Indocyanine green angiography (ICGA) is a fluorescence angiography test in which ICG dye is injected intravenously and the fundus is photographed using near-infrared light. It allows detailed observation of choroidal vessels that are difficult to visualize with fluorescein angiography (FA).
ICG (indocyanine green) is a dark greenish-blue water-soluble dye with a molecular weight of about 775 (approximately 2.3 times that of fluorescein used in FA, which is about 332). The following optical properties are advantageous for choroidal angiography.
Maximum absorption wavelength: 805 nm (when protein-bound)
Fluorescence wavelength: 835 nm
Near-infrared region: Penetrates melanin in the RPE, allowing direct visualization of the choroid
While FA uses visible light with excitation at 465–490 nm and fluorescence at 520–530 nm, ICGA uses near-infrared light that is less absorbed by RPE melanin. This wavelength characteristic enables visualization of sub-RPE and choroidal lesions that are difficult to depict with FA.
After administration, ICG plasma concentration decreases exponentially. Its half-life is short, about 3–4 minutes, and it is taken up by hepatocytes and excreted into bile without metabolism (no enterohepatic circulation). This metabolic pathway differs from FA, which is renally excreted. ICGA can be used to some extent even in patients with renal impairment, but caution is needed in hepatic impairment due to delayed excretion.
In the 1960s, Fox and Wood first applied ICG to ophthalmology. In the 1970s, its use in fluorescein fundus angiography was reported, and in the 1990s, clinical application became widespread with the advent of digital technology.
QHow are ICGA and FA used differently?
A
FA is superior for evaluating retinal vascular disorders and RPE function, while ICGA is superior for visualizing choroidal vessels and sub-RPE lesions. ICGA is essential for PCV and diseases with choroidal vascular hyperpermeability (e.g., central serous chorioretinopathy). Both are often performed simultaneously.
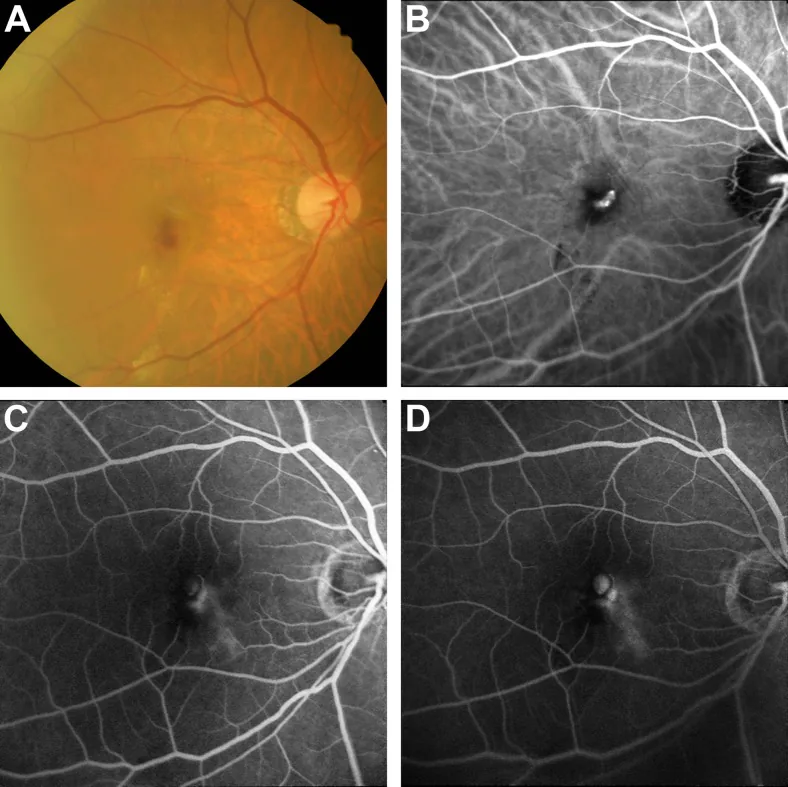
Tan CS, et al. EVEREST study report 3: diagnostic challenges of polypoidal choroidal vasculopathy. Lessons learnt from screening failures in the EVEREST study. Graefes Arch Clin Exp Ophthalmol. 2016. Figure 2. PMCID: PMC5045476. License: CC BY.
In a patient with RAP, (a) color fundus photograph showing macular hemorrhage, (b) hyperfluorescent spot on ICGA resembling a polyp, (c) and (d) FA showing dye leakage and pooling in cystic spaces. This corresponds to retinal angiomatous proliferation discussed in section “2. Indications and Clinical Findings”.
Type 2 choroidal neovascularization (classic type): Useful for identifying the full extent of the abnormal vascular network and the feeding choroidal vessels.
Type 3 macular neovascularization (RAP: retinal angiomatous proliferation): Reported to be associated with approximately one-quarter of Type 1 macular neovascularization.
It delineates the extent and degree of choroidal vascular hyperpermeability and is useful for determining the irradiation site for photodynamic therapy (PDT). It is also excellent for visualizing dilated inner choroidal vessels (pachyvessels).
VKH (Vogt-Koyanagi-Harada disease): Useful for detecting choroidal thickening, filling delay, and early recurrence. Multiple patchy hypofluorescent spots are seen from the early phase.
There are mainly two types of ICGA imaging equipment.
Fundus camera type: Equipped with excitation filter 640–780 nm and barrier filter 820–900 nm. Suitable for wide-field imaging.
Scanning laser ophthalmoscope (SLO) type: Uses a 785 nm diode laser as the light source. Wide dynamic range and high contrast. Simultaneous imaging with FA is possible, allowing simultaneous evaluation of the retina and choroid.
Many of these devices allow simultaneous imaging with FA (excitation 488 nm).
Assessment of dye pooling and tissue staining. Differentiation by residual fluorescence in lesions
In the early phase, filling begins from the short posterior ciliary arteries and flows into the choriocapillaris. In the middle phase, uniform choroidal background fluorescence is obtained, and in the late phase, background fluorescence attenuates and large vessels emerge as silhouettes. Residual fluorescence (staining) is useful for differentiating lesions.
Since ICG fluorescence intensity decreases exponentially over time, attention must be paid to light intensity settings. Generally, it is set high at the start of imaging, lowered once fluorescence is confirmed, and increased again toward the late phase.
When performing FA and ICGA simultaneously, sequential administration of FA followed by ICG, or nearly simultaneous administration, is performed. With the SLO method, both angiographies can be captured simultaneously with a single device.
QIs ICGA examination painful?
A
There may be a mild stinging sensation when the contrast agent is injected intravenously, but the examination itself is essentially painless. Eye drops for pupil dilation are required, and after dilation, glare and blurred near vision may occur for several hours. Driving a car or motorcycle should be avoided on the day of the examination.
In normal eyes, the early phase shows filling in the order of choroidal arteries → veins → choriocapillaris, and a uniform background fluorescence is obtained in the middle phase. In the late phase, background fluorescence gradually decreases, and silhouettes of large vessels emerge. Window defects observed in FA do not occur in ICGA because ICG penetrates the RPE and reaches the choroidal vessels.
Blocking: Blockage of ICG fluorescence by thick hemorrhage, pigment, or exudate.
Delayed filling: Delayed arrival due to choroidal ischemia. Seen in giant cell arteritis, triangular syndrome, and Takayasu arteritis.
Filling defect (choriocapillaris non-perfusion): Non-perfusion of the choriocapillaris due to acute inflammation such as APMPPE. Also observed in MEWDS and the acute phase of VKH.
Choroidal neovascular network: A hyperfluorescent reticular structure that persists into the late phase in age-related macular degeneration Type 1 macular neovascularization.
Lipid accumulation in Bruch’s membrane prevents ICG from reaching the RPE properly. This results in localized hypofluorescent spots in the late phase of ICGA (ASHS-LIA: area of decreased late-phase hypofluorescence after ICG angiography). 4) This is an important finding for understanding the pathology of age-related macular degeneration and polypoidal choroidal vasculopathy.
ICGA is a relatively safe examination, but because it involves intravenous injection, side effects may occur. According to a report by Hope-Ross (1994), the overall frequency of side effects is approximately 0.15%, and severe anaphylactic shock occurs in about 0.05% of cases. The frequencies of major side effects are shown in the table below.
Severity
Symptoms
Frequency (approximate)
Mild
Nausea, vomiting, feeling of warmth
Approximately 0.15%
Moderate
Urticaria, fever, blood pressure changes
Approximately 0.2%
Severe
Anaphylactic shock
Approximately 0.05%
For reference, FA has been reported to have a mortality risk of approximately 1 in 200,000 5), and ICGA requires a similar level of risk management.
After the examination, blood pressure should be measured, and the patient’s condition should be confirmed before discharge 6). If adverse effects occur, it is recommended to report them 6).
QCan I receive the test if I have an iodine allergy?
A
ICG preparations (e.g., Ophthagreen®) contain sodium iodide as a stabilizer. A history of iodine allergy is an absolute contraindication for ICGA, and allergy history must be confirmed before administration. Switching to iodine-free infrared cyanine green may be considered.
ICG is an amphiphilic cyanine dye with a molecular weight of 775. Below, the pharmacological properties of ICG and a comparison with FA are shown.
High protein binding rate (98%): Almost all ICG binds to albumin and lipoproteins in plasma, remaining within blood vessels with little leakage. The protein binding rate of FA is about 80%, and even in lesions with profuse fluorescein leakage on FA, leakage is less prominent on ICGA.
Plasma half-life of 3–4 minutes: Plasma concentration decreases exponentially after administration. In the late phase, background fluorescence diminishes, making residual fluorescence in lesions stand out.
Metabolism and excretion: After hepatic uptake, it is excreted into bile without metabolism (no enterohepatic circulation). Unlike other cyanine dyes, it has low accumulation in the body. This route differs from FA’s renal excretion, allowing some use in patients with renal impairment, but caution is needed in hepatic impairment due to accumulation.
Low quantum yield: ICG’s fluorescence quantum yield is lower than that of FA, resulting in weak fluorescence signals. This is why high-sensitivity near-infrared cameras and appropriate light intensity settings are necessary.
Abnormal vascular networks (BVN) are detected as high-flow areas on OCTA, but ICGA is superior for detecting polypoidal lesions. 2) The relatively slow blood flow within polyps and the high intravascular retention of ICG allow gradual filling and clearer visualization in the late phase.
TelCaps (Telangiectatic Capillary anomalies) are large capillary anomalies (diameter ≥150 μm) with high affinity for ICG. 1) These lesions are difficult to detect with FA or OCTA and are noted as a cause of anti-VEGF treatment-resistant macular edema.
Perrin and Porter (2024) reported a case series of ICGA-guided photocoagulation (TelCaps PDT) for TelCaps. 1) In 13 eyes with diabetic macular edema, TelCaps-targeted photocoagulation resulted in significant improvement over two years. A prospective RCT involving 270 patients is currently underway in France.
Development of Non-ICGA Diagnostic Criteria for Polypoidal Choroidal Vasculopathy
Cheung et al. (2025) reported an AUC of 0.90 for OCT-based non-ICGA diagnostic criteria. 4) These criteria combine OCT findings of pachychoroid (choroidal thickening, central serous chorioretinopathy-like changes, and findings equivalent to BVN).
QIs ICGA still necessary now that OCTA is widely used?
A
ICGA is still necessary for the definitive diagnosis of polypoidal choroidal vasculopathy. OCTA is excellent for detecting BVN and evaluating blood flow, but ICGA has been reported to be superior in detecting polypoidal lesions. 2) Although non-ICGA diagnostic criteria are being developed (AUC 0.90), ICGA is currently indispensable for the standard diagnosis of polypoidal choroidal vasculopathy.
Perrin EL, Porter RGB. ICG angiography-guided photocoagulation of large microvascular abnormalities (TelCaps). Retinal Cases Brief Rep. 2024;18:355-359.
Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal Choroidal Vasculopathy: An Update on Diagnosis and Treatment. Clin Ophthalmol. 2023;17:53-70. doi:10.2147/OPTH.S385827. PMID:36636621; PMCID:PMC9831529.
Vemulakonda GA, Bailey ST, Kim SJ, Kovach JL, Lim JI, Ying GS, et al. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P1-P74. doi:10.1016/j.ophtha.2024.12.018. PMID:39918524.
Cheung CMG, Dansingani KK, Koizumi H, et al. Pachychoroid disease: review and update. Eye (Lond). 2025;39(5):819-834. doi:10.1038/s41433-024-03253-4.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P270-P302. doi:10.1016/j.ophtha.2024.12.024. PMID:39918522.