Hypertension and dyslipidemia promote systemic arteriosclerosis, which is reflected in fundus findings. Retinal vessels are the only vascular bed in the body that can be directly observed macroscopically, and they are considered a “window” reflecting systemic vascular status 1).
Hypertensive retinopathy is an independent indicator of cardiovascular risk, and changes in retinal arterioles can be used to assess the severity of hypertension and the degree of arteriosclerosis 1). Hypertension is the most important risk factor for retinal vein occlusion (RVO), with an odds ratio of 3.0 to 5.0 reported 2). Hypertension and dyslipidemia are also major risk factors for retinal artery occlusion (RAO) 3).
In dyslipidemia, in addition to promoting arteriosclerosis, characteristic fundus findings such as Hollenhorst plaques (cholesterol emboli) occur. Xanthelasma and arcus senilis are also important ocular findings of dyslipidemia 6).
The fundus is the only site in the body where blood vessels can be directly observed, serving as a window for cardiovascular risk assessment 1)
Hypertension is the most important risk factor for retinal vein occlusion, with an OR of 3.0 to 5.0 2)
Retinal artery occlusion is considered a “retinal stroke” and requires urgent evaluation similar to stroke 3)
Detection of Hollenhorst plaques is an indicator of carotid artery disease and stroke risk
Ocular findings of dyslipidemia include xanthelasma, arcus corneae, and lipemia retinalis6)
QDoes high blood pressure affect the eyes?
A
High blood pressure is reflected as vascular changes in the ocular fundus, increasing the risk of retinal vein occlusion, retinal artery occlusion, and ischemic optic neuropathy. Hypertensive fundus changes are evaluated using the Keith-Wagener-Barker (KWB) classification, and grade II or higher is associated with a significantly increased risk of cardiovascular events. The ocular fundus is the only site where systemic vascular status can be directly observed, and fundus examination is useful for cardiovascular risk assessment.
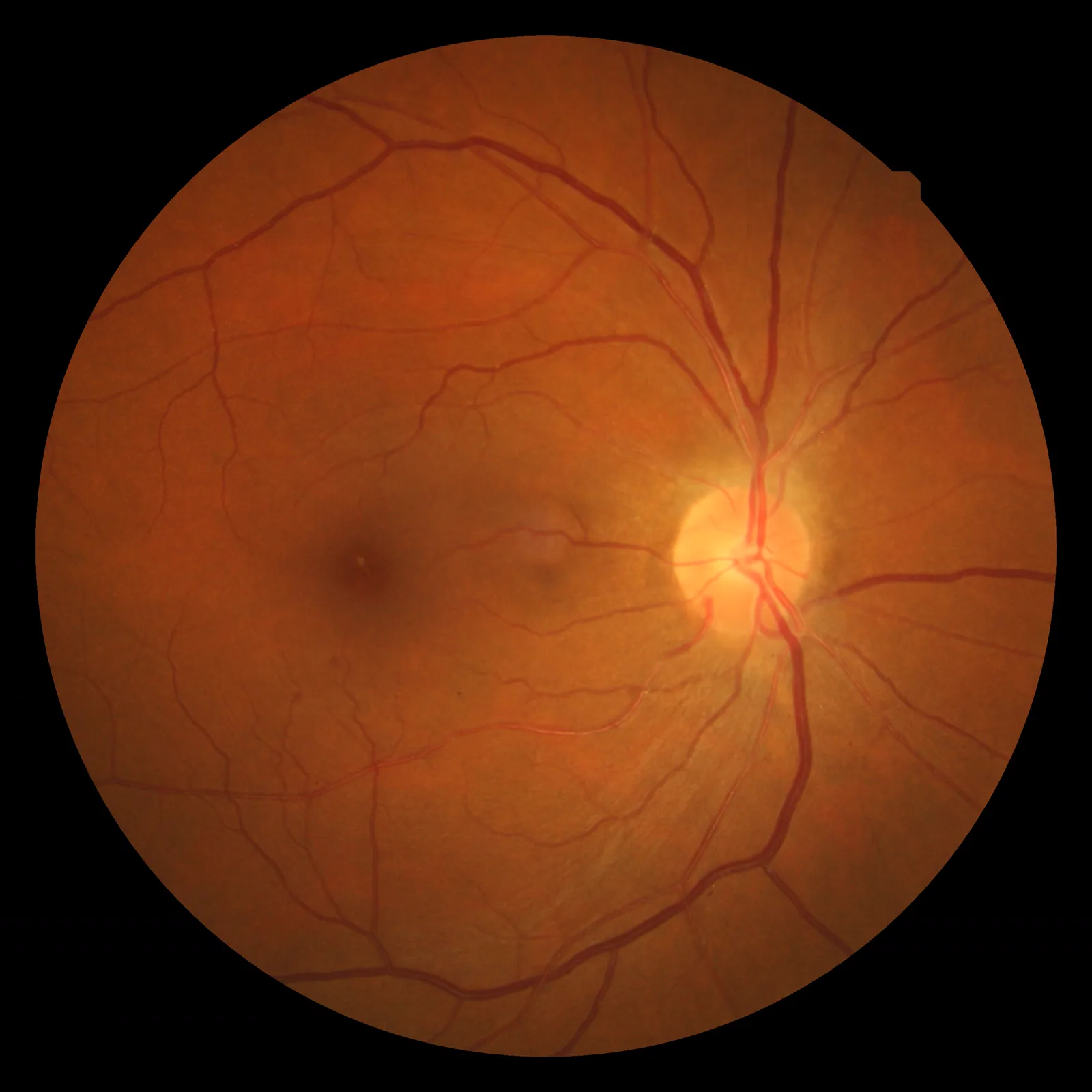
Wood F. Hypertensive retinopathy fundus photograph. 2009. Figure 1. Source ID: Wikimedia Commons (File:Hypertensiveretinopathy.jpg). License: CC BY 3.0.
Fundus photograph showing retinal arteriolar narrowing and arteriovenous crossing phenomenon (KWB grade II) due to hypertension. Corresponds to the arteriovenous crossing phenomenon and arteriolar changes discussed in section “2. Hypertensive fundus changes”.
Hypertension causes characteristic changes in the retinal arterioles. There are several classification systems, including the Keith-Wagener-Barker (KWB) classification, which is still used in health checkups.
Keith-Wagener-Barker (KWB) classification:
Grade
Fundus findings
I
Irregularity of arteriolar caliber, mild increase in light reflex
In KWB classification, grade II or higher indicates organic changes in retinal arterioles, significantly increasing the risk of stroke and coronary artery disease5). Grade IV (malignant hypertension) is an ophthalmic emergency requiring prompt blood pressure control.
Scheie classification:
Independently evaluates hypertensive changes (H classification) and arteriosclerotic changes (S classification)4)
A two-axis classification of H0–H4 / S0–S4, allowing separate assessment of hypertensive and arteriosclerotic changes
Wong-Mitchell simplified classification:
Three stages: mild, moderate, malignant5)
Moderate or higher stages are associated with significantly increased risk of stroke and cardiovascular events5)
A large cohort study (ARIC Study) showed that moderate or greater retinal arteriolar narrowing is an independent predictor of coronary artery disease5)
Arteriovenous ratio (AVR):
Normal retinal arteriovenous ratio (AVR) is approximately 0.675)
Decreased AVR (narrowing of arteriolar diameter) is a quantitative indicator of hypertension and arteriosclerosis and correlates with cardiovascular risk5)
Arteriosclerotic fundus changes:
Copper-wire artery: widening of the light reflex due to hyaline degeneration of the arterial wall
Silver-wire artery: loss of the blood column reflex due to fibrous thickening of the arterial wall (indicating severe arteriosclerosis)
Hollenhorst plaque: cholesterol emboli dislodged from atheroma of the carotid artery or aorta, impacted in a retinal artery branch
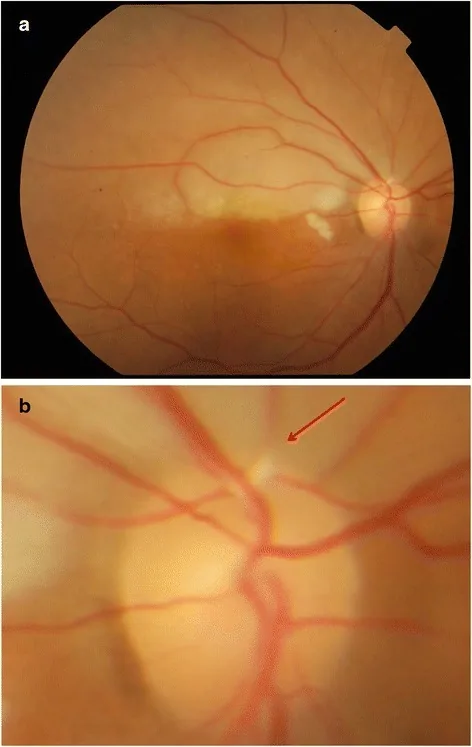
Yong MH, Mustapha M, Che Hamzah J, et al. Right eye findings showing pale retina and Hollenhorst plaque. 2023. Figure 1. Source ID: Wikimedia Commons (File:Right_eye_findings,_Pale_Retina_and_Hollenhorst_plaque.png). License: CC BY 4.0.
Superior retinal pallor (a) and a cholesterol embolus (Hollenhorst plaque, arrow) impacted at the superior temporal vascular arcade (b) are observed. This corresponds to the Hollenhorst plaque discussed in section “3. Dyslipidemia and Ocular Diseases.”
Dyslipidemia increases the risk of many ocular diseases by promoting arteriosclerosis and also causes characteristic ocular findings.
Arteriosclerotic fundus changes (lipid-related):
Hollenhorst plaque: cholesterol emboli dislodged from atheroma of the carotid artery or aorta, impacted in a retinal artery. Upon detection, carotid ultrasound and echocardiography are mandatory, and collaboration with neurology and cardiology is necessary for stroke prevention.
The presence of cholesterol plaques is often asymptomatic but indicates a risk of cerebral embolism.
Characteristic ocular findings of dyslipidemia:
Arcus senilis: lipid deposition in the peripheral cornea. Appearance before age 50 is considered a sign of dyslipidemia6)
Xanthelasma: lipid deposition (yellow plaque-like lesions) on the eyelid skin. Associated with elevated LDL cholesterol6)
Lipemia retinalis: a rare finding where retinal vessels become milky white due to hypertriglyceridemia (TG > 2,000 mg/dL)7)
Yong KC, Tan AK, Yeap TG, et al. Branch retinal vein occlusion color fundus photograph. 2012. Figure 1. Source ID: Wikimedia Commons (File:Branch_retinal_vein_occlusion.jpg). License: CC BY 2.0.
Left eye fundus image showing fan-shaped intraretinal hemorrhages and hard exudates in the corresponding area due to occlusion of the superior temporal retinal vein. This corresponds to retinal vein occlusion discussed in section “4. Related eye diseases.”
Hypertension and dyslipidemia are directly associated with several major eye diseases.
Retinal vein occlusion (RVO)
Hypertension is the most important risk factor for CRVO: OR 3.0–5.02)
Pathogenesis of BRVO: Hypertension-induced arterial wall thickening compresses the vein at the arteriovenous crossing, causing occlusion2)
Treatment for macular edema: Anti-VEGF therapy (e.g., ranibizumab) is effective10)
Basic management: Medical management of hypertension and dyslipidemia is the most important measure for preventing recurrence
Retinal artery occlusion (RAO)
Retinal stroke: Emergency evaluation similar to stroke is required3)
Cerebral infarction complication: Approximately 30% of CRAO patients and 25% of BRAO patients have concurrent cerebral infarction within one week
Risk factors: Hypertension, diabetes, and dyslipidemia are major risk factors 8)
Role of nocturnal blood pressure dip: Nocturnal dipping (excessive drop in nighttime blood pressure) contributes to optic nerve blood flow impairment in the pathogenesis 8)
Management: Consider adjusting the timing of antihypertensive medication (e.g., avoid taking before bedtime)
Hypertensive Choroidopathy
Choroidal ischemia in malignant hypertension: Caused by fibrinoid necrosis of choroidal vessels 9)
Pregnancy-induced hypertension can also cause similar pathology
Characteristic findings: Elschnig spots (depigmented spots due to RPE damage) and Siegrist streaks (linear pigmentation) 9)
Urgency: Prompt blood pressure control is necessary, similar to KWB classification grade IV
QCan fundus examination detect arteriosclerosis?
A
The fundus is the only site in the body where blood vessels can be directly observed. The degree of arteriosclerosis can be assessed by findings such as copper-wire arteries, silver-wire arteries, arteriovenous crossing phenomena (Gunn sign, Salus sign), and arteriovenous ratio (AVR), which serve as indicators of cardiovascular risk. If Hollenhorst plaques (cholesterol emboli) are found in the fundus, it may indicate the presence of carotid atherosclerosis, and internal medicine evaluation is necessary from the perspective of stroke risk.
Management of ocular diseases associated with hypertension and dyslipidemia is based on a combination of ophthalmic treatment and systemic medical management.
Ophthalmic examination:
Dilated fundus examination (ophthalmoscope, fundus camera): evaluation using KWB classification and Scheie classification
Fluorescein angiography (FA): assessment of retinal circulation and identification of vascular occlusion sites
OCT: evaluation of macular edema and inner retinal layer damage
Fundus photography: documentation and follow-up
Systemic evaluation (in collaboration with internal medicine):
Acute CRAO: t-PA thrombolytic therapy (within 4.5 hours of onset) is considered effective but is not covered by insurance, so facility-specific management is required
NAION: if nocturnal hypotension is suspected, discuss adjustment of antihypertensive medication timing with internal medicine
Medical management:
Antihypertensives: ARBs (angiotensin II receptor blockers) and ACE inhibitors have vascular protective effects 11)
Statins: Lowering LDL-C suppresses progression of atherosclerosis. Meta-analyses have shown a weak protective effect on AMD risk 12)
QWhat should be done if an abnormality is pointed out on a health checkup fundus examination?
A
Hypertensive retinopathy is an indicator of cardiovascular risk. Findings of KWB grade II or higher and Scheie grade H2 or higher indicate that arteriosclerotic changes have reached an organic stage. In addition to detailed ophthalmologic examination (dilated fundus exam, OCT), evaluation of blood pressure, lipids, and blood glucose by internal medicine is recommended. If a Hollenhorst plaque (bright yellow plaque) is noted, evaluation for carotid artery disease is particularly important, and the patient should promptly see an internist or neurologist.
6. Pathophysiology and detailed mechanisms of onset
The mechanisms by which hypertension and dyslipidemia damage ocular tissues are broadly divided into three categories: structural changes in the vessel wall, blood flow disturbance, and embolic mechanisms.
Progressive stages of retinal arteriolar changes due to hypertension:
Phase 1 (vasoconstrictive phase): Arterioles constrict as a functional response to hypertension. Irregularity of caliber and increased light reflex (KWB grade I) occur 1)
Phase 2 (arteriosclerotic phase): Persistent hypertension causes organic thickening of the vessel wall. At arteriovenous crossings where the arterial and venous walls share a common adventitia, the vein is compressed and narrowed (KWB grade II) 2)
Phase 3 (exudative phase): Flame-shaped hemorrhages, cotton-wool spots, and hard exudates due to increased vascular permeability and rupture (KWB grade III) 1)
Phase 4 (malignant hypertension phase): Fibrinoid necrosis of choroidal vessels and papilledema (KWB grade IV) 9)
Mechanism of arteriovenous crossing changes (KWB grade II):
Retinal arterioles and venules share a common adventitia at crossing sites 2)
Hypertension-induced arterial wall thickening compresses the venule via the common adventitia, causing narrowing (Gunn sign)
Severe compression can displace the venular course (Salus sign)
This narrowing at the arteriovenous crossing increases the risk of venous thrombosis, directly leading to BRVO
Mechanism of cholesterol emboli (Hollenhorst plaques):
Micro-cholesterol crystals dislodge from atherosclerotic plaques in the carotid artery or aortic arch 3)
They travel via the bloodstream into the ophthalmic artery, central retinal artery, and branch arteries, becoming impacted at bifurcations
Observed in the fundus as shiny yellow-orange plaques
They often do not completely occlude the artery, but indicate the presence of an embolic source (carotid artery) and signify stroke risk
AI-based prediction of cardiovascular risk from fundus photographs:
Estimation of cardiovascular risk factors (age, sex, smoking history, systolic blood pressure, etc.) from fundus photographs using deep learning models has been reported 13).
Google research has shown that major cardiovascular event risk can be predicted from fundus photographs 13).
Application to teleophthalmology, using the fundus as a cardiovascular screening tool, is expected.
Prospective studies on retinal vascular parameters and cardiovascular risk:
The association between quantitative assessment of AVR (arteriovenous ratio), retinal arteriolar diameter, and venular diameter with cardiovascular events is being studied in large prospective cohorts 5).
The ARIC Study (Atherosclerosis Risk in Communities Study) showed that retinal arteriolar narrowing is an independent predictor of coronary artery disease5)
Quantitative assessment of retinal microcirculation using OCTA:
Research is investigating whether quantitative assessment of retinal capillary density and avascular area using optical coherence tomography angiography (OCTA) may be useful for early detection of hypertensive retinal changes
It has been reported that capillary density in the superficial and deep layers is reduced in hypertensive patients
Statins and retinal protective effects:
The association between statin use and risk of developing AMD has been examined in meta-analyses, suggesting a weak protective effect12)
Prospective studies on the effect of statins on RVO risk are also ongoing
Basic research has shown direct retinal vascular protective effects (pleiotropic effects) of statins, but clinical significance has not been established
Tien Y. Wong, Paul Mitchell. Hypertensive Retinopathy. N Engl J Med. 2004;351(22):2310-2317. doi:10.1056/nejmra032865.
Hayreh SS, Zimmerman MB, Podhajsky P. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. American journal of ophthalmology. 1994;117(4):429-41. doi:10.1016/s0002-9394(14)70001-7. PMID:8154523.
Mac Grory B, Schrag M, Biousse V, Furie KL, Gerhard-Herman M, Lavin PJ, Sobrin L, Tjoumakaris SI, Weyand CM, Yaghi S, American Heart Association Stroke Council; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Hypertension; and Council on Peripheral Vascular Disease. Management of Central Retinal Artery Occlusion: A Scientific Statement From the American Heart Association. Stroke. 2021;52(6):e282-e294. doi:10.1161/str.0000000000000366. PMID:33677974.
SCHEIE HG. Evaluation of ophthalmoscopic changes of hypertension and arteriolar sclerosis. A.M.A. archives of ophthalmology. 1953;49(2):117-38. doi:10.1001/archopht.1953.00920020122001. PMID:13007237.
Wong TY, Klein R, Sharrett AR, et al. Retinal arteriolar narrowing and risk of coronary heart disease in men and women. The Atherosclerosis Risk in Communities Study. JAMA. 2002;287(9):1153-1159. doi:10.1001/jama.287.9.1153.
Zech LA Jr, Hoeg JM. Correlating corneal arcus with atherosclerosis in familial hypercholesterolemia. Lipids in health and disease. 2008;7:7. doi:10.1186/1476-511X-7-7. PMID:18331643; PMCID:PMC2279133.
Vinger PF, Sachs BA. Ocular manifestations of hyperlipoproteinemia. American journal of ophthalmology. 1970;70(4):563-73. doi:10.1016/0002-9394(70)90890-1. PMID:5505473.
Hayreh SS. Management of ischemic optic neuropathies. Indian J Ophthalmol. 2011;59(2):123-136. PMID: 21350282. PMCID: PMC3116541. doi:10.4103/0301-4738.77024.
Campochiaro PA, Heier JS, Feiner L, Gray S, Saroj N, Rundle AC, et al. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1102-1112.e1. doi:10.1016/j.ophtha.2010.02.021.
O’Brien T, Nguyen TT, Zimmermann MB. Hyperlipidemia and diabetes mellitus. Mayo Clin Proc. 1998;73(10):969-976. doi:10.4065/73.10.969.
Ma L, Wang Y, Du J, et al. The association between statin use and risk of age-related macular degeneration. Sci Rep. 2015;5:18280. doi:10.1038/srep18280.
Poplin R, Varadarajan AV, Blumer K, Liu Y, McConnell MV, Corrado GS, et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nature biomedical engineering. 2018;2(3):158-164. doi:10.1038/s41551-018-0195-0. PMID:31015713.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.