
Possible Causes of Distorted or Missing Vision
Key Points at a Glance
Section titled “Key Points at a Glance”1. What Does It Mean When Vision Is Distorted or Missing?
Section titled “1. What Does It Mean When Vision Is Distorted or Missing?”Symptoms such as “things look distorted,” “straight lines appear curved,” or “part of the visual field is missing or dark” can arise from various causes including macular diseases, retinal diseases, glaucoma, optic nerve diseases, and brain diseases. These symptoms are broadly classified into two pathologies.
Metamorphopsia is a symptom in which the shape, size, or straight lines of objects appear distorted. The main cause is structural changes in the macula (the central part of the retina), typically causing grids or straight lines to appear wavy.
Visual field defect is a symptom in which part of the visual field becomes invisible (feels dark or missing). It is caused by a wide range of diseases including glaucoma, retinal detachment, retinal vascular occlusion, optic nerve diseases, and brain diseases.
The prevalence of age-related macular degeneration (AMD) in the Hisayama study was reported as 1.6% for advanced stages (exudative type 1.5%, atrophic type 0.1%), and precursor lesions were found in 22.8% of participants in the Nagahama study. AMD is more common in people aged 50 and older and in men (male:female = 3:1), with bilateral involvement in 40% of cases. Meanwhile, the prevalence of glaucoma is about 5% in people aged 40 and older 1), making it one of the major causes of visual impairment in Japan.
Accurately understanding the type and onset pattern of symptoms and visiting an ophthalmologist at the appropriate time are key to protecting vision. The habit of checking each eye separately leads to early detection.
2. Diseases Causing Metamorphopsia (Distortion)
Section titled “2. Diseases Causing Metamorphopsia (Distortion)”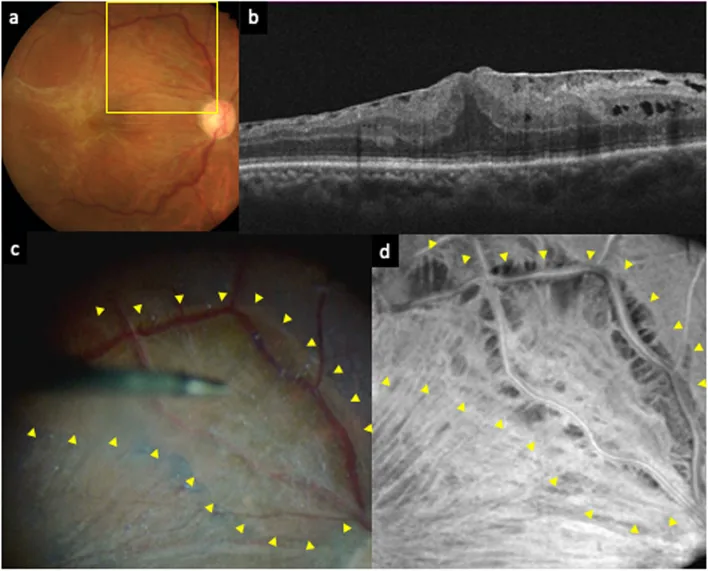
Metamorphopsia is often caused by structural changes in the macula (the central part of the eye). Typical symptoms include straight lines or grids appearing wavy, and the central vision becoming dark (central scotoma).
| Disease | Typical Age/Sex | Main Features | Urgency |
|---|---|---|---|
| Epiretinal Membrane | Middle-aged and elderly | Metamorphopsia, macropsia. Gass classification Grade 0–2. Diagnosed by OCT. | Low to moderate (observation → surgery) |
| Age-related Macular Degeneration (AMD) | 50 years or older, male predominance | Initial symptoms: metamorphopsia and central scotoma. Progression leads to visual acuity ≤ 0.1. | Moderate to high (early treatment is important) |
| Macular hole | Middle-aged and older women | Full-thickness foveal defect → central scotoma and metamorphopsia | Moderate (surgery indicated) |
| Central serous chorioretinopathy (CSC) | Young to middle-aged men | Triggered by stress or steroid use. Micropsia also present 2) | Low to moderate (often resolves spontaneously) |
| Diabetic macular edema (DME) | Patients with diabetes | Metamorphopsia and vision loss due to macular edema 3) | Moderate to high (treatment prevents worsening) |
Details of epiretinal membrane (macular pucker)
Section titled “Details of epiretinal membrane (macular pucker)”Epiretinal membrane occurs when retinal glial cells proliferate on the internal limiting membrane and form fibrous tissue in idiopathic cases. Secondary cases may follow inflammation, retinal detachment, trauma, or retinal vascular tumors. Symptoms include decreased vision and metamorphopsia, sometimes with macropsia. Gass classification ranges from Grade 0 (cellophane maculopathy: transparent, no retinal distortion) to Grade 2 (gray, opaque membrane with marked wrinkling). OCT examination confirming the epiretinal membrane and increased retinal thickness provides the basis for definitive diagnosis. Vitrectomy with epiretinal membrane peeling is indicated when there is visual impairment, marked retinal thickening, or severe metamorphopsia. Postoperative visual acuity correlates well with preoperative acuity, and recovery may take a long time (over one year).
Classification of age-related macular degeneration (AMD)
Section titled “Classification of age-related macular degeneration (AMD)”AMD progresses from precursor lesions (soft drusen, retinal pigment epithelium abnormalities) and is classified into atrophic (geographic atrophy) and exudative (choroidal neovascularization: CNV) types. Among exudative types, polypoidal choroidal vasculopathy (PCV) is a special subtype common in Japanese individuals. Exudative AMD begins with metamorphopsia and central scotoma, and if left untreated, approximately 90% of cases progress to visual acuity of 0.1 or worse. In cases of massive hemorrhage, sudden severe vision loss may occur.
If the grid lines of the Amsler chart appear distorted, partially missing, or if you perceive a scotoma, it may be a sign of macular disease. It is recommended to see an ophthalmologist within a few days and undergo OCT (optical coherence tomography) examination. Especially if abnormalities are found when checking each eye separately, priority is high. The detection sensitivity of the Amsler chart for AMD within the central 5 degrees is reported to be approximately 70% 8), and regular examinations are important even without subjective symptoms.
3. Diseases Causing Visual Field Defects (Missing Areas)
Section titled “3. Diseases Causing Visual Field Defects (Missing Areas)”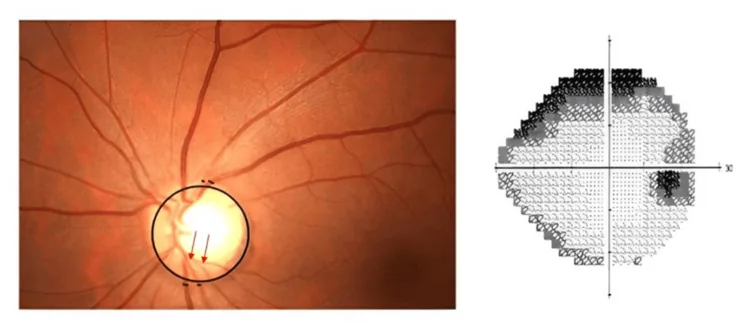
Visual field defects manifest as symptoms such as parts of the visual field appearing dark, missing, or as if a curtain is drawn. Causes range from slowly progressive conditions like glaucoma to sudden-onset emergencies such as retinal detachment and retinal artery occlusion.
| Disease | Visual Field Defect Pattern | Urgency |
|---|---|---|
| Glaucoma | Arcuate scotoma, paracentral scotoma. Central vision is preserved until the end stage 1) | Low to moderate (chronic progressive; regular management required) |
| Retinal Detachment (Rhegmatogenous) | Curtain-like or drape-like visual field defect. Spreads from one side. | Emergency (may require same-day surgery) |
| Retinal vein occlusion (branch type) | Sector-shaped visual field defect (corresponding to the occluded vein area) 4) | Moderate to high (early treatment affects prognosis) |
| Retinal artery occlusion | Sudden painless vision loss and extensive visual field defect 5) | Emergency (the first few hours after onset are critical) |
| Bilateral visual field defect | Hemianopia with a vertical border (homonymous hemianopia) → Suspect brain disease 6) | Emergency (coordination with neurology/neurosurgery) |
Characteristics of visual field defects in glaucoma
Section titled “Characteristics of visual field defects in glaucoma”In glaucoma, degeneration and loss of optic nerve fibers cause arcuate scotomas and paracentral scotomas in the corresponding visual field. In the early to middle stages, central vision is preserved, so patients are often unaware until significant visual field loss has occurred 1). According to the Tajimi Study, the prevalence of primary open-angle glaucoma is approximately 3.9% in Japanese people aged 40 and older 1), and regular intraocular pressure measurement and fundus examination are essential for early detection.
Visual field defects in retinal detachment
Section titled “Visual field defects in retinal detachment”In rhegmatogenous retinal detachment, as subretinal fluid spreads from a retinal tear, a curtain-like or veil-like visual field defect expands from one side 9). This is often preceded by a sudden increase in photopsia and floaters. When the visual field defect reaches the macula (central area), visual acuity drops significantly, so emergency surgery before that point greatly affects visual prognosis.
Visual field defects due to brain disease
Section titled “Visual field defects due to brain disease”Homonymous hemianopia, where both visual fields are symmetrically missing, indicates a brain lesion in the optic radiation or occipital lobe. It can be caused by cerebral infarction, brain tumor, or intracranial hemorrhage 6), and prompt coordination with neurology and neurosurgery is necessary.
4. Sudden Visual Field Changes (Scintillating Scotoma / Amaurosis Fugax)
Section titled “4. Sudden Visual Field Changes (Scintillating Scotoma / Amaurosis Fugax)”Sudden temporary visual field changes range from migraine-related scintillating scotoma, which resolves spontaneously, to amaurosis fugax requiring urgent evaluation. Key differentiating points include whether it is monocular or binocular, duration, and accompanying symptoms.
| Symptom | Duration | Eye Involvement | Features | Urgency |
|---|---|---|---|---|
| Scintillating scotoma (migraine aura) | Resolves spontaneously in 20–30 minutes | Binocular (homonymous visual field) | Zigzag ring of light, colorful lights that expand | Low (consult migraine clinic) |
| Amaurosis fugax (TIA ocular symptom) | Seconds to minutes | Monocular | One eye becomes completely blind, sensation of a curtain descending from above7) | Emergency (same-day neurology/ophthalmology) |
| Retinal detachment precursor (photopsia) | Recurrent | Unilateral | Flashes or lightning-like lights in dark places. Accompanied by increased floaters. | High (see an ophthalmologist within a few days) |
| Vitreous hemorrhage | Sudden, persistent | Unilateral | Rapid increase in floaters, blurring, vision loss | High (urgent ophthalmology visit) |
Urgency of Bilateral Hemianopia
Section titled “Urgency of Bilateral Hemianopia”If the same half of the visual field is missing in both eyes simultaneously (e.g., the right visual field is missing in both eyes), it is an emergency sign indicating cerebral infarction, brain tumor, or occipital lobe lesion 6). Immediate emergency consultation is required.
5. Self-Check Method (Amsler Grid) and When to See a Doctor
Section titled “5. Self-Check Method (Amsler Grid) and When to See a Doctor”How to Use the Amsler Grid
Section titled “How to Use the Amsler Grid”Self-testing with the Amsler grid is useful for monitoring AMD and macular diseases, with reported sensitivity of about 70% for detecting AMD within the central 5 degrees 8). However, due to its limited sensitivity, regular eye examinations should continue even if the grid shows no abnormalities.
Urgency of Consultation
Section titled “Urgency of Consultation”| Urgency Level | Symptoms | Recommended Action |
|---|---|---|
| Same-day visit (including emergency) | Sudden curtain-like visual field defect / Sudden painless vision loss in one eye / Transient vision loss in one eye / Homonymous hemianopia in both eyes | Visit ophthalmologist or emergency room same day. Possible retinal detachment, RAO, or TIA. |
| Early visit (within a few days) | Distortion or scotoma detected on Amsler grid / Change in vision in one eye / Sudden increase in floaters with photopsia | OCT examination at an ophthalmologist within 1–3 days. |
| Regular visit | Family history of AMD, history in one eye, glaucoma risk factors (high intraocular pressure, family history, high myopia) present1) | Regular eye exams 1–2 times per year. |
In early to moderate glaucoma, central vision remains normal, making it very difficult to notice visual field defects. This is because the other eye and the brain unconsciously compensate for the missing field. Getting into the habit of checking vision by closing one eye and undergoing regular visual field tests at an ophthalmologist are important for early detection. According to the Tajimi Study, approximately 90% of glaucoma patients are undiagnosed1), so regular checkups are recommended for people aged 40 and older even if asymptomatic.
6. Pathophysiology of Distortion and Defects
Section titled “6. Pathophysiology of Distortion and Defects”Mechanism of Metamorphopsia in Macular Diseases
Section titled “Mechanism of Metamorphopsia in Macular Diseases”In epiretinal membrane, retinal glial cells proliferate on the internal limiting membrane, forming fibrous tissue that creates wrinkles on the retinal surface. These wrinkles disrupt the arrangement of photoreceptor cells, causing metamorphopsia and macropsia.
In age-related macular degeneration (AMD), the retinal pigment epithelium (RPE) in the macula is first damaged, leading to drusen formation and RPE abnormalities. In atrophic AMD, it progresses to geographic atrophy (GA) with loss of photoreceptors; in exudative AMD, choroidal neovascularization (CNV) forms, causing bleeding and exudate that damage the macula. This process results in loss of photoreceptor function, leading to metamorphopsia and central scotoma.
Macular hole involves a full-thickness defect of the fovea, resulting in central scotoma and metamorphopsia.
Central serous chorioretinopathy (CSC) involves increased choroidal permeability leading to fluid accumulation under the RPE and neurosensory retina, causing localized elevation of the macula. This elevation changes the focal distance, resulting in metamorphopsia and micropsia2).
Mechanism of visual field defects in glaucoma
Section titled “Mechanism of visual field defects in glaucoma”In glaucoma, optic nerve fibers degenerate and are lost due to mechanisms such as axonal damage at the optic nerve head, mechanical compression from intraocular pressure, and ischemia1). Visual field defects occur in retinal areas corresponding to the lost fibers, typically presenting as arcuate scotomas and paracentral scotomas. Central vision is preserved until the late stages, which is the main reason for delayed self-awareness.
Pathophysiology of retinal detachment
Section titled “Pathophysiology of retinal detachment”In rhegmatogenous retinal detachment, retinal traction associated with posterior vitreous detachment leads to the formation of a retinal tear. Liquefied vitreous enters the subretinal space through the tear, causing the sensory retina to detach from the RPE9). Photoreceptors in the detached retina become ischemic, resulting in corresponding visual field defects. Detachment of the central macula leads to a significant decrease in visual acuity, and recovery becomes difficult after a prolonged course.
7. Latest treatments and research
Section titled “7. Latest treatments and research”Next-generation anti-VEGF drug (faricimab)
Section titled “Next-generation anti-VEGF drug (faricimab)”In the TENAYA/LUCERNE randomized controlled trials by Heier et al. (2022), faricimab, which dually inhibits VEGF-A and Angiopoietin-2 (Ang-2), demonstrated non-inferiority for neovascular AMD with dosing intervals up to 16 weeks10). Extended dosing intervals are expected to reduce patient burden.
Complement inhibitors for atrophic AMD (geographic atrophy)
Section titled “Complement inhibitors for atrophic AMD (geographic atrophy)”The complement C3 inhibitor pegcetacoplan, in a phase 2 trial aimed at slowing the progression of geographic atrophy (GA) in atrophic AMD, showed a reduction in GA area enlargement compared to placebo11). Atrophic AMD has had no effective treatment until now, and this is attracting attention as a new therapeutic option.
Efficacy of internal limiting membrane peeling in epiretinal membrane surgery
Section titled “Efficacy of internal limiting membrane peeling in epiretinal membrane surgery”A systematic review and meta-analysis by Azuma et al. (2017) showed that adding internal limiting membrane (ILM) peeling to epiretinal membrane surgery improves postoperative visual acuity and anatomical outcomes12). A reduction in recurrence risk has also been reported.
Early Detection of AMD Using Home Monitoring Devices
Section titled “Early Detection of AMD Using Home Monitoring Devices”The HOME study (randomized controlled trial) by Chew et al. (2014) showed that a home monitoring device (ForeseeHome) detected progression to exudative AMD earlier than usual care, contributing to improved visual prognosis 13). Daily monitoring by patients themselves using digital technology is expected to become more widespread in the future.
8. References
Section titled “8. References”- Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology. 2004;111(9):1641-8. doi:10.1016/j.ophtha.2004.03.029. PMID:15350316.
- Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82-118.
- 日本糖尿病眼学会. 糖尿病網膜症診療ガイドライン(第1版). 日眼会誌. 2020;124(12):955-981.
- Ehlers JP, Fekrat S. Retinal vein occlusion: beyond the acute event. Surv Ophthalmol. 2011;56(4):281-299.
- Hayreh SS. Acute retinal arterial occlusive disorders. Prog Retin Eye Res. 2011;30(5):359-394.
- Zhang X, Kedar S, Lynn MJ, et al. Homonymous hemianopia in stroke. J Neuroophthalmol. 2006;26(3):180-183.
- Biousse V, Trobe JD. Transient monocular visual loss. Am J Ophthalmol. 2005;140(4):717-721.
- Faes L, Bodmer NS, Bachmann LM, Thiel MA, Schmid MK. Diagnostic accuracy of the Amsler grid and the preferential hyperacuity perimetry in the screening of patients with age-related macular degeneration: systematic review and meta-analysis. Eye (London, England). 2014;28(7):788-96. doi:10.1038/eye.2014.104. PMID:24788016; PMCID:PMC4094801.
- Feltgen N, Walter P. Rhegmatogenous retinal detachment—an ophthalmologic emergency. Deutsches Arzteblatt international. 2014;111(1-2):12-21; quiz 22. doi:10.3238/arztebl.2014.0012. PMID:24565273; PMCID:PMC3948016.
- Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729-740.
- Liao DS, Grossi FV, El Mehdi D, et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized phase 2 trial. Ophthalmology. 2020;127(2):186-195.
- Azuma K, Ueta T, Eguchi S, et al. Effects of internal limiting membrane peeling combined with removal of idiopathic epiretinal membrane: a systematic review of literature and meta-analysis. Retina. 2017;37(10):1813-1819.
- Chew EY, Clemons TE, Bressler SB, et al. Randomized trial of the ForeseeHome monitoring device for early detection of neovascular age-related macular degeneration. The HOME Study. Ophthalmology. 2014;121(2):535-544.