Choroidal neovascularization (CNV) is an abnormal proliferation of blood vessels from the choroid through Bruch’s membrane toward the retina. In recent years, it is also called macular neovascularization (MNV).
OCT angiography (OCTA) is a non-invasive examination that visualizes blood flow using motion contrast from signal changes (decorrelation) between repeated B-scans. Without contrast agents, it can depict fine vascular structures around the choroid and RPE with depth resolution through segmentation. Combining OCT and OCTA allows three-dimensional description of the three types of macular neovascularization at the histological level 8).
QWhat is the principle by which OCTA visualizes blood vessels?
A
The same site is scanned repeatedly in a short time; stationary tissue (retina, choroid) does not change, while areas with blood flow show signal fluctuations. This “decorrelation signal” is imaged as motion contrast. Since no contrast agent is used, patient burden is low, making it suitable for repeated examinations.
Choroidal neovascularization differs in type depending on localization and layer relationship. It is assessed by combining OCT tomographic images and slit-lamp findings.
Type 1 MNV: Remains under the retinal pigment epithelium (RPE). On OCT, it shows RPE irregularity/elevation and medium reflectivity. Fluorescein angiography (FA) shows occult findings.
Type 2 MNV: Penetrates the RPE and extends into the subretinal space. On OCT, it is observed as a medium-reflective mass above the RPE. FA shows classic findings.
Type 3 MNV (retinal angiomatous proliferation, RAP): Neovascularization arises within the retina, often accompanied by punctate intraretinal hemorrhage.
Polypoidal choroidal vasculopathy: Orange-red elevated lesions are seen in the fundus. OCT shows steep RPE elevation and a double layer sign (double structure of RPE and Bruch’s membrane).
High myopia: Stretching and rupture of Bruch’s membrane due to axial elongation trigger choroidal neovascularization. In pseudoxanthoma elasticum (PXE), angioid streaks lead to choroidal neovascularization in over 70% of cases, with bilaterality reaching about 90%5).
Peripapillary exudative hemorrhagic chorioretinopathy (PEHCR): May be associated with choroidal neovascularization, posing challenges in diagnosis and treatment 1).
Sclerochoroidal calcification (SCC): Although rare, cases of choroidal neovascularization complicating SCC lesions have been reported 4).
QCan choroidal neovascularization occur in conditions other than age-related macular degeneration?
A
Choroidal neovascularization occurs in various diseases such as high myopia, PXE, PIC, chronic central serous chorioretinopathy, trauma, uveitis, PEHCR, and SCC. In particular, PXE frequently leads to choroidal neovascularization on a background of angioid streaks, with a tendency for bilaterality and resistance to treatment 5). Identifying the underlying disease is important for determining the treatment strategy.
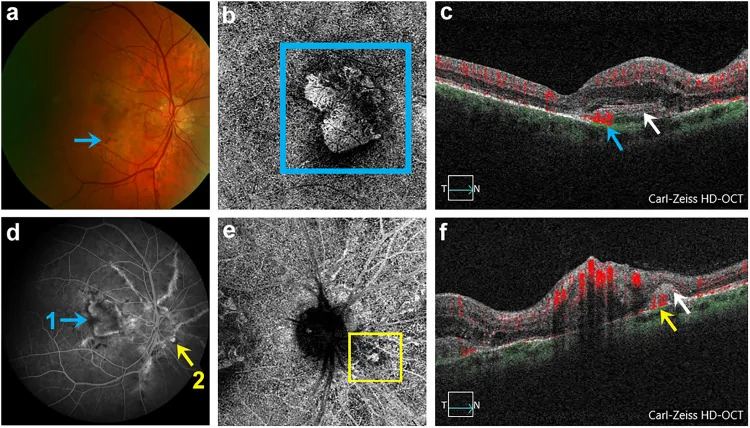
Adnan Kilani; Denise Vogt; Armin Wolf; Efstathios Vounotrypidis. The role of multimodal imaging in characterization and monitoring of choroidal neovascularization secondary to angioid streaks. Eur J Ophthalmol. 2025 Jan 27; 35(1):306-313 Figure 3. PMCID: PMC11697489. License: CC BY.
Right eye with angioid streaks (AS), 2 CNV (macular and juxtapapillary) and Optic nerve head drusen (ONHD) of study patient number 3 (a) Fundus with AS, ONHD, macular CNV and retinal hemorrhage (blue arrow). (b) OCTA of detected macular CNV in outer retina-chorio-capillaris (ORCC) segmentation (blue square). (c) Corresponding B-scan of macular CNV with blood flow registration (blue arrow). (d) FA revealing macular CNV (designated as 1, marked with blue arrow) and juxtapapillary CNV (designated as 2, marked with yellow arrow). (e) SD-OCTA representation of detected juxtapapillary CNV in ORCC segmentation (yellow square). (f) Corresponding B-scan of juxtapapillary CNV with blood flow registration (yellow arrow) and subretinal hyper-reflective material (SHRM) (white arrow).
Multimodal imaging evaluation is essential for the diagnosis of choroidal neovascularization. OCTA plays a central role, but there are situations where it alone is insufficient.
OCTA can be used with either SD-OCT (spectral domain) or SS-OCT (swept source). After imaging, segmentation processing displays blood flow in each retinal layer, around the RPE, and in the choroid as en face images.
OCTA findings by type of choroidal neovascularization
Location: Between the RPE and Bruch’s membrane (sub-RPE).
OCTA morphology: Sea-fan or coral-like vascular network. On en face OCTA, it is visualized in the RPE to choriocapillaris layer 8).
Pachychoroid type 1 macular neovascularization: Shows mature, planar vascular structures with good OCTA visualization. SIRE is a useful biomarker6). Double layer sign can be confirmed on OCT8).
Type 2 Choroidal Neovascularization
Location: Penetrates the RPE and extends into the subretinal space.
OCTA morphology: Visualized as a hyperreflective lesion above the RPE. May show vascular loops or wheel-like patterns.
Corresponding FA findings: Corresponds to classic choroidal neovascularization, showing well-defined hyperfluorescence from the early phase.
OCTA morphology: Abnormal vessels are visualized in the inner retinal layers, with a tendency for particularly clear visualization. Continuous blood flow signal up to the bump sign is characteristic 8).
Clinical features: Often accompanied by punctate intraretinal hemorrhage and small cystoid macular edema, with rapid progression.
OCTA Findings in Polypoidal Choroidal Vasculopathy
Polypoidal choroidal vasculopathy is considered a subtype of type 1 macular neovascularization, consisting of a branching neovascular network (BNN) and polypoidal peripheral lesions.
BNN detection rate: Nearly 100% detectable by OCTA7).
Polyp detection rate: Only about 79% by OCTA7). Factors for non-visualization include increased polyp height, pulsatility, and blockage by subretinal hemorrhage 7).
Morphological classification of BNN: Classified into four types: dead-tree type, coral-bush type, anastomosis type, and pseudopod-like type 7).
Structural classification of BNN (Huang classification): Three types: trunk, glomeruli, and stick 7).
ICGA comparison: OCTA has been reported to have a sensitivity of 97% for detecting pachychoroid macular neovascularization, compared to 66% for ICGA6).
The characteristics of each examination method are shown below.
Even in choroidal neovascularization associated with sclerochoroidal calcification, OCTA can visualize the neovascular network 4). Although rare, imaging confirmation directly determines treatment strategy.
QCan choroidal neovascularization be invisible on OCTA?
A
False negatives can occur due to projection artifacts and segmentation errors. Additionally, the detection rate of polyps in polypoidal choroidal vasculopathy is only about 79% 7), and visualization becomes difficult when there is extensive subretinal hemorrhage. OCTA must always be interpreted in combination with B-scanOCT.
QCan OCTA replace FA or ICGA?
A
OCTA shows sensitivity equal to or greater than ICGA in detecting BNN 6), but FA and ICGA are still useful in some situations for evaluating leakage and confirming polyps. Multimodal imaging is recommended, especially for polypoidal choroidal vasculopathy and assessment of treatment response.
PXE-related choroidal neovascularization: Anti-VEGF provides short-term visual improvement, but injection frequency tends to be higher (mean interval 4.4 months vs. 7.2 months for typical AMD) 5), making long-term management challenging.
SCC-related choroidal neovascularization: Ranibizumab PRN (3–9 injections over 6 years) achieved visual acuity of 20/25 in one report 4).
PEHCR: Anti-VEGF is useful, with a mean of 7.7 injections administered 1).
PDT is considered for vertical polypoidal choroidal vasculopathy (poor vision cases) or anti-VEGF non-responders. Verteporfin is administered intravenously followed by 689 nm laser irradiation.
There are cases that are resistant to standard anti-VEGF therapy, such as PIC-related choroidal neovascularization. A report describes a case that was incomplete with aflibercept but was controlled with 6 doses of faricimab (VEGF-A/Ang-2 dual inhibitor) 6 mg each 3).
QDoes treatment response differ depending on the type of choroidal neovascularization?
A
Anti-VEGF is the basic treatment for all types, but there are differences in response. Type 1 macular neovascularization (including pachychoroid type) is relatively easy to control, while for polypoidal choroidal vasculopathy, combination with PDT is considered depending on visual acuity. Type 3 (RAP) often progresses rapidly and requires intensive treatment. When associated with underlying diseases such as PXE or PIC, it can be even more refractory 5).
The common pathway of choroidal neovascularization is dysfunction of Bruch’s membrane and increased VEGF production.
With aging or genetic predisposition, accumulation of metabolic products (drusen) on Bruch’s membrane impairs substance transport between the RPE and the choriocapillaris. This leads to local hypoxia, and VEGF is produced by the RPE. VEGF promotes migration and proliferation of vascular endothelial cells, initiating the neovascularization cascade.
Choroidal neovascularization due to hereditary diseases has specific mechanisms.
Cowden syndrome (PTEN mutation): Loss of PTEN function leads to constitutive activation of PI3K/Akt/VEGF signaling 5). This may be a molecular mechanism of resistance to anti-VEGF therapy.
PXE (ABCC6 mutation): VEGFA polymorphisms have been shown to be associated with severe retinopathy 5), and genetic background influences the severity of choroidal neovascularization.
In the concept of pachychoroid neovasculopathy, an abnormally thickened choroid compresses and causes ischemia of the choriocapillaris, and chronic oxidative stress to the RPE is thought to be a breeding ground for type 1 macular neovascularization.
7. Latest Research and Future Prospects (Investigational Reports)
Research is ongoing to improve the detection accuracy and reproducibility of choroidal neovascularization through automated segmentation using deep learning. Improvements in projection artifact removal (PR-OCTA) technology are also progressing.
Evolution of the Concept of Pachychoroid Neovasculopathy
With the widespread use of OCTA, the independent pathological concept of type 1 macular neovascularization with a pachychoroid background is being established 6). Clinical validation of new biomarkers such as SIRE continues.
Standardization of Pathophysiology and Classification of Polypoidal Choroidal Vasculopathy
Debate continues on whether polyps in polypoidal choroidal vasculopathy are true aneurysms 6). International standardization of nomenclature and classification remains an unresolved issue, which is important for unifying treatment strategies.
Faricimab, which simultaneously inhibits VEGF-A and Ang-2 (angiopoietin-2), is being investigated for application in refractory choroidal neovascularization resistant to existing anti-VEGF monotherapy 3). Its novel mechanism of action of vascular stabilization is expected to extend injection intervals and show efficacy in treatment-resistant cases.
Elwood KF, et al. PEHCR: Diagnostic and Therapeutic Challenges. Medicina. 2023;59(9):1507.
Garg A, Khaleel H, Wahab C, Yan P. Acquired Focal Choroidal Excavation Secondary to Pachychoroid Choroidal Neovascular Membrane After Central Serous Chorioretinopathy. J Vitreoretin Dis. 2023;7(4):340-343. doi:10.1177/24741264231163395. PMID:37927310; PMCID:PMC10621713.
Maurizio Battaglia Parodi, Alessandro Arrigo, Adelaide Pina, Francesca Calcagno, Alessio Antropoli, Rashid Hassan Farah, Francesco Bandello, Ahmad M. Mansour. Choroidal neovascularization complicating sclerochoroidal calcifications. American Journal of Ophthalmology Case Reports. 2021;24:101235. doi:10.1016/j.ajoc.2021.101235.
Wu F, Mukai S. Refractory CNV in PXE and Cowden Syndrome. J VitreoRetinal Dis. 2023;7(1):70-73.
Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal Choroidal Vasculopathy: An Update on Diagnosis and Treatment. Clin Ophthalmol. 2023;17:53-70. doi:10.2147/OPTH.S385827. PMID:36636621; PMCID:PMC9831529.
Vemulakonda GA, Bailey ST, Kim SJ, Kovach JL, Lim JI, Ying GS, et al. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1-P74. doi:10.1016/j.ophtha.2024.12.018. PMID:39918524.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.