopy are important for classification into non-ischemic and ischemic types, treatment indications, and prognosis prediction. Over time, acute hemorrhages are absorbed and soft exudates also resolve. In the long term, collateral circulation may develop around the optic disc and between retinal veins. Macular edema may resolve spontaneously, but if it persists, it leads to retinal pigment epithelium atrophy and worsens visual prognosis.
The key points for differentiating non-ischemic and ischemic types are shown in the table below. It has been reported that about one-third of non-ischemic cases convert to ischemic type during the course, with conversion occurring in 15% within 4 months and 34% within 3 years10).
In CRVO, OCTB-scan may show a band-like hyperreflectivity in the inner nuclear layer of the parafovea, called PAMM (paracentral acute middle maculopathy). It is thought to be caused by circulatory disturbance of peripheral arterioles supplying the deep retinal capillary plexus due to venous perfusion impairment. Hyperreflectivity is not prominent on en face images of the superficial retina, but is clearly visualized on en face images of the deep retina, corresponding to whitened retina. PAMM reflects ischemia of the intermediate capillary plexus and is noted as an auxiliary indicator for assessing the degree of retinal ischemia in CRVO.
Matsuo T et al. (2025) reported a case of bilateral CRVO in a 71-year-old man 1). The right eye progressed to neovascular glaucoma with intraocular pressure of 35 mmHg 4 months after onset, eventually losing light perception. The left eye maintained vision with anti-VEGF therapy and conservative treatment. Right heart dysfunction after cardiac surgery was considered a trigger for bilateral onset.
QHow often do I need to visit the hospital after being diagnosed with central retinal vein occlusion?
A
Non-ischemic type should be re-evaluated 4–6 weeks after onset. Ischemic type has a high risk of neovascular glaucoma, requiring monthly visits and gonioscopy for 6 months 9). Since about one-third of non-ischemic type convert to ischemic type, gonioscopy should always be performed. During anti-VEGF therapy, monthly OCT is recommended to evaluate macular edema.
The pathophysiology of CRVO is explained by Virchow’s triad (vascular injury, blood stasis, hypercoagulability). Posterior to the lamina cribrosa, the central retinal artery and central retinal vein share a common adventitia. When the arterial wall thickens and hardens due to arteriosclerotic changes, the adjacent vein is compressed, leading to endothelial damage, thrombus formation, and occlusion.
Major risk factors are shown in the table below.
Risk factor
Frequency/Association
Aging
Most important: over 90% are aged 55 or older
Hypertension
Up to 73% of those aged 50 or older have comorbidity 9, 10)
Hyperlipidemia
Major risk factor 7)
Diabetes mellitus
Independent risk factor 9, 10)
Glaucoma / high intraocular pressure
Independent risk factor 9, 10)
Meta-analysis indicates that 48% of RVO is attributable to hypertension, 20% to hyperlipidemia, and 5% to diabetes mellitus 10).
Other important risk factors are listed below.
Low HDL cholesterol: Low HDL-C has been reported as an independent risk factor for RVO, and it is important to note that it is often overlooked in routine lipid screening 10).
Systemic autoimmune diseases: In patients with SLE, the incidence of CRVO is reported to be 3.5 times that of controls 9, 10).
Cardiovascular risk: Patients with RVO have an increased risk of cardiovascular events and all-cause mortality. Collaboration with internal medicine is important 9, 10).
PDE5 inhibitors (e.g., sildenafil): 82 cases of RVO have been reported to the FDA, and the mechanism is thought to be retinal venous engorgement induced under systemic hypotension 2).
COVID-19 infection: The mechanism is thought to be vascular endothelial damage and hypercoagulability due to cytokine storm 3, 4).
COVID-19 vaccine: A VITT (vaccine-induced thrombotic thrombocytopenia) mechanism has been proposed, and the incidence of thrombosis after ChAdOx1 (AstraZeneca) vaccination is reported to be 1.13 per 100,000 doses 5, 6).
MTHFR gene mutation: Hypercoagulability due to hyperhomocysteinemia 3, 4).
Right heart dysfunction: Increased venous pressure due to impaired venous drainage can trigger bilateral CRVO 1).
Sleep apnea syndrome and carotid occlusive disease: Reported as risk factors for CRVO 10).
Contralateral eye risk: If CRVO occurs in one eye, the risk of developing CRVO in the fellow eye is 1% per year 10).
Depression: There are reports that the risk of RVO is increased in patients with depression 10).
For onset under age 50, systemic evaluation is strongly recommended. It has been reported that 58% of cases have non-traditional risk factors (e.g., coagulation abnormalities, autoimmune diseases) identified 9, 10). Even in patients over 50, it is recommended to check the management status of hypertension, diabetes, and dyslipidemia, and to share information with the primary care physician.
QCan young people develop central retinal vein occlusion?
A
Onset under age 40 is rare but possible. Coagulation abnormalities, MTHFR gene mutations, COVID-19 infection, post-vaccine VITT, and PDE5 inhibitors can be causes 2, 3, 4, 5, 6). In patients under 50, coagulation screening (protein C/S, antithrombin III, etc.) and autoantibody tests (antiphospholipid antibodies, antinuclear antibodies, etc.) are recommended 9, 10). In young CRVO, differentiation from papillophlebitis is also important, as the latter may require systemic steroid treatment.
Diagnosis is made by combining medical history, visual acuity, and fundus findings. The characteristic fundus findings of flame-shaped hemorrhages in all four quadrants and venous dilation and tortuosity make diagnosis straightforward, but the following tests are essential for classifying ischemic/non-ischemic type and determining treatment indications.
Medical history: Course of vision loss, medications (anticoagulants, PDE5 inhibitors), past medical history (hypertension, diabetes, blood disorders, sleep apnea) 9, 10).
Visual acuity test: In ischemic type, visual acuity is often less than 20/200 at initial visit.
RAPD test: Usually negative in non-ischemic type, but positive in about 90% of ischemic type, making it very useful for differentiating ischemic from non-ischemic type. It is also important as a predictor of neovascularization risk 9, 10).
Slit-lamp and fundus examination: Evaluation of hemorrhages in all four quadrants, optic disc edema, and macular edema. Check for iris neovascularization before dilation.
Intraocular pressure and gonioscopy: In ischemic type, perform gonioscopy monthly for 6 months to check for iris and angle neovascularization9). Since about one-third of non-ischemic type converts to ischemic type, angle observation should always be performed.
Differentiation of ischemic type (reduced b/a ratio)
Visual field testing
Large central scotoma in ischemic type
FA (Fluorescein Angiography): Essential for defining ischemic type according to CVOS criteria (capillary nonperfusion area ≥10 disc areas)9, 10). However, in the acute phase, extensive retinal hemorrhage may block fluorescence, making it difficult to assess nonperfusion areas. Therefore, re-examination may be needed several weeks later after hemorrhage absorption. Wide-field FA is improving the accuracy of evaluating peripheral ischemia and may be useful for predicting the risk of conversion from nonischemic to ischemic type9, 10). FA is also useful for differentiating collateral vessels (no leakage in late phase) from neovascularization (leakage in both early and late phases)18).
OCT (Optical Coherence Tomography): Very useful for quantitative assessment of macular edema and for monitoring treatment response9, 10). In CRVO, PAMM findings (hyperreflective bands) may be observed in the inner nuclear layer of the parafovea, reflecting peripheral arteriolar circulatory disturbance.
OCTA (Optical Coherence Tomography Angiography): Can detect capillary nonperfusion areas without contrast agent9). Enlargement of the FAZ (foveal avascular zone) area can also be assessed, but limited imaging range is a challenge.
ERG (Electroretinography): In ischemic type, reduced b/a ratio, decreased b-wave amplitude, and reduced flicker response are observed, useful for differentiating ischemic from nonischemic type.
Visual field testing: Shows a large central scotoma in ischemic type.
Papillophlebitis: Differential diagnosis is important in young-onset CRVO. CRVO associated with papillophlebitis may require systemic steroid therapy.
Hematologic diseases: If CRVO occurs in both eyes, it may be associated with hematologic diseases such as polycythemia, leukemia, or myeloproliferative disorders, requiring further investigation.
Diabetic retinopathy: Differential diagnosis is needed when diffuse retinal hemorrhage is present. CRVO is characterized by unilateral acute onset with uniform hemorrhage in all four quadrants, whereas diabetic retinopathy is bilateral, chronic, and has a different pattern of neovascularization.
Ocular ischemic syndrome: Chronic ocular ischemia due to carotid occlusive disease may present with fundus findings similar to CRVO. In CRVO, hemorrhage is more acute and massive, whereas in ocular ischemic syndrome, hemorrhage is moderate and hypotony and iris neovascularization tend to appear early.
Intravitreal anti-VEGF injection is the first-line treatment for macular edema associated with CRVO 9, 10). Its efficacy has been confirmed in multiple large-scale RCTs. Compared to BRVO, more injections are required, and especially in the ischemic type, complete cure is rare, but it is currently the treatment with the most expected visual improvement.
Ranibizumab
CRUISE trial: The 0.5 mg group showed a mean improvement of +14.9 letters at 6 months. 47.7% improved by ≥15 letters (sham group: 0.8 letters improvement, 16.9% improved by ≥15 letters) 12).
COMINO trial (CRVO/hemi-CRVO, n=729): Baseline BCVA 50.5 letters, CST 711.6 μm. The 6 mg group showed a mean improvement of +16.9 letters at 24 weeks. 56.6% improved by ≥15 letters. Non-inferiority to aflibercept was achieved 11).
CST change: CST reduction at 24 weeks was faricimab -461.6 μm vs. aflibercept -448.8 μm. Macular leakage resolution rate was faricimab 44.4% vs. aflibercept 30.0% 11).
Safety: The incidence of intraocular inflammation (IOI) was 2.2% for faricimab vs 1.1% for aflibercept. Serious IOI included 2 cases of uveitis in the faricimab group and 1 case of non-infectious endophthalmitis in the aflibercept group11).
Mechanism: It is a bispecific antibody that has anti-Ang-2 action in addition to anti-VEGF-A action.
Other anti-VEGF drugs and results of major clinical trials are shown below.
LEAVO trial (100 weeks, CRVO 463 patients): Improvement of +15.1 letters in the aflibercept group, +12.5 letters in the ranibizumab group, and +9.8 letters in the bevacizumab group. Aflibercept showed non-inferiority to ranibizumab, but comparison with bevacizumab was inconclusive16). Visual improvement of 15 letters or more was achieved in 52% of the aflibercept group, 47% of the ranibizumab group, and 45% of the bevacizumab group.
SCORE2 trial (CRVO/hemi-CRVO 362 patients): Visual acuity at 6 months (primary endpoint) was equivalent between bevacizumab and aflibercept17). Patients with poor response at 6 months received rescue treatment with dexamethasone implant. At 24 months, both groups showed a tendency for visual acuity to decline from 12 months.
Treatment duration: Approximately 56–75% of CRVO patients require continued anti-VEGF treatment beyond 5 years10). Regular long-term follow-up and continued treatment are essential; treatment interruption poses a risk of vision loss.
Dosing regimen: Starting with monthly injections, a treat-and-extend approach is widely adopted, extending the interval while confirming improvement of macular edema on OCT. For faricimab, extension up to 16-week intervals is being investigated11).
It is selected when anti-VEGF is ineffective or unsuitable.
Triamcinolone acetonide intravitreal injection (TAIV): In the SCORE study, visual improvement of 15 letters or more at 12 months was seen in 7% of the standard treatment (photocoagulation) group, 27% of the TAIV 1 mg group, and 26% of the 4 mg group. However, macular edema recurred in over 60% of cases, requiring additional injections. Since the 4 mg group had significantly higher rates of intraocular pressure elevation and cataract progression, 1 mg is recommended if used10).
Dexamethasone sustained-release implant (Ozurdex 0.7 mg): In the GENEVA trial (CRVO/BRVO 1267 patients), visual improvement began at day 30 and peaked at 90 days, but the effect disappeared by 6 months15). At 1 year, intraocular pressure ≥25 mmHg was observed in 16%. Compared to anti-VEGF, the risk of cataract and intraocular pressure elevation is higher.
Delayed-onset endophthalmitis: Delayed-onset endophthalmitis after DEX implant has also been reported, and foreign body sensation, redness, and vision loss require prompt attention 8).
PRP (panretinal photocoagulation) is used to manage neovascularization in ischemic CRVO 9). PRP does not improve visual acuity, but it prevents the development of neovascular glaucoma through regression and inhibition of neovascularization.
Non-ischemic type: Since neovascularization does not occur, PRP is not indicated. Prophylactic PRP is not recommended.
Ischemic type: About 30% of ischemic CRVO cases develop neovascularization, so PRP may be necessary. Currently, VEGF inhibitors can control neovascularization to some extent, so it is considered acceptable to perform PRP after neovascularization is observed. However, in cases of severe ischemia or in elderly patients, early PRP may be considered.
CVOS findings: The Central Vein Occlusion Study (CVOS) investigated grid laser photocoagulation for macular edema in CRVO, but no visual improvement was demonstrated. Therefore, grid laser photocoagulation for macular edema is not recommended. Dense panretinal photocoagulation is recommended only when iris or angle neovascularization is confirmed 9, 10). Combination with anti-VEGF drugs may facilitate complete PRP10).
After the approval of VEGF inhibitors, vitrectomy is not performed as a first-line treatment. No large-scale clinical trials have been conducted for macular edema due to CRVO, and evidence is not established. Radial optic neurotomy, which was previously performed based on the theoretical rationale of reducing venous pressure by decompressing the lamina cribrosa, is no longer performed because it can cause serious complications such as visual field defects and hemorrhage.
In cases with vitreous hemorrhage, PRP can be performed simultaneously with hemorrhage removal. In cases complicated by tractional vitreomacular syndrome (epiretinal membrane, vitreomacular traction), vitrectomy may contribute to improvement of macular edema.
Vaccine-associated CRVO: Steroid pulse therapy (methylprednisolone 1 g × 3 days) has been reported effective, with improvement in central foveal thickness from 823 μm to 166 μm and visual acuity from 2/60 to 6/9 6).
Anticoagulation therapy: May worsen visual prognosis and is not recommended 4).
Follow-up is performed according to the following schedule to assess treatment efficacy and detect complications early.
Non-ischemic type: Re-evaluate 4–6 weeks after onset, then follow up every 1–3 months depending on macular edema status. Perform OCT quantitative assessment of macular edema and visual acuity testing at each visit.
Ischemic type: Monthly visits are mandatory for the first 6 months after onset 9). Check for iris neovascularization before dilation, and monitor angle neovascularization by gonioscopy. Even after discontinuation of anti-VEGF therapy, the risk of neovascularization persists, so continued follow-up including gonioscopy is necessary.
Monitoring for conversion from non-ischemic to ischemic type: Approximately one-third of non-ischemic cases convert to ischemic type during follow-up, so angle observation should always be performed. Changes in RAPD, sudden visual acuity decrease, and worsening of hemorrhage are findings suggestive of conversion to ischemic type.
During anti-VEGF therapy: Evaluate macular edema by OCT every month after injection, and reinject if recurrence occurs. If stable, gradually extend the injection interval (treat-and-extend regimen).
Systemic management: Perform regular monitoring of blood pressure, blood glucose, and lipids in collaboration with internal medicine. Since CRVO carries a risk of contralateral eye involvement (1% per year), regular examination of both eyes is important 10).
QHow many anti-VEGF injections are typically needed?
A
In the CRUISE study, monthly injections for 6 months were administered, and significant visual improvement was confirmed 12). In actual treatment, monthly injections are started, and the interval is extended while confirming improvement of macular edema on OCT. It has been reported that approximately 56–75% of CRVO cases require treatment continuation beyond 5 years 10), making long-term regular follow-up essential. For faricimab, a treat-and-extend regimen with extension up to 16-week intervals is being considered 11).
Posterior to the lamina cribrosa, the central retinal artery and central retinal vein share a common adventitia (connective tissue sheath). Thickening and hardening of the arterial wall due to arteriosclerosis compress the adjacent vein, leading to endothelial damage → thrombus formation → occlusion 9, 10). In BRVO, occlusion mainly occurs at arteriovenous crossings, whereas in CRVO, occlusion near the lamina cribrosa is characteristic, but the mechanism of thrombus formation itself is considered similar to that of BRVO.
All three elements of Virchow’s triad (vascular injury, blood stasis, hypercoagulability) are involved. In BRVO, compression at the arteriovenous crossing is the main cause of occlusion, whereas in CRVO, the unique structure where the artery and vein share an adventitia in the narrow anatomical space of the lamina cribrosa forms the basis for occlusion.
Relationship between VEGF, Macular Edema, and Neovascularization
Venous occlusion → increased venous pressure → leakage of plasma components → retinal edema and hemorrhage. Retinal ischemia → hypoxia → overproduction of VEGF (vascular endothelial growth factor) → worsening of macular edema and formation of neovascularization (iris neovascularization, retinal neovascularization) occur 9, 10).
Among all retinal vascular diseases, RVO has been reported to have the highest levels of Ang-2 (angiopoietin-2). Ang-2 competes with Ang-1 for binding to Tie2, inhibiting vascular stabilization by Ang-1/Tie2 signaling 11). This provides the rationale for the mechanism of action of faricimab, which targets both VEGF-A and Ang-2.
This mechanism is the theoretical basis for anti-VEGF therapy and anti-Ang-2 therapy. In ischemic CRVO, VEGF production is significantly higher than in non-ischemic CRVO, and neovascularization involving the iris, angle, and retina progresses rapidly. VEGF inhibitors not only improve macular edema but also induce regression of neovascularization; however, recurrence occurs when drug efficacy wanes, requiring continuous administration.
In CRVO, impaired venous perfusion leads to circulatory disturbance at the peripheral arteriolar level. On OCTB-scan, it appears as a band-like hyperreflectivity in the inner nuclear layer of the parafovea (PAMM finding). It is inconspicuous on superficial en face images, but the hyperreflective area corresponding to the whitened retina is clearly visible on deep en face images.
COVID-19-related: Cytokine storm-induced endothelial damage, prothrombotic state, and direct infection of vascular endothelial cells collectively lead to hypercoagulability 3).
VITT (vaccine-induced thrombotic thrombocytopenia): Autoantibodies against platelet factor 4 (PF4) are formed, activating platelets and leading to thrombus formation 5).
PDE5 inhibitors: Under systemic hypotension, they induce retinal venous dilation and decreased blood flow velocity, increasing the risk of venous thrombosis 2).
Right heart dysfunction: Impaired venous drainage in the right heart increases ocular venous pressure, which can trigger bilateral CRVO 1).
QWhy is it called "90-day glaucoma"?
A
In ischemic CRVO, extensive retinal ischemia produces large amounts of VEGF, inducing iris neovascularization. Iris rubeosis occurs in 45–80% of ischemic cases, and these new vessels obstruct the angle, causing neovascular glaucoma. It often appears within 2–4 months (about 90 days) after onset, hence the name “90-day glaucoma” 9, 10). Regular angle examination is essential for early detection, and PRP and anti-VEGF therapy determine visual prognosis.
7. Latest Research and Future Perspectives (Investigational Reports)
Reports on the risk of retinal vein occlusion after COVID-19 infection are accumulating.
RiaziEsfahani H et al. (2024) reported a case of hemi-CRVO in a young patient with a history of COVID-19 3). It suggested that RVO risk may persist for several months after infection.
In a review of 20 cases of RVO after vaccination, 7 cases were in individuals under 40 years of age 6). The incidence of thrombosis after ChAdOx1 (AstraZeneca) vaccination is reported as 1.13 per 100,000 doses, and a hypercoagulable state via VITT mechanism has been proposed 5, 6).
Torkashvand A et al. (2023) reported a case of combined CRVO and central retinal artery occlusion after sildenafil use 2). OCTA documented decreased vascular density, highlighting the impact of PDE5 inhibitors on retinal circulation.
Advances in wide-field imaging technology have refined the assessment of peripheral ischemic areas 9, 10). Wide-field FA can now detect non-perfused areas in the peripheral retina that were difficult to evaluate with conventional standard FA, improving the prediction of transition risk from non-ischemic to ischemic type. OCTA allows quantitative evaluation of FAZ enlargement and capillary density reduction without contrast agents, and its usefulness in follow-up of RVO patients has been reported. However, due to current limitations in imaging range, it has not yet fully replaced FA9).
Automated detection of RVO from color fundus photographs using deep learning algorithms has been studied, with good discriminative ability reported 10). Future applications in screening and telemedicine are expected.
From 2021 to 2024, the FDA approved two ranibizumab biosimilars (ranibizumab-nuna [Byooviz], ranibizumab-eqrn [Cimerli]) and four aflibercept biosimilars (aflibercept-jbvf [Yesafili], aflibercept-yszy [Opuviz], aflibercept-mrbb [Ahzantive], aflibercept-ayyh [Pavblu]) for the indication of macular edema due to RVO10). The widespread use of biosimilars is expected to improve treatment access and reduce healthcare costs.
In the COMINO trial of faricimab, after week 24 (Part 2: weeks 24-72), all patients were switched to faricimab 6 mg T&E dosing (up to 16-week intervals). Durability and long-term safety data at 72 weeks are expected to be published in the future, with important results anticipated regarding the potential for extended dosing intervals in RVO treatment 11).
Cases of right heart dysfunction discovered through bilateral CRVO have been reported, highlighting the importance of cross-disciplinary collaboration with cardiac surgery and cardiology 1).
Matsuo T, Masuda Z, Sugiyama H, Nakamura K. Sequential Bilateral Central Retinal Vein Occlusion With Differential Long-Term Outcomes Following Cardiac Surgery. Cureus. 2025;17(12):e100045. doi:10.7759/cureus.100045. PMID:41583289; PMCID:PMC12831097.
Torkashvand A, et al. Central retinal vein and artery occlusion associated with sildenafil: a case report and review of the literature. J Med Case Rep. 2023;17:399. doi:10.1186/s13256-023-04104-8. PMID:37726852; PMCID:PMC10510287.
RiaziEsfahani H, et al. Hemicentral retinal vein occlusion in a patient with a history of coronavirus disease 2019 infection: a case report and review of the literature. J Med Case Rep. 2024;18:50. doi:10.1186/s13256-023-04333-x. PMID:38341577; PMCID:PMC10859018.
Staropoli PC, et al. CRVO associated with COVID-19 and MTHFR mutation in a 15-year-old male. Am J Ophthalmol Case Rep. 2022;26:101522. doi:10.1016/j.ajoc.2022.101522. PMID:35469132; PMCID:PMC9020500.
Sonawane NJ, Yadav D, Kota AR, Singh HV. Central retinal vein occlusion post-COVID-19 vaccination. Indian journal of ophthalmology. 2022;70(1):308-309. doi:10.4103/ijo.IJO_1757_21. PMID:34937265; PMCID:PMC8917569.
Dutta Majumder P, et al. Retinal venous occlusion following COVID-19 vaccination: Report of a case after third dose and review of the literature. Indian J Ophthalmol. 2022;70:2191-4. doi:10.4103/ijo.IJO_592_22. PMID:35648014; PMCID:PMC9359265.
Zhao J, et al. Chylous aqueous humor caused by hyperlipidemia: A case report and literature review. Medicine. 2023;102:e34972. doi:10.1097/MD.0000000000034972. PMID:37682141; PMCID:PMC10489254.
Tripathi AN, et al. Atypical Delayed-Onset Endophthalmitis Following Intravitreal Dexamethasone Implant Managed Without Implant Removal: A Rare Case Report and Literature Review. Rom J Ophthalmol. 2024;68(4):343-8. doi:10.22336/rjo.2024.64. PMID:39936053; PMCID:PMC11809834.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, Ying GS. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P288-P320. doi:10.1016/j.ophtha.2019.09.029. PMID:31757503.
Flaxel CJ, et al. Retinal Vein Occlusions Preferred Practice Pattern. Ophthalmology. 2024;131:P288-P332.
Tadayoni R, Paris LP, Danzig CJ, Abreu F, Khanani AM, Brittain C, et al. Efficacy and Safety of Faricimab for Macular Edema due to Retinal Vein Occlusion: 24-Week Results from the BALATON and COMINO Trials. Ophthalmology. 2024;131(8):950-960. doi:10.1016/j.ophtha.2024.01.029. PMID:38280653.
Campochiaro PA, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study (CRUISE). Ophthalmology. 2010;117(6):1124-1133.e1. doi:10.1016/j.ophtha.2010.02.022. PMID:20381871.
Boyer D, et al. Vascular endothelial growth factor Trap-Eye for macular edema secondary to central retinal vein occlusion: six-month results of the phase 3 COPERNICUS study. Ophthalmology. 2012;119(5):1024-1032. doi:10.1016/j.ophtha.2012.01.042. PMID:22440275.
Holz FG, et al. VEGF Trap-Eye for macular oedema secondary to central retinal vein occlusion: 6-month results of the phase III GALILEO study. Br J Ophthalmol. 2013;97(3):278-284. doi:10.1136/bjophthalmol-2012-301504. PMID:23298885.
Haller JA, et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion (GENEVA). Ophthalmology. 2010;117(6):1134-1146.e3. doi:10.1016/j.ophtha.2010.03.032. PMID:20417567.
Hykin P, et al. Clinical Effectiveness of Intravitreal Therapy With Ranibizumab vs Aflibercept vs Bevacizumab for Macular Edema Secondary to Central Retinal Vein Occlusion: A Randomized Clinical Trial. JAMA Ophthalmol. 2019;137(11):1256-1264. doi:10.1001/jamaophthalmol.2019.3305. PMID:31465100; PMCID:PMC6865295.
Scott IU, et al. Effect of bevacizumab vs aflibercept on visual acuity among patients with macular edema due to central retinal vein occlusion: the SCORE2 randomized clinical trial. JAMA. 2017;317(20):2072-2087. doi:10.1001/jama.2017.4568. PMID:28492910; PMCID:PMC5710547.