Polypoidal choroidal vasculopathy (PCV) is a disease characterized by an abnormal branching vascular network (BVN) of the choroid and polypoidal vascular dilations at its terminals. 5) It is a subtype of age-related macular degeneration (AMD) that shows polypoidal choroidal vessel dilation on indocyanine green angiography (ICGA), forming orange-red spherical lesions under the retinal pigment epithelium (RPE) and causing serous or hemorrhagic pigment epithelial detachment (PED).
It commonly occurs in men aged 50–65 years. Among Asians, it accounts for 22–62% of patients with exudative nAMD, 5) and some reports indicate that about half of exudative AMD cases are PCV. 11) In Western Caucasians, it accounts for only about 10–20%. 5) The global population aged 65 and over is estimated to exceed 1.5 billion by 2050, and an increase in nAMD and PCV patients is expected. 5)
QIs polypoidal choroidal vasculopathy the same disease as age-related macular degeneration (AMD)?
A
Polypoidal choroidal vasculopathy is often classified as a subtype of nAMD, but there are differences in pathology, treatment response, and genetic background. It tends to have more hemorrhage and less IRF than nAMD. Whether it should be considered an independent disease entity within the pachychoroid spectrum is still under debate. 5, 6)
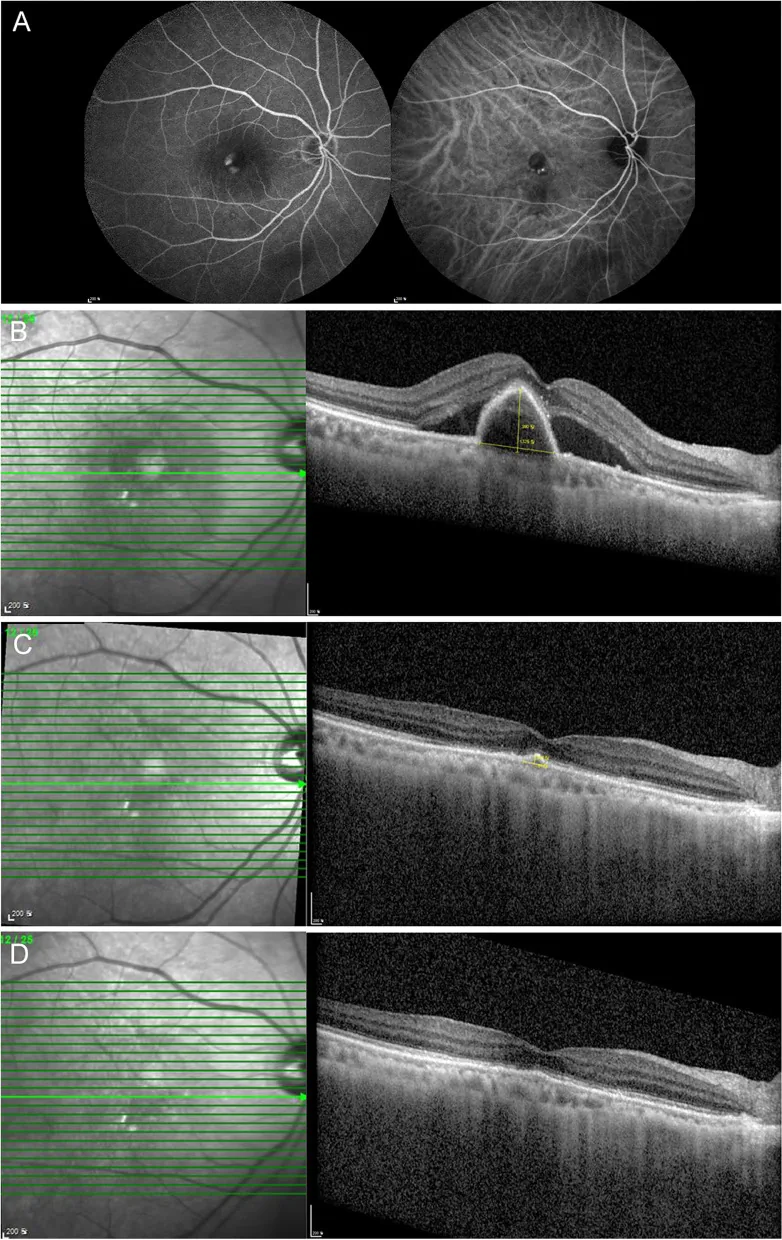
Nam SW, et al. Response to brolucizumab treatment for refractory serous pigment epithelial detachment secondary to polypoidal choroidal vasculopathy. BMC Ophthalmol. 2022. Figure 2. PMCID: PMC9749193. License: CC BY.
Decreased visual acuity: Lesions involving the fovea cause acute and progressive vision loss. 5)
Metamorphopsia (distortion): Straight lines appear bent due to exudative changes in the macula.
Central scotoma: When the lesion extends to the fovea, a dark area is perceived in the center of the visual field.
Sudden worsening of vision: Occurs when massive submacular hemorrhage (SMH) develops. Hemorrhagic changes are characteristic, and the incidence of SMH over 5 years is reported to be about 10%. 5)
Compared to typical nAMD, polypoidal choroidal vasculopathy tends to have abundant hemorrhage but less intraretinal fluid (IRF). It is also characterized by frequent serous PED and subretinal hemorrhage.
Clinical Findings (Findings Confirmed by Physician Examination)
Fundus examination reveals characteristic orange-red elevated lesions. These are observed as polypoidal vascular dilations under the RPE. They are often accompanied by hemorrhagic PED or serosanguinous PED.
Features of PCV
Orange-red spherical lesion: Polyp-like vascular dilation under the RPE. Observed as an orange-red spherical lesion on ophthalmoscopy.
Hemorrhagic pigment epithelial detachment: Steep elevation due to massive hemorrhage under the RPE. IRF tends to be minimal.
OCT findings provide important information for the diagnosis of PCV. 5)
Double-layer sign: A finding showing a double-layer structure of the RPE and Bruch’s membrane. Observed in the area of abnormal vascular network. Sensitivity 59%. 5)
Steep RPE elevation: Characterized by a steep elevation of the RPE corresponding to the polyp lesion.
Hematocrit sign: Separation of fluid and blood within a hemorrhagic PED.
Bola (thumb-like PED): Rounded, polyp-like steep elevation under the RPE.
APOIS criteria: Combination of OCT findings achieves AUC 0.90 for differentiation from nAMD. 5, 12)
Many cases are known to have a thick choroid, and the association with the pachychoroid spectrum is attracting attention.
ICGA: Characteristic polypoidal choroidal vascular dilations and abnormal vascular network (branching vascular network) are observed. Detection of polypoidal lesions is the definitive diagnosis. 5, 7)
Fluorescein angiography (FA): Areas corresponding to polypoidal lesions show hyperfluorescence relatively early. In the late phase, window defects corresponding to atrophic lesions are often seen.
OCTA can noninvasively visualize blood vessels, and the branching vascular network (BVN) is often more clearly depicted than with ICGA. 5) A BNN 3-type classification has been reported, with a PCV detection sensitivity of 82.6% and specificity of 100%. 5) However, detection of polypoidal lesions is limited and inferior to ICGA. For the differential diagnosis of PCV and retinal angiomatous proliferation (RAP), OCTA alone still has challenges, and multimodal imaging diagnosis is important.
Polypoidal choroidal vasculopathy is a special type of type 1 choroidal neovascularization (CNV) located under the RPE. 5, 8) The underlying pathological basis is considered to be pachychoroid, characterized by dilation of Haller’s layer (outer choroidal vascular layer) and associated thinning of Sattler’s layer and the choriocapillaris. 5)
Vortex vein stasis: Stasis of choroidal veins causes dilation of Haller’s layer. In about 90% of cases, dilated pachyvessels are anastomosed with vortex veins. 5)
Ischemia/occlusion of the choriocapillaris: Ischemia at the choriocapillaris level induces the formation of neovascular complexes (BVN). 5)
Damage to RPE and Bruch’s membrane: Chronic choroidal stasis damages the RPE and Bruch’s membrane, leading to the formation of polypoidal lesions with increased protease activity. 5)
Associations with polymorphisms in CFH (complement factor H) and ARMS2/HTRA1 genes have been reported. 5) Some susceptibility genes overlap with typical nAMD, but in the non-pachychoroid type (drusen-driven PCV, normal choroidal thickness), the ARMS2/HTRA1 association is stronger. 5, 8) SNPs in the ANGPT2 gene and missense mutations in the FGD6 gene have also been suggested to be associated with PCV development. 5)
About half of PCV eyes show normal choroidal thickness. 5) The pachychoroid type tends to occur in younger individuals, has more CSC-like features, is associated with choroidal vascular hyperpermeability, and may show resistance to anti-VEGF therapy. The non-pachychoroid type is drusen-driven (AMD-like features) and has a stronger association with ARMS2/HTRA1. 5, 8)
Choriocapillaris flow deficit (CCFD) is increased not only in eyes with PCV but also in healthy fellow eyes, suggesting that pachychoroid may act as a systemic predisposition rather than a local factor. 5)
Secondary PCV after choroiditis: Chronic damage to the RPE and Bruch’s membrane due to tuberculous choroiditis can be a predisposing factor. A case has been reported where PCV developed about 20 years after inflammation, and visual acuity improved from 6/9 to 6/6 after three injections of aflibercept. 1)
Rapid progression after COVID-19 vaccine: A case (79-year-old male) has been reported where symptoms appeared 16 hours after the third vaccination and rapidly progressed to massive submacular hemorrhage within two weeks. 4)
PCV consists of polypoidal lesions and an abnormal vascular network. Current diagnostic criteria classify it as follows.
Definite case: Orange-red elevated lesions are observed on fundus examination, and polypoidal lesions are detected on ICGA. 7)
Suspicious findings: Only an abnormal vascular network is seen on ICGA. Recurrent hemorrhagic or serous retinal pigment epithelial detachment is observed.
The diagnostic criteria based on ICGA established by the EVEREST study group are widely used internationally. 7, 10) PCV is diagnosed if any of the following are met.
Orange-red spherical lesions observed on fundus examination
Nodular hyperfluorescent lesions (polyps) observed on ICGA
Abnormal branching vascular network (BVN) is observed on ICGA.
ICGA is the gold standard for diagnosing PCV. 5, 7) It excels at visualizing choroidal vessels and can depict vascular structures even through sub-RPE hemorrhage, fluid, and lipids due to the long-wavelength properties of ICG. 5) It identifies polypoidal lesions with early hyperfluorescence and BVN.
For PCV differentiation using OCT alone, the APOIS criteria (APOIS PCV workgroup) have been reported to have an AUC of 0.90. 5, 12) The double-layer sign is useful for screening in facilities that do not perform ICGA, but its sensitivity remains at 59%. 5) When ICGA is not available, a combination of OCT and OCTA may serve as an alternative, but ICGA remains important for treatment decisions (e.g., whether to add PDT).
Advances in OCT and OCTA are making ICGA-independent diagnostic support possible, but at present, ICGA remains the gold standard. Although the APOIS criteria show high discriminative ability with an AUC of 0.90, ICGA is still an important test for treatment decisions (e.g., whether to add PDT). 5, 12)
According to the 2012 treatment guidelines by the Ministry of Health, Labour and Welfare research group, treatment selection based on visual acuity is recommended.
Good visual acuity (0.6 or better): Consider anti-VEGF monotherapy.
Visual acuity ≤ 0.5: Photodynamic therapy (PDT) alone or PDT + anti-VEGF combination therapy is recommended.
In PCV, regression of polypoidal lesions is related to recurrence after treatment. Ranibizumab achieved a polyp complete regression rate of 20–30%, while aflibercept achieved a higher rate of 40–50%. In recent years, VEGF inhibitor monotherapy has been increasingly used regardless of visual acuity. 9)
Aflibercept shows a higher polyp occlusion rate than ranibizumab. In the PLANET trial, comparing aflibercept monotherapy with aflibercept + PDT combination, non-inferiority of aflibercept monotherapy to PDT combination was demonstrated (1-year results). 9) The polyp occlusion rate reached over 85% even in the monotherapy group. 3, 9)
Vella et al. (2021) reported that in PCV cases unresponsive to six doses of ranibizumab, a single dose of aflibercept resulted in complete resolution of SRF (subretinal fluid). 3)
Irradiation size: lesion maximum diameter based on angiography findings + 1000 μm
Avoid direct sunlight for 2 days after treatment
In combination therapy of PDT and VEGF inhibitor, VEGF inhibitor may be administered before PDT (within 1 week) or on the same day as PDT (under light shielding).
In the EVEREST I trial, the lesion closure rate with PDT + ranibizumab combination or PDT alone was 77.8%, whereas ranibizumab alone was only 26.7%.10) In the EVEREST II trial (RCT), the PDT + ranibizumab group showed a 9.6-letter improvement in visual acuity at 24 weeks compared to the ranibizumab alone group.10)
As a minimally invasive alternative to PDT, the efficacy of 577 nm micropulse laser has been reported.
Jafar et al. (2024) reported a case of PCV treated with 577 nm micropulse laser (duty cycle 5%, 400 mW, 200 μm, 200 ms), with complete resolution of SRF at 12 weeks. Visual acuity improved from 20/60 to 20/25.2)
Cases with massive SMH may require vitrectomy for hematoma removal.5)
Sasajima et al. (2022) performed vitrectomy using tissue plasminogen activator (tPA 12.5 μg/0.05 mL) + SF6 gas 1.2 mL for rapidly progressive PCV (79-year-old male) after the third dose of COVID-19 vaccine. On postoperative day 13, reduction of SMH and SRF was observed. 4)
QWhich to choose: aflibercept or ranibizumab?
A
Aflibercept has a complete polyp regression rate of 40–50%, surpassing ranibizumab (20–30%). The PLANET trial also demonstrated non-inferiority of aflibercept monotherapy to PDT, and it is currently recommended as the first-line anti-VEGF agent for PCV. 3, 9)
Dilated large choroidal vessels (pachysessels) in the Haller layer are central to the pathology. 5) Anastomoses between the superior and inferior vortex veins are observed in approximately 90% of PSD eyes, leading to loss of the horizontal watershed zone. 5) This vortex vein stasis causes a stepwise progression: Haller layer dilation → thinning of the Sattler layer and choriocapillaris → capillary-level ischemia → formation of neovascular complexes. 5)
Chronic choroidal congestion leads to the following changes in a stepwise manner.
Metabolic impairment and dysfunction of the RPE
Structural destruction of Bruch’s membrane due to increased protease activity5)
Formation of abnormal branching vascular networks (BVN)
Appearance of polypoidal dilatations
The choroid lacks a capillary complex like the retina and is directly exposed to pulsatile blood flow. This makes the tips of CNV prone to dilate and form polyps.5) Additionally, choriocapillaris flow deficit (CCFD) is increased not only in eyes with PCV but also in healthy fellow eyes, suggesting that pachychoroid may act as a bilateral systemic predisposition.5)
Pachychoroid-type PCV tends to occur in younger patients, shows more CSC-like features, is associated with choroidal vascular hyperpermeability (CVH), and may exhibit resistance to anti-VEGF therapy.5, 8) In contrast, non-pachychoroid type (drusen-driven PCV) shows AMD-like features and is strongly associated with ARMS2/HTRA1 risk alleles.5, 8) Since the two types show different clinical courses and treatment responses, individualized treatment strategies are required.
Direct damage to the RPE and Bruch’s membrane due to inflammation can predispose to the development of PCV.1) In a case where PCV developed 20 years after tuberculous choroiditis, it is speculated that accumulation of tissue damage from chronic inflammation contributed to the onset of PCV.1)
7. Latest research and future perspectives (research-stage reports)
Brolucizumab (a high-affinity single-chain antibody to VEGF-A) has shown non-inferior visual acuity improvement and superior anatomical outcomes compared to existing anti-VEGF agents. 5) Along with faricimab (VEGF-A/Ang-2 dual inhibition), it is attracting attention as a candidate drug that enables treat-and-extend (T&E) dosing intervals. 6) Both are still awaiting accumulation of long-term data.
PDS, a sustained-release device for anti-VEGF drugs, is being developed as an alternative to frequent intravitreal injections. 5) It may help reduce the treatment burden for patients with nAMD, including PCV.
T&E is a regimen that extends the dosing interval based on individual recurrence risk after initial fixed dosing. 6) It is attracting attention for application in PCV patients, but the optimal protocol has not yet been established.
AI diagnosis based on OCT findings (APOIS criteria) has shown a discriminative ability for nAMD vs. PCV with an AUC of 0.90. 5, 12) The TIGER trial is investigating a new diagnostic and treatment response evaluation system using OCTA and AI. 5)
With the spread of the pachychoroid spectrum concept, debate continues on whether PCV should be considered a subtype of nAMD or an independent disease. 6, 8)Pachychoroid-type PCV and non-pachychoroid-type (drusen-driven) PCV have been shown to differ in choroidal thickness, treatment response, and long-term prognosis. 14) Refining treatment strategies to individually decide between anti-VEGF monotherapy or PDT combination after distinguishing these two types is a major future challenge.
The prognosis of PCV is closely related to the degree of polypoidal lesion regression. Complete polyp regression rates with aflibercept are 40–50%, exceeding the 20–30% with ranibizumab. 9) Cases with complete polyp regression have a lower risk of recurrence, but in cases with incomplete regression, reaccumulation of fluid occurs frequently, so regular imaging evaluation is essential.
Even after successful treatment and resolution of exudative changes, sudden massive submacular hemorrhage (SMH) due to polyp rupture can occur. The incidence of SMH over 5 years is reported to be approximately 10%. 5) Patients should be repeatedly instructed to seek immediate medical attention if visual symptoms change suddenly. Massive submacular hemorrhage involving the fovea has a poor visual prognosis and may require surgical intervention such as tPA with gas tamponade.
Pachychoroid-type PCV tends to be resistant to anti-VEGF therapy and often requires combination with PDT. 5, 8) On the other hand, non-pachychoroid (drusen-driven) type tends to follow a chronic progressive course similar to AMD and requires long-term maintenance therapy. 5, 8) Both subtypes have high recurrence rates, and it is important to continue regular OCT and ICGA evaluations even after treatment is completed.
Mohankumar A, Mohan S, Rajan M. Polypoidal choroidal vasculopathy 20 years after resolution of tubercular choroiditis. Digital journal of ophthalmology : DJO. 2023;29(3):94-96. doi:10.5693/djo.02.2023.07.003. PMID:37780035; PMCID:PMC10539005.
Jafar SM, Hussein ZR, Yasir MB. A case of treating polypoidal choroidal vasculopathy subretinal fluid by subthreshold micropulse laser. American journal of ophthalmology case reports. 2024;36:102225. doi:10.1016/j.ajoc.2024.102225. PMID:39691633; PMCID:PMC11650130.
Vella G, Sacconi R, Borrelli E, Bandello F, Querques G.. Polypoidal choroidal vasculopathy in a patient with early-onset large colloid drusen. Am J Ophthalmol Case Rep. 2021;22:101085. doi:10.1016/j.ajoc.2021.101085. PMID:33898862; PMCID:PMC8056241.
Sasajima H, Zako M, Maeda R, Ueta Y. Rapid Progression of Polypoidal Choroidal Vasculopathy following Third BNT162b2 mRNA Vaccination. Case reports in ophthalmology. 2022;13(2):459-464. doi:10.1159/000525151. PMID:35950020; PMCID:PMC9247562.
Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal Choroidal Vasculopathy: An Update on Diagnosis and Treatment. Clinical ophthalmology (Auckland, N.Z.). 2023;17:53-70. doi:10.2147/OPTH.S385827. PMID:36636621; PMCID:PMC9831529.
Cheung CMG, Dansingani KK, Koizumi H, et al. Pachychoroid disease: review and update. Eye (Lond). 2025;39(5):819-834. doi:10.1038/s41433-024-03253-4.
Koh AH, Expert PCV Panel, Chen LJ, Chen SJ, Chen Y, Giridhar A, Iida T, Kim H, Yuk Yau Lai T, Lee WK, Li X, Han Lim T, Ruamviboonsuk P, Sharma T, Tang S, Yuzawa M. Polypoidal choroidal vasculopathy: evidence-based guidelines for clinical diagnosis and treatment. Retina. 2013;33(4):686-716. doi:10.1097/iae.0b013e3182852446. PMID:23455233.
Cheung CMG, Lai TYY, Ruamviboonsuk P, Chen SJ, Chen Y, Freund KB, Gomi F, Koh AH, Lee WK, Wong TY.. Polypoidal Choroidal Vasculopathy: Definition, Pathogenesis, Diagnosis, and Management. Ophthalmology. 2018;125(5):708-724. doi:10.1016/j.ophtha.2017.11.019. PMID:29331556.
Lee WK, Iida T, Ogura Y, Chen SJ, Wong TY, Mitchell P, et al. Efficacy and Safety of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy in the PLANET Study: A Randomized Clinical Trial. JAMA ophthalmology. 2018;136(7):786-793. doi:10.1001/jamaophthalmol.2018.1804. PMID:29801063; PMCID:PMC6136040.
Lim TH, Lai TYY, Takahashi K, Wong TY, Chen LJ, Ruamviboonsuk P, Tan CS, Lee WK, Cheung CMG, Ngah NF, Patalauskaite R, Margaron P, Koh A, EVEREST II Study Group.. Comparison of Ranibizumab With or Without Verteporfin Photodynamic Therapy for Polypoidal Choroidal Vasculopathy: The EVEREST II Randomized Clinical Trial. JAMA Ophthalmol. 2020;138(9):935-942. doi:10.1001/jamaophthalmol.2020.2443. PMID:32672800; PMCID:PMC7366282.
Voraporn Chaikitmongkol, Chui Ming Gemmy Cheung, Hideki Koizumi, Vishal Govindahar, Jay Chhablani, Timothy Y.Y. Lai. Latest Developments in Polypoidal Choroidal Vasculopathy: Epidemiology, Etiology, Diagnosis, and Treatment. Asia-Pacific Journal of Ophthalmology. 2020;9(3):260-268. doi:10.1097/01.apo.0000656992.00746.48.
Chong Teo KY, Sadda SR, Gemmy Cheung CM, Chakravarthy U, Staurenghi G, Invernizzi A, et al. Non-ICGA treatment criteria for Suboptimal Anti-VEGF Response for Polypoidal Choroidal Vasculopathy: APOIS PCV Workgroup Report 2. Ophthalmology. Retina. 2021;5(10):945-953. doi:10.1016/j.oret.2021.04.002. PMID:33866022.
Dansingani KK, Balaratnasingam C, Nishi K, et al. Understanding aneurysmal type 1 neovascularization (polypoidal choroidal vasculopathy): a lesson in the taxonomy of ‘expanded spectra’ — a review. Prog Retin Eye Res. 2018;65:89-117.
Miyake M, Ooto S, Yamashiro K, Takahashi A, Yoshikawa M, Akagi-Kurashige Y, Ueda-Arakawa N, Oishi A, Nakanishi H, Tamura H, Tsujikawa A, Yoshimura N.. Pachychoroid neovasculopathy and age-related macular degeneration. Sci Rep. 2015;5:16204. doi:10.1038/srep16204. PMID:26542071; PMCID:PMC4635432.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.