Choroidal rupture is a condition in which the choriocapillaris, Bruch’s membrane, and retinal pigment epithelium (RPE) are torn due to non-penetrating (closed) blunt trauma to the eye. The sclera withstands the tensile strength, but the less elastic Bruch’s membrane breaks, causing the rupture.
In a retrospective study of 101 patients, the average age was 36 years, and 76% were male. Closed eye injuries are three times more common than open injuries.
The main mechanisms of injury are as follows:
Sports injuries: martial arts, basketball, soccer, tennis, golf, etc.
Traffic injuries: eye contusion from airbag deployment
Other blunt trauma: fist blows, falls, etc.
The distribution of rupture sites is reported as: fovea 30%, extrafoveal macula 45%, extramacular 25%.
QCan choroidal rupture occur without trauma?
A
It is usually caused by blunt ocular trauma. However, in systemic diseases that increase the fragility of Bruch’s membrane (such as pseudoxanthoma elasticum, Ehlers-Danlos syndrome, angioid streaks, etc.), rupture can occur even with minor trauma.
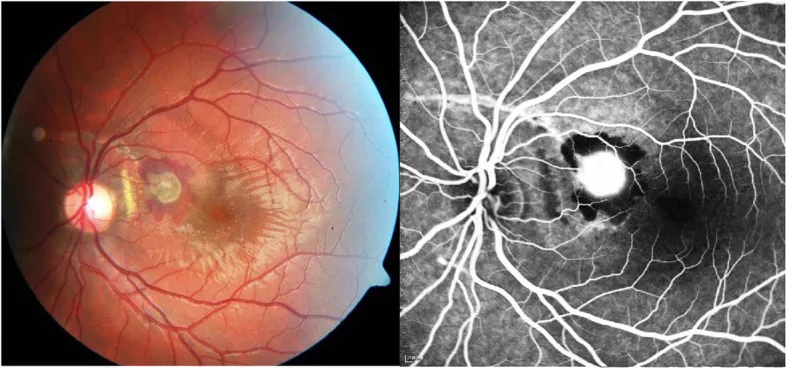
Barth T, et al. Intravitreal anti-VEGF treatment for choroidal neovascularization secondary to traumatic choroidal rupture. BMC Ophthalmol. 2019. Figure 1. PMCID: PMC6878647. License: CC BY.
In the left eye of a 19-year-old male, an arcuate choroidal rupture crossing above the optic disc, choroidal neovascularization (CNV) near the macula, and subretinal hemorrhage are observed. This corresponds to the choroidal rupture discussed in the section “2. Main Symptoms and Clinical Findings.”
Decreased visual acuity: Occurs when the rupture line extends to the fovea. The effect of hemorrhage also contributes.
Metamorphopsia: Caused by macular hemorrhage or rupture involving the macula.
Asymptomatic: If the rupture is confined to the periphery, subjective symptoms may be absent.
For several days to weeks after injury, the rupture line is often hidden by hemorrhage, making it difficult to confirm on fundus examination. Clear findings are obtained only after the hemorrhage is absorbed.
QIs it possible that choroidal rupture is not found immediately after injury?
A
Yes. Immediately after injury, choroidal hemorrhage and subretinal hemorrhage often cover the rupture line, making it difficult to confirm on fundus examination. After several days to weeks, as the hemorrhage is absorbed, it can be seen as a white to yellowish-white streak.
OCT reveals a break in the inner choroidal layers including Bruch’s membrane and loss of RPE continuity. The neurosensory retina overlying the rupture site is often preserved.
The cause of choroidal rupture is almost always non-penetrating blunt ocular trauma. The following systemic diseases increase the fragility of Bruch’s membrane, making rupture more likely even with minor trauma.
Caution is needed for Bruch’s membrane fragility in the following diseases:
QIs there a way to prevent choroidal rupture when playing sports?
A
Wearing polycarbonate protective glasses (sports eye guards) is effective. Polycarbonate has higher impact resistance than regular plastic lenses and prevents direct eye trauma.
Diagnosis is based on a combination of history of ocular trauma and characteristic fundus findings. Immediately after injury, examination may be difficult due to bleeding, so re-examination after the bleeding is absorbed is important.
Dilated fundus examination: Confirm a crescent-shaped white to yellowish-white line. Re-examine after hemorrhage absorption if performed immediately after injury.
Fluorescein angiography (FA): The rupture site shows hypofluorescence in the early phase and staining in the late phase. If CNV is present, hyperfluorescence increases, making this test essential for CNV detection.
Fundus autofluorescence (FAF): The RPE defect area shows hypofluorescence, while the edge of the rupture shows hyperfluorescence. Useful for assessing the extent of the rupture.
OCT: Can confirm loss of RPE continuity and thinning of the inner choroid. Also useful for evaluating CNV activity.
Ocular ultrasound: Depicted as a dome-shaped elevation of choroidal hemorrhage. Used as an adjunctive diagnostic tool when fundus observation is difficult.
There is no drug therapy or surgical procedure to heal choroidal rupture itself. The basic approach is observation, waiting for spontaneous absorption of choroidal hemorrhage (weeks to months).
Choroidal neovascularization (CNV) occurs in about 5-10% of choroidal rupture cases after blunt trauma. Older age, rupture involving the fovea, and long rupture length (especially ≥4000 μm) are reported as independent risk factors. The average time from injury to CNV diagnosis is about 5.7 months, and most cases develop within 1 year. Traumatic CNV typically occurs as type 2 and may be accompanied by serous or hemorrhagic pigment epithelial detachment. When CNV is confirmed, the following treatments are performed.
Anti-VEGF Injection
First-line treatment: Intravitreal injection of anti-VEGF agents is the first-line treatment for traumatic CNV.
Agents: Ranibizumab, aflibercept, bevacizumab, etc. are used.
Other Treatments
Laser photocoagulation: Indicated for choroidal neovascularization in the macula located more than 200 μm from the fovea. It is difficult to perform when close to the fovea.
Observation only: If the CNV is small and distant from the fovea, observation may be an option.
QIf CNV occurs, can treatment improve it?
A
Intravitreal injection of anti-VEGF drugs is the first choice, and traumatic CNV tends to be controlled with fewer injections (average 4.2 injections) compared to age-related macular degeneration. However, if the fovea is already damaged, complete recovery of vision may be difficult.
When the eye is compressed from the front, the tissue around the firmly fixed optic disc is pushed backward, creating circular stress centered on the disc. The choroid has relatively poor extensibility, and this mechanical action often causes circumferential rupture in the posterior pole, especially around the optic disc. The reactions of each tissue are as follows:
Sclera: High tensile strength, withstands external force.
Retina: Has elasticity and can adapt to deformation.
Bruch’s membrane: Due to insufficient tensile strength and elasticity, it ruptures upon rapid overstretching.
Direct Rupture
Location: The fundus around the site of direct impact (mainly temporal side).
Morphology: Linear fissure parallel to the ora serrata.
Frequency: Less common than indirect rupture.
Indirect Rupture
Location: Occurs at the posterior pole due to countercoup effect, opposite the impact site.
Morphology: Arcuate to crescent-shaped striae concentric with the optic disc.
Ament CS, Zacks DN, Lane AM, Krzystolik M, D’Amico DJ, Mukai S, Young LH, Loewenstein J, Arroyo J, Miller JW. Predictors of visual outcome and choroidal neovascular membrane formation after traumatic choroidal rupture. Arch Ophthalmol. 2006;124(7):957-966. PMID: 16832018
Lupidi M, Muzi A, Castellucci G, Kalra G, Cardillo Piccolino F, Chhablani J, Cagini C. The choroidal rupture: current concepts and insights. Surv Ophthalmol. 2021;66(5):761-770. PMID: 33545177
Singh S, Saxena S. Unraveling the perplexities of choroidal rupture. Indian J Ophthalmol. 2023;71(6):2326-2327. PMID: 37322692 / PMCID: PMC10417958
Raman SV, Desai UR, Anderson S, Samuel MA. Visual prognosis in patients with traumatic choroidal rupture. Can J Ophthalmol. 2004;39(3):260-266. PMID: 15180143
Arthur A, Rajasekaran NM, Kuriakose T. A reappraisal of indirect choroidal rupture using swept-source optical coherence tomography in-vivo pathology images in patients with blunt eye trauma. Indian J Ophthalmol. 2020;68(11):2469-2473. PMID: 32971624 / PMCID: PMC7728025
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.