Retinal angiomatous proliferation (RAP) is a special subtype of age-related macular degeneration (AMD). Unlike other types of AMD that originate from choroidal vessels, new blood vessels arise from the deep retinal capillary plexus and, as they progress, may anastomose with choroidal neovascularization.
In 2001, Yannuzzi et al. proposed it as an independent disease entity and initially classified it into three stages (Stage 1 to 3) 3). Later, in 2010, Yannuzzi himself added Stage 4, reporting a four-stage classification. On the other hand, Freund et al. proposed the unified term “Type 3 neovascularization” and took the position that staging is unnecessary 4).
In the Japanese clinical practice guidelines for neovascular AMD (2024), macular neovascularization (MNV) is used as a general term for new vessels in the macula, and RAP is formally classified as “type 3 MNV” 1). Since the traditional term “choroidal neovascularization (CNV)” does not include retinal-derived new vessels, the shift to MNV is now progressing.
Traditionally, new vessels in the macula were called “choroidal neovascularization (CNV)”, but since retinal-derived new vessels are also included, the term “macular neovascularization (MNV)” has been used internationally since 2020 1). Type 3 MNV, corresponding to RAP, originates from retinal vessels and is clearly different in origin from type 1 and type 2 MNV, which are choroidal in origin.
In Western countries, RAP accounts for 15-20% of neovascular AMD patients. In Japan, the frequency is lower, reported at about 5% in Asians. It is characterized by a predilection for elderly women, with onset often at age 70 or older.
The rate of bilateral involvement is extremely high, and once one eye is affected, the risk of developing the condition in the fellow eye increases significantly. Therefore, clinical follow-up of the fellow eye is critically important. Compared to other AMD subtypes, progression is faster, and even with treatment, the recurrence rate is high. Over the long term, atrophic lesions tend to develop, and this subtype is recognized as having a poor visual prognosis among AMD types.
QIs RAP the same disease as age-related macular degeneration?
A
RAP is classified as a special subtype of age-related macular degeneration (AMD). The essential difference from typical neovascular AMD is the origin of the new blood vessels: they arise from the deep retinal capillary plexus rather than the choroid. In the current international classification, it is called “type 3 MNV” 1). Treatment approaches are similar, but the prognosis differs due to higher treatment resistance and bilateral involvement rates.
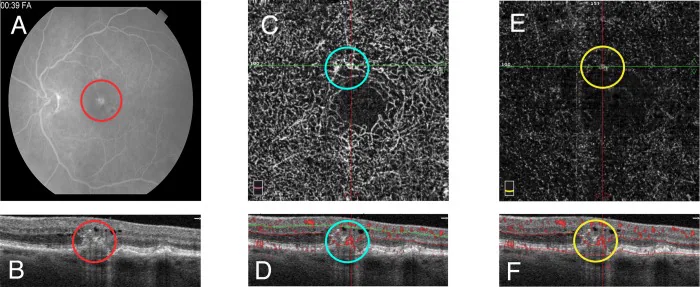
Fayed AE, et al. Projection resolved optical coherence tomography angiography to distinguish flow signal in retinal angiomatous proliferation from flow artifact. PLoS One. 2019. Figure 1. PMCID: PMC6519823. License: CC BY.
A shows hyperfluorescence on fluorescein angiography, B shows intraretinal hyperreflective lesions on OCT, and C and D show abnormal vascular structures and blood flow signals in the deep capillary plexus on OCTA. These correspond to the intraretinal angiomatous lesions discussed in section “2. Main Symptoms and Clinical Findings.”
The following subjective symptoms appear from the early to middle stages.
Metamorphopsia (distorted vision): Occurs due to macular edema and exudation. This is a common initial complaint.
Central scotoma: When the lesion involves the fovea, patients notice a defect in the central visual field.
Visual acuity loss: Progresses rapidly during periods of high activity of cystoid macular edema or neovascularization.
Symptom progression is relatively fast, and compared to other AMD subtypes, severe visual loss tends to occur early. When cystoid macular edema is prominent, rapid visual decline may occur, making early consultation and diagnosis important for preserving visual function.
Clinical Findings (Findings Confirmed by Physician Examination)
The characteristic background findings include clusters of soft drusen in the posterior pole and reticular pseudodrusen (RPD). RPD are reticular to dot-like deposits located on the retinal pigment epithelium (RPE) and are considered important precursor lesions for RAP 1).
During the active phase, the following findings are observed.
Superficial retinal hemorrhage and intraretinal hemorrhage: Small to moderate amounts of hemorrhage in the posterior pole. In particular, in Stage 1, a small amount of superficial hemorrhage is observed around the neovascularization, which appears as nodular red dots.
Cystoid macular edema: A characteristic finding of RAP, which tends to appear more severely and earlier than in other AMD subtypes.
Subretinal fluid and serous retinal detachment: Appear from Stage 2 onward.
Type 3 MNV is difficult to observe with ophthalmoscopy or fundus photography, so confirmation by imaging is essential 1). The main examination methods and findings are summarized below.
Noninvasive visualization of intraretinal and subretinal neovascularization
OCT is the mainstay for staging RAP and evaluating treatment response. The bump sign is a small elevated lesion just above the RPE and is considered relatively specific for type 3 MNV. OCT shows cystoid macular edema from early onset, and PED develops as the disease progresses 1).
OCTAB-scan images can capture intraretinal neovascularization anastomosed with superficial retinal vessels extending into the subretinal space or penetrating the RPE into the sub-RPE space 1). Since RAP originates within the retina, abnormal vessels are particularly well visualized on OCTA among AMD subtypes. In elderly patients who cannot undergo repeated contrast angiography, noninvasive lesion assessment with OCTA is useful 10).
IRF (intraretinal fluid) and SRF (subretinal fluid) are used as indicators of disease activity. Because type 3 MNV lesions do not necessarily occur at the fovea, it is recommended to scan the entire macula or the entire lesion to accurately assess fluid 1).
QWhat can be seen on OCT?
A
On OCT, a characteristic finding is a mass-like reflection just above the RPE called the “bump sign.” Additionally, cystoid macular edema, intraretinal fluid (IRF), subretinal fluid (SRF), and pigment epithelial detachment (PED) are observed. OCTAB-scan images show continuous blood flow signals from superficial retinal vessels to the bump sign 1). The presence or absence of IRF and SRF is used as an indicator for activity assessment.
Aging: The greatest risk factor. The older the age, the higher the risk of onset.
Sex: More common in women.
Soft drusen in the posterior pole: Eyes with multiple large soft drusen (≥125 μm in diameter) in the macula are important precursors for the progression of AMD1).
Reticular pseudodrusen (RPD): Recognized as the precursor lesion most closely associated with the onset of RAP. RPD are reticular to dot-like deposits located above the RPE, distinct from typical drusen (which are beneath the RPE), and are widely known as risk factors for progression to type 3 MNV and atrophic AMD1).
Genetic predisposition: Polymorphisms in the ARMS2 gene and the CFH (complement factor H) gene contribute to overall AMD susceptibility 11). Large-scale genome-wide association studies have confirmed that these loci are major determinants of AMD risk.
Smoking: A risk factor for overall AMD and the most important modifiable risk factor. The Funagata, Hisayama, and Nagahama studies in Japanese populations have all reported an association between smoking and AMD, with the Hisayama study indicating that smoking increases the risk of late AMD by fourfold 12).
A high rate of bilateral involvement is also an important feature; when one eye is affected, regular follow-up of the fellow eye is essential. If soft drusen or RPD are also present in the fellow eye, the risk of onset is even higher, requiring close-interval detailed examinations.
Regarding sex ratio, overall neovascular AMD is more common in men (male:female = 3:1), whereas RAP is more common in women. The age of onset is similar to or slightly older than that of overall AMD, with the majority being 70 years or older.
QIf only one eye is affected, will the other eye also develop the condition?
A
RAP has a very high rate of bilateral involvement. Even when only one eye is affected, the risk of the fellow eye developing the condition is higher than for other AMD subtypes. Regular detailed examinations of the fellow eye are essential from the time of unilateral onset.
Type 3 MNV is difficult to observe with ophthalmoscopy or fundus photography, so a systematic evaluation combining multiple imaging tests is essential for definitive diagnosis 1).
The diagnostic procedure is as follows.
Clinical suspicion: Suspect type 3 MNV in elderly patients with multiple soft drusen in both eyes and intraretinal hemorrhage in the posterior pole.
OCT examination: Cystoid macular edema appears early in the disease; a bump sign (RPE break-like mound reflex) is highly suggestive. Presence of PED indicates progression.
OCTA examination: On B-scan, confirm continuous blood flow signal from superficial retinal vessels toward the bump sign. Non-invasive and particularly useful for elderly patients who have difficulty with contrast imaging.
FA/ICGA examination: FA shows nodular hyperfluorescence (hot spot) and intense late leakage. ICGA reveals RRA/RCA as a hot spot, contributing to disease staging.
OCT is the mainstay for assessing activity, non-invasively determining the presence of IRF, SRF, and sub-RPE fluid 1). Differentiation between serous PED and hemorrhagic PED is based on OCT content brightness: medium brightness suggests drusen, low brightness suggests serous fluid.
Ellipsoid zone defect, retinal cavity (no thickening)
Progression rate
Fast (mainly exudation/hemorrhage)
Slow (mainly retinal atrophy)
In MacTel type 2, right-angled venules (small veins that bend at a right angle and are drawn into the deep retinal layers) and crystallin-like deposits are characteristic findings. Red-free images (especially confocal blue light reflectance) show a ring-shaped or horizontally oval hyperreflective lesion in the macula, which is present from the early stage and is useful for diagnosis 5). On OCT, retinal cavities without retinal thickening are characteristic, and progression may lead to outer lamellar holes or macular holes 5).
In contrast, RAP is characterized by a hot spot on IA and clustering of soft drusen, and OCT predominantly shows a bump sign and cystoid macular edema, clearly distinguishing it from MacTel. MacTel progresses slowly with mainly retinal atrophy, whereas RAP tends to progress rapidly with exudation and hemorrhage.
Differential diagnosis from polypoidal choroidal vasculopathy (PCV)
PCV shows polypoidal lesions (nodular hyperfluorescence) and an abnormal vascular network (branching vascular network) on IA, and OCT typically shows a steep RPE elevation with an internal hyporeflective cavity 1). Fundus photography reveals orange-red elevated lesions. RAP is differentiated by a predominant hot spot on IA and prominent cystoid macular edema. PCV is often associated with choroidal thickening (pachychoroid findings), whereas RAP has a background of clustered soft drusen and RPD.
Differential diagnosis from typical AMD (type 1 and type 2 MNV)
In typical AMD, neovascularization originates from the choroid. Type 1 MNV is located beneath the RPE and shows a double-layer sign on OCT. Type 2 MNV is located above the RPE (subretinal space) and appears as a medium-reflective mass on OCT1). RAP can be distinguished by the presence of intraretinal neovascularization originating from retinal vessels, leading to early cystoid macular edema and a bump sign. Additionally, RAP is often bilateral and tends to be associated with multiple soft drusen.
The first-line treatment for neovascular AMD is intravitreal anti-VEGF injection 1). For type 3 MNV, all anti-VEGF agents have also shown visual improvement effects.
Currently, anti-VEGF drugs available for neovascular AMD are as follows1).
Ranibizumab (Lucentis/Ranibizumab BS): In the MARINA study, the sham group lost 14.9 letters of visual acuity over 24 months, while the monthly ranibizumab group gained 6.6 letters14). The ANCHOR study also demonstrated superiority over PDT15).
Aflibercept 2 mg (Eylea): In the VIEW 1/2 studies, dosing every 8 weeks after 3 initial loading doses showed non-inferiority in maintaining visual acuity compared to monthly ranibizumab6).
Brolucizumab 6 mg (Beovu): In the HAWK/HARRIER studies, dosing every 8–12 weeks after 3 initial loading doses showed non-inferiority in visual acuity improvement compared to aflibercept, and superiority in reducing central retinal thickness7).
Faricimab (Vabysmo): A bispecific antibody against VEGF and angiopoietin-2. In the TENAYA/LUCERNE studies, dosing every 8–16 weeks after 4 initial loading doses showed non-inferiority to aflibercept8).
Loading phase: One injection per month, usually 3 consecutive doses (4 for faricimab), to improve visual acuity1).
Maintenance phase administration methods include the following options.
Fixed dosing: The method used in clinical trials. Administered at fixed intervals (e.g., every 8 weeks).
Pro re nata (PRN): Monthly monitoring, with injection only when disease activity is observed. However, long-term reports indicate that PRN may lead to worsening of visual acuity1, 13).
Treat-and-extend (T&E): A method that gradually extends the dosing interval based on disease activity. This is currently the most recommended maintenance therapy. Meta-analyses show that it maintains visual improvement comparable to monthly dosing and achieves better visual outcomes than PRN1).
In the ALTAIR study targeting Japanese patients, the T&E method for aflibercept (adjusting intervals by 2-week or 4-week increments) maintained improvements in visual acuity and retinal thickness over 96 weeks9). There is no consensus on how long to continue T&E; decisions should consider the patient’s condition and social circumstances1).
OCT is the main tool for evaluating treatment response. The presence or recurrence of fluid around the MNV (IRF, SRF, sub-RPE fluid) indicates activity1). Since type 3 MNV intraretinal neovascularization is not necessarily confined to the fovea, scanning the entire macula or the entire lesion is recommended.
When the effect is poor during treatment (treatment-resistant cases) or when the effect diminishes (acquisition of resistance), switching to another anti-VEGF drug may be effective 1). Since RAP is a disease type that tends to show treatment resistance, early switching when response is poor is important. Switching drugs may also be considered to reduce treatment burden.
PDT alone for type 3 MNV is currently not recommended 1). In cases resistant to anti-VEGF drugs, combination with PDT may be considered, but PDT may worsen macular atrophy in the long term. It is desirable to avoid PDT in cases with thin choroid or pre-existing macular atrophy 1).
The prescription when combining PDT is as follows.
Verteporfin (Visudyne): 6 mg/m² body surface area, intravenous infusion over 10 minutes
Laser irradiation: Irradiation 15 minutes after start of infusion (689 nm, 600 mW/cm², 83 seconds)
Irradiation spot size: Maximum lesion diameter based on angiographic findings + 1,000 μm
Timing of anti-VEGF combination: Administered within 1 week before PDT or on the same day as PDT (under light shielding)
Postoperative management: Avoid direct sunlight for 2 days after treatment
Complete cure of neovascular AMD is currently impossible, and without appropriate treatment and long-term management, irreversible vision loss occurs 1). RAP requires particular long-term attention regarding the following points.
Even if MNV activity is quiet, recurrence may occur over the long term
Repeated exudation leads to atrophic changes and fibrous scarring. Over the long term, retinal atrophy (geographic atrophy) is likely to occur, which is the main cause of irreversible vision loss
MNV also occurs at a high rate in the fellow eye
When severe visual function decline occurs, actively consider introducing low vision care such as magnifiers and magnifying reading devices. Since complete cure of neovascular AMD is impossible, it is desirable to share a sustainable management plan with the patient, taking into account the patient’s social situation and the condition of the fellow eye 1).
QHow many injections are needed?
A
There is significant individual variation, but after an initial loading phase of 3 consecutive doses (4 for faricimab), the interval is adjusted using a treat-and-extend regimen 1). RAP tends to be more treatment-resistant than other AMD subtypes and may require many injections. The ALTAIR study in Japanese patients confirmed maintenance of treatment effect over 96 weeks 9). Newer agents such as faricimab allow maintenance dosing at intervals up to 16 weeks, reducing treatment burden 8).
The essence of RAP is intraretinal neovascularization originating from the deep retinal capillary plexus. This is the basis for naming it “type 3 MNV,” and its pathogenesis is fundamentally different from type 1 and type 2 MNV, which originate from the choroid1).
The classification of type 3 MNV within MNV is as follows:
The aggregation of soft drusen and reticular pseudodrusen (RPD) are important as precursor lesions. RPD are triangular-shaped deposits located above the retinal pigment epithelium (RPE), unlike typical drusen which are deposits beneath the RPE. On OCT, they appear as protrusions from the RPE layer into the retina, sometimes extending beyond the ellipsoid zone to the external limiting membrane. RPD are closely associated with atrophic AMD and type 3 MNV (RAP), and are clinically important as predictors of RAP development 1).
Against the background of RPD and soft drusen accumulation, dysfunction of the RPE and photoreceptors progresses. Under chronic hypoxic conditions, pro-angiogenic factors including VEGF are produced and accumulate, inducing sprouting of new vessels from the deep capillary plexus. The new vessels progress stepwise through the following stages.
Stage 1: New vessel formation within the deep capillary plexus (intraretinal neovascularization)
In the original 2001 report by Yannuzzi et al., a model of progression from the retinal side toward the choroid was proposed 3). However, with recent advances in OCT, a form in which new vessels originate from the choroidal side and anastomose with retinal vessels has also been reported. Freund et al. refer to new vessels that form retinal-choroidal anastomosis as “Type 3 neovascularization” and take the position that staging is unnecessary 4).
Currently, the following three pathways are hypothesized.
In any pathway, damage to the RPE and photoreceptors is the starting point for increased VEGF production. Once retinal-choroidal anastomosis is established, treatment resistance further increases and progression to fibrous scarring accelerates, so it is important to suppress neovascular activity as early as possible.
7. Latest research and future perspectives (reports at the research stage)
In the 2-year results of the TENAYA and LUCERNE trials (Khanani et al., 2024), faricimab (anti-VEGF/anti-Ang-2 bispecific antibody) maintained non-inferiority in visual and anatomical outcomes compared to aflibercept 2 mg, and approximately half of patients achieved maintenance dosing at intervals of up to 16 weeks 8). Synergistic effects of vascular stabilization and exudation suppression through Ang-2 inhibition are expected.
Aflibercept 8 mg (high-dose formulation) is more concentrated than the existing 2 mg formulation, and maintenance dosing at intervals of up to 16–20 weeks is being investigated in the PULSAR trial 2). In disease types such as RAP that require multiple injections, extending the dosing interval is expected to greatly reduce treatment burden.
OCTA is rapidly being introduced into clinical practice as a non-invasive modality for assessing the activity of retinal neovascularization10). RAP is suitable for visualization with OCTA because neovascularization is present within the retina, and it is expected to serve as an alternative when repeated contrast imaging is difficult in elderly patients. Future challenges include the development of treatment decision algorithms based on quantitative OCTA analysis.
Genetic personalized treatment and prevention strategies
Research is progressing on risk stratification and personalized treatment strategies based on ARMS2 and CFH gene polymorphisms 11). The realization of treatment selection and preventive interventions according to genetic profiles is considered a future challenge. The possibility of improving visual prognosis by identifying patients at high genetic risk at the intermediate AMD stage and providing early treatment intervention is being explored.
In neovascular AMD including RAP, massive submacular hemorrhage can cause sudden vision loss. In the early stage, intravitreal gas injection (SF6 or C3F8 0.3–0.5 mL injection plus prone positioning) or vitrectomy with hematoma displacement may be effective for visual improvement. Concomitant use of tissue plasminogen activator (tPA) has also been attempted, but further investigation of indications is needed 1).
Freund KB, Ho IV, Barbazetto IA, Koizumi H, Laud K, Ferrara D, et al. Type 3 neovascularization: the expanded spectrum of retinal angiomatous proliferation. Retina (Philadelphia, Pa.). 2008;28(2):201-11. doi:10.1097/IAE.0b013e3181669504. PMID:18301024.
Jeffrey S. Heier, David M. Brown, Victor Chong, Jean-Francois Korobelnik, Peter K. Kaiser, Quan Dong Nguyen, Bernd Kirchhof, Allen Ho, et al. Intravitreal Aflibercept (VEGF Trap-Eye) in Wet Age-related Macular Degeneration. Ophthalmology. 2012;119(12):2537-2548. doi:10.1016/j.ophtha.2012.09.006.
Dugel PU, Koh A, Ogura Y, Jaffe GJ, Schmidt-Erfurth U, Brown DM, et al. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2020;127(1):72-84. doi:10.1016/j.ophtha.2019.04.017. PMID:30986442.
Khanani AM, Kotecha A, Chang A, Chen SJ, Chen Y, Guymer R, Heier JS, Holz FG, et al. TENAYA and LUCERNE: Two-Year Results from the Phase 3 Neovascular Age-Related Macular Degeneration Trials of Faricimab with Treat-and-Extend Dosing in Year 2. Ophthalmology. 2024;131(8):914-926. doi:10.1016/j.ophtha.2024.02.014. PMID:38382813.
Ohji M, Takahashi K, Okada AA, et al. Efficacy and safety of intravitreal aflibercept treat-and-extend regimens in exudative age-related macular degeneration: 52- and 96-week findings from ALTAIR: A Randomized Controlled Trial. Adv Ther. 2020;37(3):1173-1187. doi:10.1007/s12325-020-01236-x.
Richard F. Spaide, James G. Fujimoto, Nadia K. Waheed, Srinivas R. Sadda, Giovanni Staurenghi. Optical coherence tomography angiography. Progress in Retinal and Eye Research. 2018;64:1-55. doi:10.1016/j.preteyeres.2017.11.003.
Fritsche LG, Igl W, Bailey JN, Grassmann F, Sengupta S, Bragg-Gresham JL, et al. A large genome-wide association study of age-related macular degeneration highlights contributions of rare and common variants. Nature genetics. 2016;48(2):134-43. doi:10.1038/ng.3448. PMID:26691988; PMCID:PMC4745342.
Klein R, Klein BE, Knudtson MD, Meuer SM, Swift M, Gangnon RE. Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology. 2007;114(2):253-62. doi:10.1016/j.ophtha.2006.10.040. PMID:17270675.
Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, Toth C, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388-98. doi:10.1016/j.ophtha.2012.03.053. PMID:22555112; PMCID:PMC3389193.
Philip J. Rosenfeld, David M. Brown, Jeffrey S. Heier, David S. Boyer, Peter K. Kaiser, Carol Y. Chung, Robert Y. Kim. Ranibizumab for Neovascular Age-Related Macular Degeneration. N Engl J Med. 2006;355(14):1419-1431. doi:10.1056/nejmoa054481.
Brown DM, Kaiser PK, Michels M, Soubrane G, Heier JS, Kim RY, Sy JP, Schneider S, ANCHOR Study Group.. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444. doi:10.1056/nejmoa062655. PMID:17021319.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.