Diabetic retinopathy (DR) is a retinal microvascular disorder caused by metabolic abnormalities due to hyperglycemia, which induce various cytokines and chemokines. This leads to diverse fundus lesions and is considered one of the three major complications along with diabetic neuropathy and diabetic nephropathy. In recent years, it has been redefined as a “neurovascular disease” rather than just a microvascular disease 2).
It is the second leading cause of acquired visual impairment, with approximately 3,000 people becoming blind annually due to DR.
Diabetic macular edema (DME) is the most common type of diabetic maculopathy. Diabetic maculopathy includes three types: macular edema, ischemic maculopathy, and retinal pigment epitheliopathy, but macular edema is the most frequent and clinically significant cause of vision loss. DME can occur at any stage of DR. The pathophysiology of DME is complex, involving multiple factors such as increased vascular permeability, blood flow impairment due to vascular occlusion, decreased colloid osmotic pressure, and traction from the posterior hyaloid membrane.
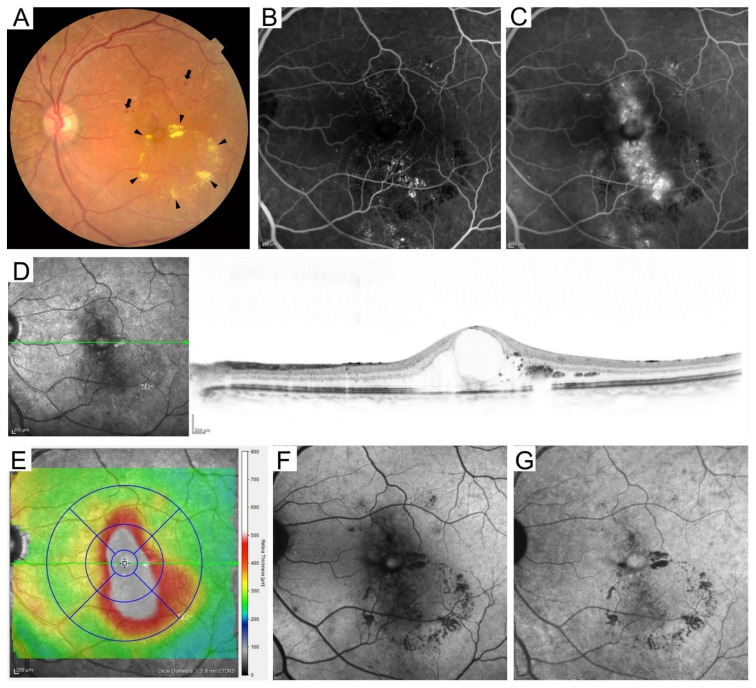
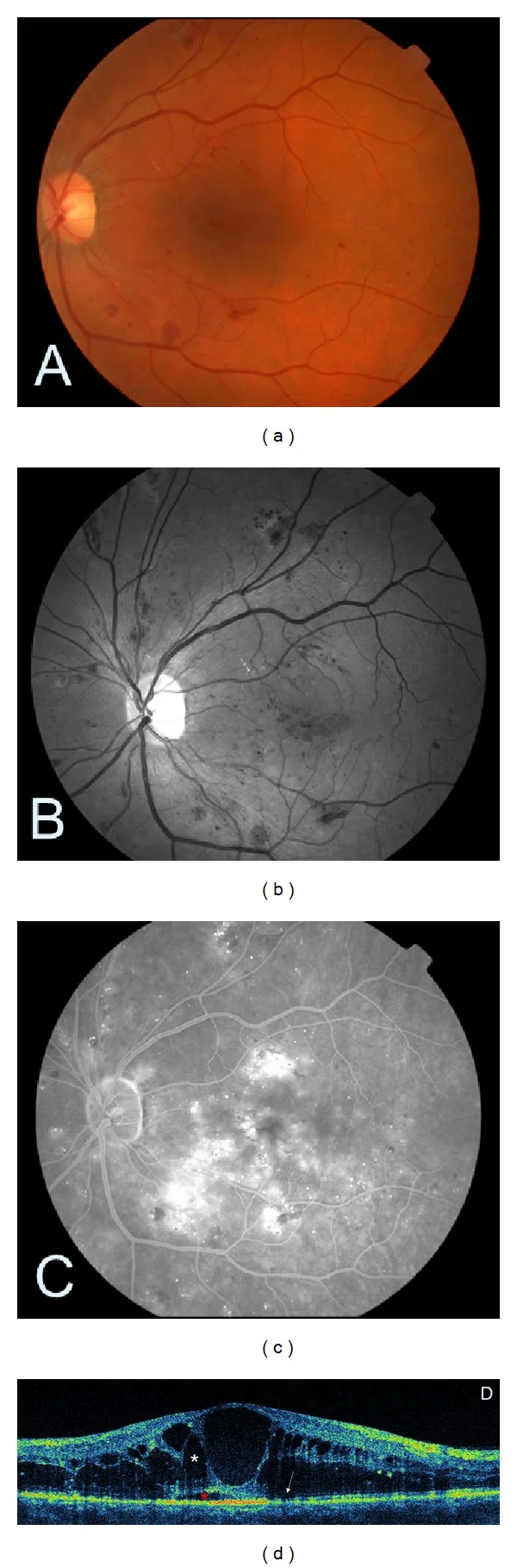
Murakami T, Ishihara K, Terada N, et al. Pathological Neurovascular Unit Mapping onto Multimodal Imaging in Diabetic Macular Edema. Medicina (Kaunas). 2023;59:896. Figure 1. PMID: 37241128; PMCID: PMC10221113; DOI: 10.3390/medicina59050896. License: CC BY.
Fundus photograph shows retinal hemorrhages and hard exudates. FA reveals macular leakage, and OCT shows cystoid spaces and retinal thickening. As an entry point to understanding DME, it is helpful to correlate fundus photography, angiography, and OCT.
Major epidemiological data in Japan are shown below1).
976 Japanese patients with type 2 diabetes followed for an average of 8.3 years: DR incidence rate 3.98% per year
JDCS (1,221 patients, mean age 58.2 years, HbA1c 8.2%) 8-year follow-up: DR incidence rate 3.83% per year
JDCS 410 patients: progression rate from mild NPDR to severe NPDR/PDR 2.11% per year
DR prevalence in Asia including Japan: 19.9%
DR prevalence in Japan: 23.5% (mild to moderate NPDR 18.5%, DME 3.7%)
Approximately 30% of patients already have DR at the time of type 2 diabetes diagnosis
Globally, 34.6% of diabetic patients (approximately 93 million) have DR2). In 2020 estimates, DR affected 131.2 million people, vision-threatening DR (VTDR) 28.54 million, and clinically significant macular edema (CSME) 18.83 million, with projections of 160.5 million by 20452). In type 1 diabetes, approximately 90% develop DR after 20 years of disease11).
QHow often does diabetic retinopathy occur?
A
In large Japanese cohorts, DR develops at a rate of 3.8–4.0% per year, and approximately 30% of patients already have DR at the time of type 2 diabetes diagnosis1). Globally, 34.6% of diabetic patients (approximately 93 million) have DR2), and about 90% of type 1 diabetes patients develop DR after 20 years11).
Rapid progression of visual field constriction: May be caused by markedly elevated intraocular pressure due to neovascular glaucoma (NVG).
QWhat symptoms appear in early diabetic retinopathy?
A
In the early stage, there are almost no subjective symptoms, and the disease progresses asymptomatically. When symptoms such as decreased visual acuity, floaters, or metamorphopsia appear, moderate to severe lesions are often already present. Therefore, once diagnosed with diabetes, regular fundus examinations are necessary even without symptoms.
The main fundus findings by disease stage are shown below.
Simple Retinopathy
Microaneurysms: The earliest finding of DR. They appear as punctate hyperfluorescent spots on fluorescein angiography.
Retinal hemorrhages: Dot and blot hemorrhages. They occur when red blood cells leak from capillaries.
Hard exudates: Plasma components leak due to increased vascular permeability, and lipids are deposited.
Preproliferative Retinopathy
Soft exudates (cotton-wool spots): Localized infarcts due to impaired axonal transport in the optic nerve fibers. They reflect retinal ischemia.
Beaded venous dilation and loop formation: Appears adjacent to areas of vascular occlusion.
IRMA (Intraretinal Microvascular Abnormalities): Shunt formation around non-perfused areas. A key differentiating feature from neovascularization is the lack of prominent leakage on fluorescein angiography.
Proliferative Retinopathy
Neovascularization: Appears on the retina and optic disc due to excessive VEGF production from widespread capillary occlusion. Shows profuse fluorescein leakage on angiography.
Fibrovascular proliferative membrane: Forms as fibroblast-like cells proliferate around new vessels.
Tractional retinal detachment: Occurs when vitreous traction is added to the adhesion between the proliferative membrane and the retina. Involvement of the macula leads to poor visual prognosis.
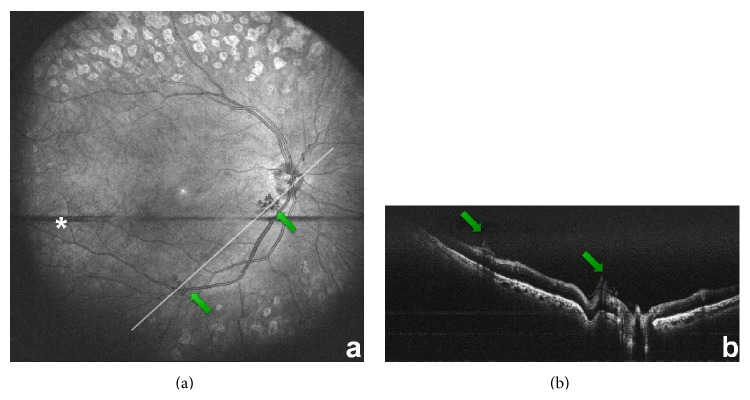
Reznicek L, Kolb JP, Klein T, et al. Wide-Field Megahertz OCT Imaging of Patients with Diabetic Retinopathy. J Diabetes Res. 2015;2015:305084. Figure 5. PMID: 26273665; PMCID: PMC4530264; DOI: 10.1155/2015/305084. License: CC BY.
In proliferative diabetic retinopathy, new vessels appear on the optic disc and retinal surface. Correlating wide-field en face images with tomographic images makes it easier to identify fibrovascular lesions protruding onto the retinal surface.
International Clinical Diabetic Retinopathy Severity Scale (ICDR) and New Fukuda Classification
Old neovascularization / VH / proliferative tissue
When the condition remains quiescent for 6 months or more after treatment, it is called inactive proliferative retinopathy. Complications are noted as M (macular lesion), D (tractional RD), G (NVG), N (ischemic optic neuropathy), P (photocoagulation), and V (vitrectomy).
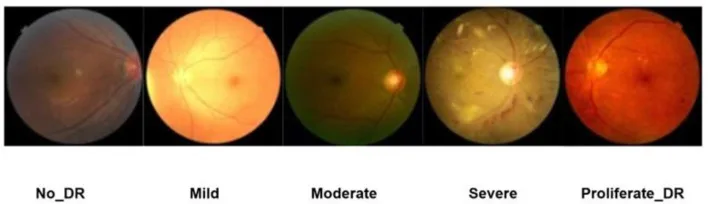
Al-Dolat W, Alhatamleh S, Alqudah N, et al. Enhancing fundus image analysis for diabetic retinopathy using CheXNet with CBAM and Grad-CAM visualization. Front Med (Lausanne). 2026;13:1732109. Figure 2. PMID: 41822901; PMCID: PMC12975473. DOI: 10.3389/fmed.2026.1732109. License: CC BY 4.0.
This is a fundus image schematically representing A1, A2, B1, and B2 of the new Fukuda classification for educational purposes. Since it is not an actual patient image, diagnosis should be made by integrating actual fundus photographs, OCT, FA/OCTA, and clinical course.
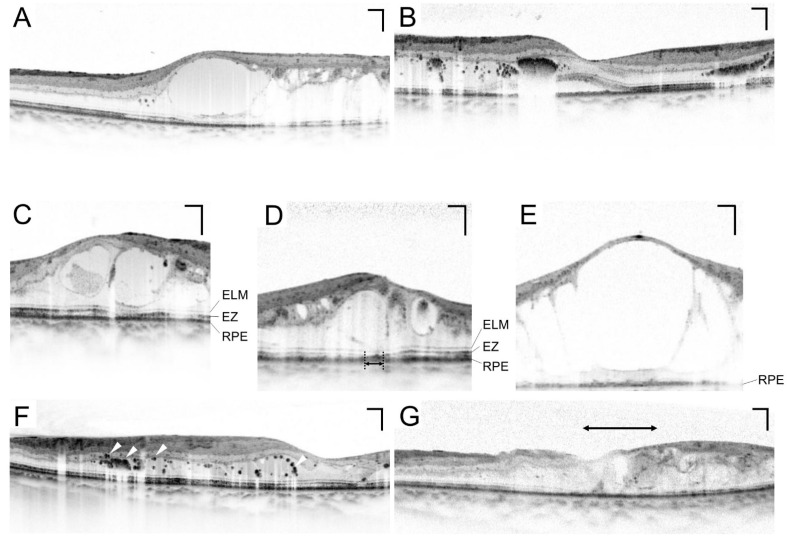
OCT tomographic images of macular edema are evaluated based on a combination of three basic types: retinal swelling, cystoid macular edema, and serous retinal detachment.
Murakami T, Ishihara K, Terada N, et al. Pathological Neurovascular Unit Mapping onto Multimodal Imaging in Diabetic Macular Edema. Medicina (Kaunas). 2023;59:896. Figure 5. PMID: 37241128; PMCID: PMC10221113; DOI: 10.3390/medicina59050896. License: CC BY.
OCT of DME shows a combination of cystoid spaces, serous retinal detachment, outer layer disruption, and hyperreflective foci. Not only retinal thickness but also the preservation of the external limiting membrane and ellipsoid zone are related to visual prognosis.
Clinically significant macular edema (CSME) is defined by the ETDRS as meeting any of the following criteria 2):
A. Retinal thickening within 500 μm of the fovea
B. Hard exudates within 500 μm of the fovea with adjacent retinal thickening
C. An area of thickening of at least 1 disc area, part of which is within 1,500 μm of the fovea
A central retinal thickness of 300 μm or more on SD-OCT is used as the threshold for DME involving the fovea (by device: Spectralis 320/305 μm, Cirrus 305/290 μm, Stratus 250/250 μm, male/female) 1). The international severity classification of DME has three stages: mild (thickening or hard exudates away from the fovea), moderate (near the fovea but not involving it), and severe (involving the fovea). DME increases with progression of NPDR, complicating 1.7–6.3% of mild NPDR and 20.3–63.2% of moderate NPDR 1).
The main risk factors associated with the progression of DR are shown below.
Risk Factor
Main Evidence
Duration of diabetes
The greatest risk factor. About 30% of patients with type 2 DM already have DR at diagnosis 1)
Glycemic control
HbA1c <7.0% prevents microvascular complications (Kumamoto Study). A 1% reduction in HbA1c reduces the risk of microvascular complications by 37% (UKPDS) 1)
Hypertension
WESDR: A 10 mmHg increase in systolic blood pressure increases the risk of early DR by 10% and proliferative DR/DME by 15%. UKPDS: A 10 mmHg reduction decreases DR progression by 35% and vision loss by 47% 1)
Dyslipidemia
Fenofibrate (FIELD Study): 31% reduction in introduction of photocoagulation, 30% reduction in proliferative DR, 31% reduction in DME. ACCORD Eye Study: 40% reduction in odds of DR progression1)
Renal dysfunction
Proteinuria and decreased GFR correlate with DR prevalence. Nephropathy → 29% increased risk of PDR progression1)
Pregnancy
No pre-existing DR → onset of DR during pregnancy 8–33%. Pre-existing NPDR → worsening during pregnancy 10–67%1)
Severe hypoglycemia
DR incidence increases approximately 4-fold (JDCS)1)
UKPDS: 1% reduction in HbA1c reduces risk of microvascular complications by 37%
DCCT/EDIC: Early intensive insulin therapy group significantly suppressed DR progression and DME occurrence even during long-term follow-up
J-DOIT3: Multifactorial intervention group showed reduced risk of DR progression
Steno-2 Study: Intensive multifactorial therapy reduced risk of DR progression by 58%
On the other hand, when blood glucose is rapidly improved in patients with long-term poor glycemic control, transient worsening of diabetic retinopathy (DR), known as “early worsening,” may occur. Since visual acuity decline persists in about 50% of cases, gradual improvement in blood glucose is desirable, and collaboration with an internist is important 1).
Additionally, retinal cells once exposed to hyperglycemia undergo epigenetic changes, leading to “metabolic memory,” where lesions persist or progress even after normalization of blood glucose 11). Downregulation of SOD2 and hypermethylation of mitochondrial DNA have been reported as mechanisms.
Fenofibrate: The FIELD Study and ACCORD Eye Study showed significant reduction in the frequency of photocoagulation and progression of DR 1).
Statins: Registry data showed a 40% reduction in the risk of developing DR compared to non-users 1).
RAS inhibitors: In the DIRECT study, candesartan administration led to 34% regression of DR. ACE inhibitors have also been reported to be more effective than ARBs 1)9).
QTo what level should HbA1c be controlled to suppress progression?
A
Targeting HbA1c below 7.0% prevents microvascular complications (Kumamoto Study) 1). A 1% reduction in HbA1c reduces the risk of microvascular complications by 37% (UKPDS) 1). Since cells once exposed to hyperglycemia retain “metabolic memory,” long-term follow-up is necessary even after blood glucose normalization 11).
Sikorski et al. Mediators Inflamm. 2013;2013:434560. Figure 4. PMCID: PMC3863575. License: CC BY.
Even if findings are subtle on color fundus photography, red-free images and FA clearly show hemorrhages, microaneurysms, and leakage. OCT allows direct evaluation of cystoid edema involving the fovea, directly linked to treatment decisions.
QWhen should a person diagnosed with diabetes have their first eye exam?
A
For type 2 diabetes, about 30% already have DR at diagnosis, so an eye exam at diagnosis is recommended 1). For type 1 diabetes, the exam should be within 5 years after diagnosis 1). If pregnancy is complicated, an exam should be done as early as possible in the first trimester, and follow-up every 3 months during pregnancy is necessary 1).
Grid coagulation: Irradiates areas of diffuse leakage or non-perfusion.
Modified ETDRS method: Avoids irradiation within 500 μm of the foveal center, performed with low power and wide spacing1).
Caution: Risk of atrophic creep (scar expansion) and subretinal fibrosis1).
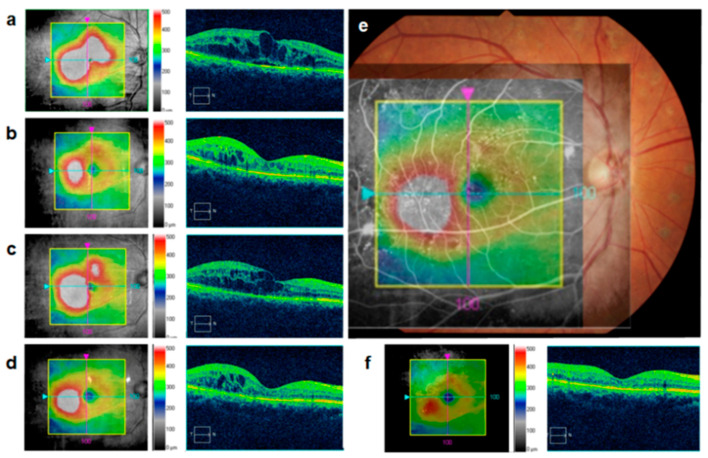
Medicina (Kaunas). 2023;59:435. Figure 4. PMCID: PMC10051835. License: CC BY.
After anti-VEGF therapy, localized edema may persist around microaneurysms. Overlaying the OCT map, OCT cross-section, and fundus photograph helps identify areas where additional laser or treatment interval adjustment should be considered.
Panretinal photocoagulation (PRP): Coagulates ischemic retina to reduce VEGF production and regress neovascularization. It is performed without exception for high-risk PDR 1). Recommended for NPA involving 3 or more quadrants 1). According to ETDRS criteria, standard settings are 0.2 seconds, 200 μm, 200 mW 1).
Selective retinal photocoagulation: Identifies NPA on FA and selectively applies treatment to those areas. Often performed for preproliferative DR 1).
Anti-VEGF (PDR): In DRCR Protocol S, intravitreal ranibizumab was non-inferior to PRP (2-year follow-up) 2). However, discontinuation of treatment carries a risk of neovascularization recurrence, requiring continuous outpatient management.
DRCR Protocol W: Prophylactic anti-VEGF injection for NPDR prevents development of PDR/DME, but long-term visual outcomes are equivalent to initial observation 2).
Vitrectomy indications: Tractional RD threatening the macula, combined rhegmatogenous RD, persistent/recurrent VH, NVG1). Minimally invasive vitrectomy surgery (MIVS) has become less invasive. Visualization with triamcinolone and ILM staining with brilliant blue G (BBG) have improved surgical precision.
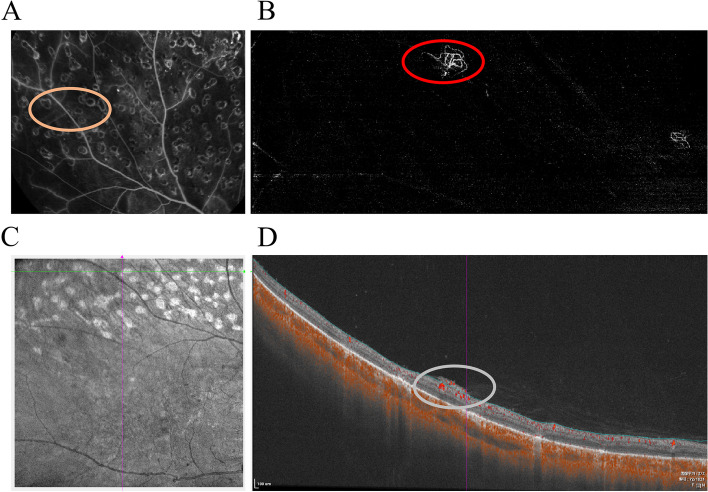
Yang Y, Li F, Liu T, et al. Comparison of widefield swept-source optical coherence tomographic angiography and fluorescein fundus angiography for detection of retinal neovascularization with diabetic retinopathy. BMC Ophthalmol. 2023;23(1):315. Figure 3. PMID: 37438731; PMCID: PMC10337091; DOI: 10.1186/s12886-023-03073-2. License: CC BY.
In PDR after PRP, FA and OCTA are useful for assessing neovascular activity. After anti-VEGF injection, leakage and blood flow signals may decrease, so pre- and post-treatment images should be compared in the same area.
QWhat is the choice of anti-VEGF drug for DME treatment?
A
For DME involving the fovea, anti-VEGF therapy is the first-line treatment 1). Ranibizumab, aflibercept, faricimab, and brolucizumab are all effective, with faricimab (up to q16w) and brolucizumab (≥50% at q12w) attracting attention for their potential to extend dosing intervals 5)9). If anti-VEGF is insufficient, consider steroid therapy with triamcinolone or dexamethasone implant 2).
The basic pathologies of DR are broadly classified into three categories: increased vascular permeability, vascular occlusion, and angiogenesis. The stages of simple retinopathy, preproliferative retinopathy, and proliferative retinopathy roughly correspond to these basic pathologies.
Four Major Metabolic Pathways Induced by Hyperglycemia
The retina expresses a local RAAS independent of the circulatory system9). The classical pathway (ACE/AngII/AT1R axis) promotes pericyte apoptosis, leukocyte stasis, and BRB breakdown, while the protective pathway (ACE2/Ang-(1-7)/Mas axis) counteracts it. Intraretinal AngII concentration is higher than in circulation, and the DIRECT trial showed that candesartan treatment led to 34% regression of DR9).
Retinal cells once exposed to hyperglycemia maintain epigenetic changes even after normalization of blood glucose (SOD2 suppression, mitochondrial DNA hypermethylation) 11). Mechanisms reported include increased ROS production from mitochondrial electron transport chain Complex I/III, excessive mitochondrial fragmentation due to Drp1/OPA1 imbalance, and impaired antioxidant response via Nrf2/KEAP1 and SIRT1.
DR has been redefined as a “neurovascular disease” 2), and GCIPL thinning can be detected by OCT before vascular lesions appear 13). Macular NFL thins by 0.25 μm per year, and GCIPL by 0.29 μm per year. Müller cell gliosis (increased GFAP) and microglial activation have also been confirmed. Fractalkine (CX3CL1) is produced by retinal ganglion cells and acts on the CX3CR1 receptor to exert anti-inflammatory and neuroprotective effects 10).
In diabetic patients, glucose concentration in the vitreous increases, and glycation of collagen fibers progresses. The degree of glycation correlates with DR progression, and collagen structural changes promote liquefaction, contraction of the vitreous cortex, and posterior vitreous detachment (PVD). If complete PVD without traction occurs, progression to proliferative DR is almost absent. In contrast, incomplete PVD (strong adhesion between vitreous and proliferative tissue) leads to persistent vitreous traction, making tractional retinal detachment and vitreous hemorrhage more likely.
QCan diabetic retinopathy be prevented by normalizing blood glucose?
A
Blood glucose control is most important for preventing and slowing DR progression, with a target HbA1c below 7.0% 1). However, according to the concept of “metabolic memory,” cells once exposed to hyperglycemia retain epigenetic changes, and lesions may persist or progress even after glucose normalization 11). The DCCT/EDIC follow-up study showed that early intensive therapy suppressed DR progression over a long period.
Aflibercept 8 mg was approved for DME indication in 2023, with expected extension of up to 16-week intervals 2). In DRCR Protocol W, prophylactic anti-VEGF for severe NPDR prevented PDR/DME onset, but long-term visual outcomes were equivalent to initial observation 2).
LumineticsCore (formerly IDx-DR) is the first autonomous AI-based retinal diagnostic system approved by the FDA in 2018 that does not require physician interpretation 3). Deep learning models have reported a sensitivity of 96.8% and specificity of 87% 3), and new systems such as EyeArt and AEYE-DS are also being developed 2).
Administration of a soluble fractalkine-expressing AAV vector (rAAV-sFKN) has shown improvement in visual acuity, reduction in fibrin leakage, and normalization of microglia 10). It has neuroprotective and anti-inflammatory mechanisms distinct from anti-VEGF therapy.
The EUROCONDOR phase II-III trial (NCT01726075) evaluated somatostatin and brimonidine eye drops, but overall analysis did not show efficacy; however, in the subgroup with abnormal baseline mfERG, progression of neuronal dysfunction was halted 13). A 36-month double-blind RCT of citicoline plus vitamin B12 eye drops reported suppression of functional, structural, and vascular progression in mild DR 13).
miRNAs are attracting attention as “master regulators” that integratively modulate multiple axes of DR pathology (oxidative stress, inflammation, neurodegeneration, vascular dysfunction) 14). The possibility of SIRT1 stabilization by miR-195 inhibition and VEGF-A translational inhibition by miR-497a-5p has been shown; approximately 350 miRNAs are expressed in the retina, and more than 86 are aberrantly expressed in DR models.
Metformin has pleiotropic effects including antioxidant, anti-inflammatory, anti-angiogenic, and neuroprotective actions via AMPK activation, and observational studies have shown an aHR of 0.29 for STDR (sight-threatening DR) in users 12). However, RCT data for ophthalmic indications are currently insufficient.
The nonsteroidal MR antagonist finerenone has been shown to reduce BRB breakdown, angiogenesis, and inflammation in preclinical models, and the significance of MR as an independent therapeutic target for DR is being investigated 9).
Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2024;131(1):P49-P130.
Huang Y, et al. Advances in diabetic retinopathy: epidemiology, pathogenesis, diagnosis, and treatment. Front Endocrinol. 2025;16:1664604.
Beuran DI, et al. Sterile endophthalmitis after intravitreal injection of triamcinolone acetonide. Rom J Ophthalmol. 2024;68(1):2-7.
Debdulal Chakraborty, Jay U. Sheth, Subhendu Boral, Tushar K. Sinha. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: A real-world case series. American Journal of Ophthalmology Case Reports. 2021;24:101197. doi:10.1016/j.ajoc.2021.101197.
Kikuchi Y, Odashima Y, Yoshikawa K, Oda T, Tanaka F, Oikawa H, Ishigaki Y, Asahi K. Renal thrombotic microangiopathy and nephrotic proteinuria induced by intravitreal injection of aflibercept for diabetic macular edema. BMC nephrology. 2022;23(1):348. doi:10.1186/s12882-022-02986-2. PMID:36309669; PMCID:PMC9618189.
Takao Hirano, Yuichi Toriyama, Yoshiaki Takahashi, Ken Hoshiyama, Toshinori Murata. Retinal arterial occlusive vasculitis after multiple intravitreal brolucizumab injections for diabetic macular edema. American Journal of Ophthalmology Case Reports. 2023;29:101788. doi:10.1016/j.ajoc.2022.101788.
O’Leary F, Campbell M. The blood-retina barrier in health and disease. The FEBS journal. 2023;290(4):878-891. doi:10.1111/febs.16330. PMID:34923749.
Li X, et al. The role of the renin-angiotensin-aldosterone system in diabetic retinopathy: mechanisms and therapies. Arch Endocrinol Metab. 2024;68:e230292.
Lee CY, Yang CH. The role of fractalkine and its receptor CX3CR1 in diabetic retinopathy. Int J Mol Sci. 2025;26(1):378.
He W, et al. Oxidative stress and diabetic retinopathy: molecular mechanisms, pathological roles, and therapeutic implications. Front Immunol. 2025;16:1571576.
Hamza Alasbily, Fardous Ali Fahmi, Majdi Abdulhamid Abdala, Adnan Fouad Asheibi, Ahmed Adeil Amhidi, Ala Abed Elallegy, Adela H. Elamami. Metformin in Diabetic Retinopathy: Mechanisms, Therapeutic Potential, and Barriers. Cureus. 2025. doi:10.7759/cureus.87455.
Bianco L, Arrigo A, Aragona E, et al. Neuroinflammation and neurodegeneration in diabetic retinopathy. Front Aging Neurosci. 2022;14:937999. doi:10.3389/fnagi.2022.937999.
Chen J, Zhang J, Li C, Wang L, Tao L, Xue S, et al. Targeting microRNAs in diabetic retinopathy: from pathogenic mechanisms to therapeutic potentials. Frontiers in endocrinology. 2025;16:1664604. doi:10.3389/fendo.2025.1664604. PMID:41064354; PMCID:PMC12500462.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.