Metabolic syndrome is a metabolic disorder characterized by visceral fat obesity (abdominal obesity) combined with hyperglycemia, hypertension, and dyslipidemia. Each component independently increases the risk of eye diseases, and epidemiological studies have confirmed that their accumulation synergistically increases the risk 1).
The prevalence in adults is estimated to be approximately 20–25% 2), and epidemiological studies have accumulated evidence linking it to eye diseases. Visceral fat obesity and insulin resistance serve as common pathological bases, and their involvement has been clarified in a wide range of eye diseases, including diabetic retinopathy, age-related macular degeneration, retinal vein occlusion, glaucoma, central serous chorioretinopathy, and dry eye1).
Lifestyle improvements (dietary therapy and exercise therapy) contribute to better ophthalmic outcomes through the improvement of metabolic syndrome. It is important for ophthalmologists to understand the relationship between systemic metabolic diseases and the risk of eye diseases and to collaborate with internists.
QDoes metabolic syndrome affect the eyes?
A
When hyperglycemia, hypertension, and dyslipidemia accumulate, the risk of eye diseases such as diabetic retinopathy, age-related macular degeneration, retinal vein occlusion, glaucoma, central serous chorioretinopathy, and dry eye increases synergistically 1). Each component alone increases the risk of eye diseases, but when multiple factors overlap, the risk further increases. Undergoing ophthalmic examinations even in the asymptomatic stage leads to early detection.
The diagnosis of metabolic syndrome requires waist circumference, an indicator of visceral fat accumulation, as an essential item, and is made by confirming the presence of other metabolic abnormalities.
The joint interim statement of the International Diabetes Federation (IDF) and the American Heart Association (AHA)/National Heart, Lung, and Blood Institute (NHLBI) (Alberti 2009) sets ethnic-specific cutoffs for waist circumference while establishing common metabolic abnormality criteria4).
Diagnostic Criteria
Waist Circumference
Blood Pressure
Blood Glucose
Lipids
Japanese criteria (2005)
Men ≥ 85 cm, women ≥ 90 cm3)
≥ 130/85 mmHg3)
≥ 110 mg/dL3)
TG ≥ 150 mg/dL3)
IDF/AHA joint (2009)
Ethnic-specific cutoffs (Japanese: men ≥ 85 cm, women ≥ 90 cm)4)
≥ 130/85 mmHg4)
≥ 100 mg/dL4)
TG ≥ 150 mg/dL4)
The main difference between the two criteria is the cutoff value for fasting blood glucose (Japanese criteria ≥ 110 mg/dL, IDF/AHA criteria ≥ 100 mg/dL). In ophthalmology practice, it is desirable to know which criteria were used for the patient’s diagnosis.
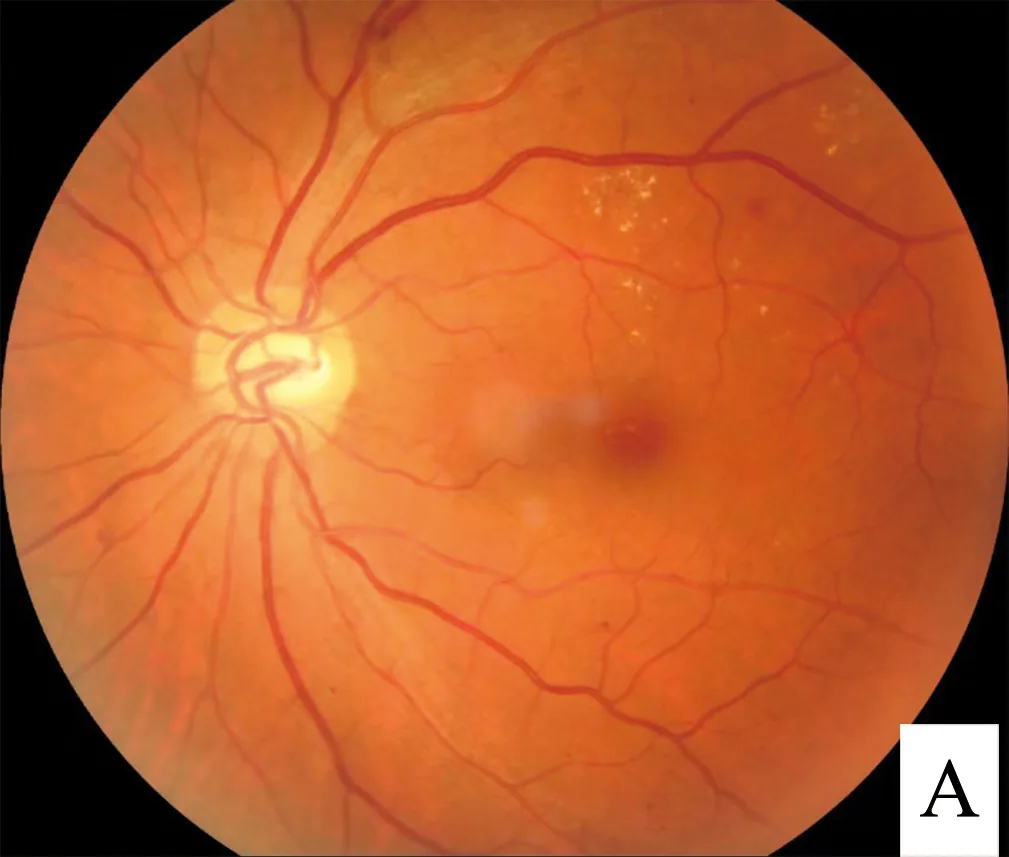
Hao S, Liu C, Li N, et al. A deep learning model for detection of diabetic retinopathy. PLoS One. 2022. Figure 1. Source ID: Wikimedia Commons / Fundus_-_diabetic_retinopathy.png. License: CC BY 4.0.
The fundus photograph shows typical findings of diabetic retinopathy: hard exudates (scattered yellowish-white spots), microaneurysms (bulging of vessel walls), and dot hemorrhages (blurred red dots). This corresponds to diabetic retinopathy (DR) discussed in the section “3. Related eye diseases.”
The components of metabolic syndrome are involved in multiple eye diseases through different mechanisms.
Diabetic Retinopathy (DR)
The most direct ocular complication.
It develops via the pathway: insulin resistance → hyperglycemia → retinal microvascular damage5). The UKPDS (United Kingdom Prospective Diabetes Study) showed that a 1% reduction in HbA1c decreases the risk of microvascular complications by 37%5). The prevalence of DR increases with the number of metabolic syndrome components.
Age-Related Macular Degeneration (AMD)
Obesity and hypertension are major risk factors.
Abdominal obesity (BMI ≥ 30) is associated with an AMD risk odds ratio of 1.3–2.06), with particular attention to visceral fat obesity. Hypertension and dyslipidemia have also been shown to promote AMD progression7). Having three or more metabolic syndrome components yields an odds ratio of 1.76).
Retinal Vein Occlusion (RVO)
Mechanism: vascular compression due to arteriosclerosis.
Arteriosclerosis caused by hypertension and dyslipidemia leads to venous compression at arteriovenous crossings. A nationwide cohort study showed an increased risk of RVO in individuals with metabolic syndrome8).
Glaucoma
Obesity and insulin resistance affect intraocular pressure.
Regarding the association between obesity and open-angle glaucoma (OAG), a 5-unit increase in BMI is associated with a 0.3–0.7 mmHg rise in intraocular pressure9). A proposed mechanism is insulin resistance → sympathetic nervous system activation → increased aqueous humor production9).
Central Serous Chorioretinopathy (CSC)
Association with cortisol and BMI.
Hypertension and steroid exposure have been reported as risk factors for CSC10). Stress-related endocrine changes and increased choroidal vascular permeability are also involved in the pathogenesis.
An association between metabolic syndrome and meibomian gland dysfunction (MGD) has been shown11), and an epidemiological correlation between dyslipidemia and MGD has been reported. The possibility of lacrimal gland dysfunction due to insulin resistance has also been suggested11).
QWhat eye diseases does metabolic syndrome increase the risk for?
A
The six main associated eye diseases are diabetic retinopathy, age-related macular degeneration (AMD), retinal vein occlusion (RVO), glaucoma, central serous chorioretinopathy (CSC), and dry eye. Each component (hyperglycemia, hypertension, dyslipidemia, obesity) independently increases the risk of eye disease, and the accumulation of multiple components synergistically increases the risk1). In particular, diabetic retinopathy is the most direct ocular complication of metabolic syndrome, and HbA1c management is directly linked to visual prognosis5).
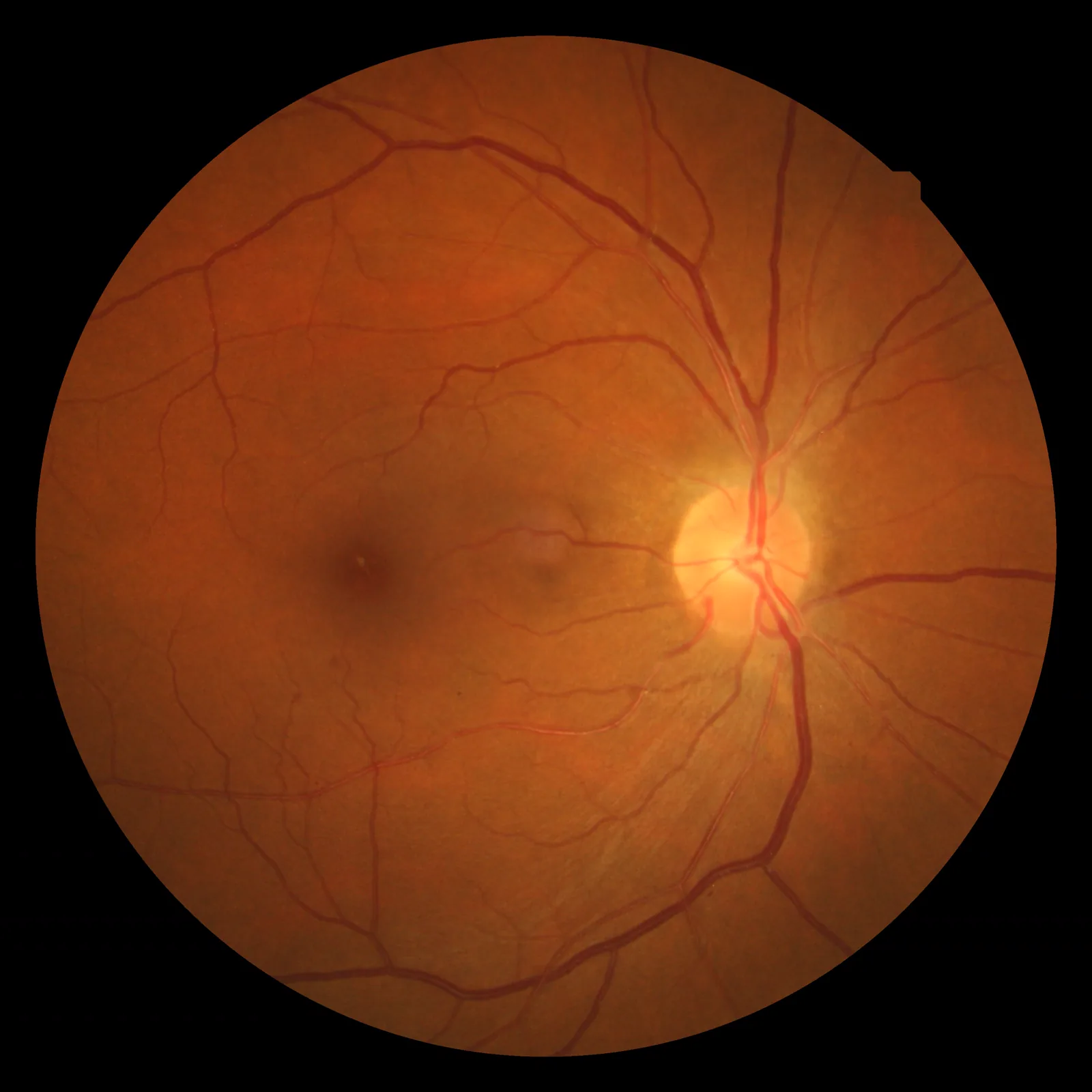
Wood F. Hypertensive retinopathy fundus photograph. 2009. Figure 1. Source ID: Wikimedia Commons / Hypertensiveretinopathy.jpg. License: CC BY 3.0.
The fundus photograph shows arteriovenous crossing phenomenon, flame-shaped hemorrhages, and cotton-wool spots, which are characteristic of hypertensive retinopathy. This corresponds to hypertension, metabolic syndrome, and retinal vascular disorders (hypertensive retinopathy, RVO) discussed in the section “4. Epidemiological Data.”
Epidemiological data showing the association between metabolic syndrome and various eye diseases are summarized below.
The prevalence of metabolic syndrome is estimated to be approximately 20–25% in adults2)
The prevalence of DR increases with the number of MetS components5)
With three or more MetS components, the odds ratio for AMD risk is 1.76)
MetS is associated with an increased risk of RVO (adjusted HR 1.46)8)
Intraocular pressure increases by 0.3–0.7 mmHg per 5-unit increase in BMI9)
Exercise intervention has been reported to lower intraocular pressure, but there are differences between studies in effect size and sustainability12)
Weight management can contribute to reducing the risk of eye diseases through control of blood glucose, blood pressure, and lipids2)
Regarding the relationship between obesity and intraocular pressure, a large-scale epidemiological study in Japan (Mori 2000) confirmed a positive correlation between BMI and intraocular pressure9), indicating that weight reduction is also important for intraocular pressure management.
Lifestyle modification centered on dietary therapy and exercise therapy forms the foundation of managing metabolic syndrome as a whole 2).
Dietary therapy: Calorie restriction, salt reduction, and lipid management. A 3–5% weight loss improves metabolic parameters 2)
Exercise therapy: Aim for moderate aerobic exercise ≥ 150 minutes per week 2)
Exercise and intraocular pressure: Exercise intervention has been reported to lower intraocular pressure, but there are differences among studies regarding effect size, exercise modality, and sustainability 12)
Weight management: Weight loss improves blood glucose, blood pressure, and lipids, and also contributes to managing the risk of ophthalmic complications 2)
Alongside standard treatment for each ocular complication, it is important to establish a collaborative system with internal medicine.
Patients with diabetes should undergo fundus examination at least once a year
Rapid improvement in HbA1c (e.g., upon insulin initiation) requires caution for temporary worsening of retinopathy (early worsening)
In patients suspected of glaucoma, weight management and intraocular pressure monitoring should be coordinated
In patients with AMD or RVO, intensified blood pressure and lipid management contributes to improved ophthalmologic prognosis
QDoes improving metabolic syndrome reduce the risk of eye diseases?
A
Weight loss, exercise, and management of blood glucose, blood pressure, and lipids are expected to reduce the risk of various eye diseases. In particular, for diabetic retinopathy, a 1% reduction in HbA1c decreases the risk of progression by 37% 5). Exercise interventions have been reported to lower intraocular pressure, but the effect size varies among studies 12). Fenofibrate has evidence of suppressing DR progression and reducing the need for photocoagulation14).
Insulin resistance is a common pathological basis of metabolic syndrome 1). Hyperinsulinemia leads to increased sympathetic nervous system activity, which in turn promotes VEGF production and increases aqueous humor production. This contributes to the risk of both diabetic retinopathy and glaucoma1).
Visceral fat secretes inflammatory cytokines such as TNF-α, IL-6, and MCP-1 1). Systemic chronic inflammation causes vascular endothelial dysfunction, leading to increased permeability of retinal and choroidal vessels. Chronic inflammation is also involved in the progression to the exudative form of AMD.
The combination of hyperglycemia and dyslipidemia increases the production of reactive oxygen species (ROS) 7). ROS damage retinal pigment epithelium (RPE) cells and are involved in the onset and progression of AMD. Activation of the polyol pathway and accumulation of advanced glycation end products (AGEs) also amplify oxidative stress5).
Visceral fat accumulation leads to increased leptin and decreased adiponectin 15). These adipokine abnormalities may contribute to the risk of eye diseases through inflammation, vascular function, and retinal metabolism 15).
Accumulation of Advanced Glycation End Products (AGEs)
Persistent hyperglycemia leads to accumulation of AGEs in retinal vessel walls 5). This causes structural changes in the basement membrane and increased vascular permeability, leading to the formation of microaneurysms and retinal edema.
In CSC, stress-related endocrine changes, steroid exposure, and increased choroidal vascular permeability are involved in the pathology 10). Systemic factors such as hypertension should be identified and modifiable factors should be addressed.
Research is progressing on detecting the presence of metabolic syndrome from fundus photographs using AI-based fundus image analysis 1). The relationship between retinal vascular morphology analysis (vessel diameter, fractal analysis, etc.) and metabolic parameters has been demonstrated, and fundus photography is attracting attention as a potential screening tool for systemic metabolic risk.
With the widespread use of GLP-1 receptor agonists (e.g., semaglutide) and SGLT2 inhibitors (e.g., empagliflozin), research on ophthalmic safety and protective effects is accumulating 13). Semaglutide has been reported to be associated with early worsening in some trials, and ophthalmic monitoring is important when used in patients with a history of DR. For SGLT2 inhibitors, clear evidence of increased ophthalmic risk is currently limited 13).
Adipokines such as adiponectin are being studied for their association with retinal vascular diseases, AMD, and glaucoma15). At present, they are in the exploratory stage as therapeutic targets, and additional validation is needed for clinical application.
Research on changes in eye disease risk associated with weight loss and improved insulin resistance is accumulating. To link exercise intervention and weight management to ophthalmic outcomes, evidence from future large-scale studies is needed 12).
It is becoming clear that the composition of the gut microbiota affects insulin resistance and chronic inflammation. Research on the role of gut microbiota in the relationship between metabolic syndrome and eye diseases is just beginning, and further accumulation of knowledge is awaited.
Risk stratification for metabolic syndrome-related eye diseases based on genetic polymorphisms is being studied. The interaction between AMD-related genes (CFH, ARMS2, etc.) and obesity/metabolic abnormalities is attracting attention, and personalized preventive interventions and screening frequencies considering genetic background are future goals.
Wong TY, Klein R, Klein BE, Tielsch JM, Hubbard L, Nieto FJ. Retinal microvascular abnormalities and their relationship with hypertension, cardiovascular disease, and mortality. Survey of ophthalmology. 2001;46(1):59-80. doi:10.1016/s0039-6257(01)00234-x. PMID:11525792.
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735-52. doi:10.1161/CIRCULATIONAHA.105.169404. PMID:16157765.
Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640-1645. PMID:19805654. doi:10.1161/CIRCULATIONAHA.109.192644.
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). The Lancet. 1998;352(9131):837-853. doi:10.1016/s0140-6736(98)07019-6.
Adams MK, Simpson JA, Aung KZ, Makeyeva GA, Giles GG, English DR, et al. Abdominal obesity and age-related macular degeneration. American journal of epidemiology. 2011;173(11):1246-55. doi:10.1093/aje/kwr005. PMID:21422060.
Usha Chakravarthy, Tien Y Wong, Astrid Fletcher, Elisabeth Piault, Christopher Evans, Gergana Zlateva, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10(1). doi:10.1186/1471-2415-10-31.
Lim DH, Shin KY, Han K, et al. Differential effect of the metabolic syndrome on the incidence of retinal vein occlusion in the Korean population: a nationwide cohort study. Transl Vis Sci Technol. 2020;9(13):15. PMID: 33344059. PMCID: PMC7726586. doi:10.1167/tvst.9.13.15.
Mori K, Ando F, Nomura H, Sato Y, Shimokata H. Relationship between intraocular pressure and obesity in Japan. International journal of epidemiology. 2000;29(4):661-6. doi:10.1093/ije/29.4.661. PMID:10922342.
Nicholson B, Noble J, Forooghian F, Meyerle C. Central serous chorioretinopathy: update on pathophysiology and treatment. Surv Ophthalmol. 2013;58(2):103-126. PMID: 23410821. PMCID: PMC3574296. doi:10.1016/j.survophthal.2012.07.004.
Braich PS, Howard MK, Singh JS. Dyslipidemia and its association with meibomian gland dysfunction. Int Ophthalmol. 2016;36(4):469-476. doi:10.1007/s10792-015-0149-4.
González-Devesa D, Suárez-Iglesias D, Diz JC, Esmerode-Iglesias A, Ayán C. Systematic review on the impact of exercise on intraocular pressure in glaucoma patients. Int Ophthalmol. 2024;44:298. PMID: 39160282. PMCID: PMC11333518. doi:10.1007/s10792-024-03216-4.
Vilsbøll T, Christensen M, Junker AE, Knop FK, Gluud LL. Effects of glucagon-like peptide-1 receptor agonists on weight loss: systematic review and meta-analyses of randomised controlled trials. BMJ (Clinical research ed.). 2012;344:d7771. doi:10.1136/bmj.d7771. PMID:22236411; PMCID:PMC3256253.
Keech AC, Mitchell P, Summanen PA, O’Day J, Davis TM, Moffitt MS, et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): a randomised controlled trial. Lancet (London, England). 2007;370(9600):1687-97. doi:10.1016/S0140-6736(07)61607-9. PMID:17988728.
Almpanidou S, Vachliotis ID, Goulas A, Polyzos SA. The potential role of adipokines and hepatokines in age-related ocular diseases. Metabol Open. 2025;26:100365. PMID: 40330313. PMCID: PMC12053655. doi:10.1016/j.metop.2025.100365.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.