Mild Grade 1-2
Grade 1 (EZ hyperreflectivity): EZ hyperreflectivity is present but structure is preserved. Visual prognosis is relatively good.
Grade 2 (IZ loss): IZ reflectivity is lost. Indicates moderate photoreceptor outer segment damage.

Commotio retinae is a reversible lesion caused by blunt ocular trauma, leading to disruption and edema of photoreceptor outer segments and retinal pigment epithelium (RPE) cells. The main finding is white retinal opacification, which often resolves spontaneously.
When the macula is involved, it is characterized by a cherry-red spot-like appearance at the fovea surrounded by white opacification, and is also called Berlin edema (Berlin opacity). In contrast, irreversible damage is termed retinal contusion necrosis.
It is a relatively common condition, occurring in about 30% of closed globe injuries. It can result from direct impact (coup injury) or from shock waves transmitted to the opposite side (contrecoup injury).
Berlin edema is the term used for commotio retinae occurring in the macula. It presents with a characteristic appearance: the fovea looks like a cherry-red spot surrounded by white opacification. Commotio retinae can occur outside the macula and is a broader disease concept.
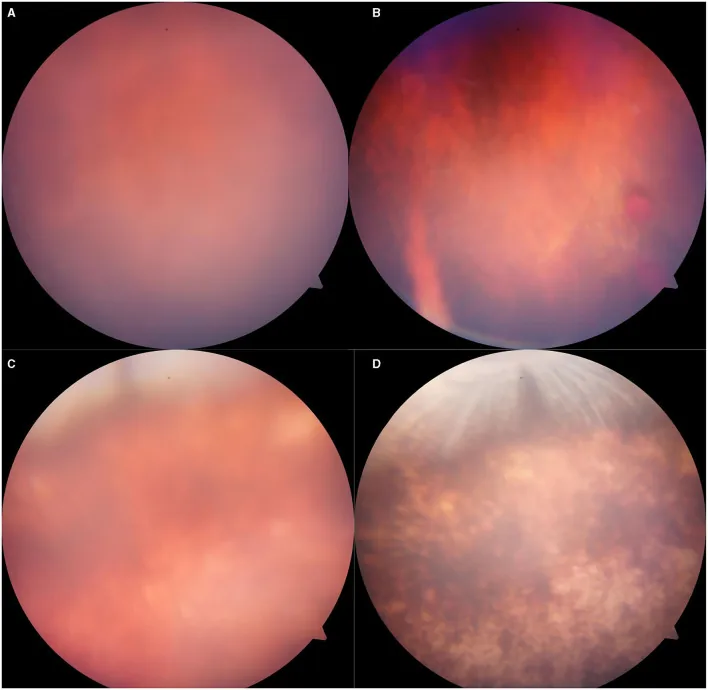
Fundus examination reveals characteristic shiny, small patchy to geographic white opacities. Opacities appear immediately after injury, peak at 2–3 days, and resolve over 1–2 weeks. Usually no hemorrhage.
In macular lesions (Berlin’s edema), a cherry-red spot-like appearance occurs due to relative redness of the fovea, with prominent contrast against the surrounding white opacities.
OCT typically shows hyperreflectivity and thickening of the ellipsoid zone (EZ) and disruption of the interdigitation zone (IZ). The OCT grading by Ahn et al. is useful for prognosis. 1)
Mild Grade 1-2
Grade 1 (EZ hyperreflectivity): EZ hyperreflectivity is present but structure is preserved. Visual prognosis is relatively good.
Grade 2 (IZ loss): IZ reflectivity is lost. Indicates moderate photoreceptor outer segment damage.
Severe Grade 3-4
Grade 3 (IZ+EZ loss): Both IZ and EZ are lost. Visual prognosis tends to be poor.
Grade 4 (IZ+EZ+ELM loss): The most severe type, with loss up to the external limiting membrane (ELM). Visual prognosis is the poorest.
OCTA may help assess changes in macular vascular density. Also, choroidal thickening may be present in the early stages of injury.
Commotio retinae is caused by closed ocular trauma or blast injury.
It is recommended to choose polycarbonate lenses according to the impact level. For low to medium impact, 2–3 mm thickness is appropriate; for high impact, 3 mm or more. For highest-risk sports such as ice hockey and lacrosse, a helmet with a face mask is suitable. Regular eyeglass lenses are insufficient as protective gear, so dedicated protective eyewear should be used.
Dilated fundus examination is the standard. Diagnosis is often relatively easy due to the characteristic finding of a shiny white opacity.
In trauma examination, it is important to simultaneously check for intraocular complications other than retinal ones.
In post-traumatic retinal whitening, the following differential diagnoses are important.
The table below shows the main differentiating points between commotio retinae and retinal contusion necrosis.
| Feature | Commotio Retinae | Contusion Necrosis |
|---|---|---|
| Opacity appearance | Shiny white | Dense white |
| Hemorrhage | None | Present |
| Prognosis | Spontaneous resolution | Irreversible |
Other differential diagnoses include the following.
Currently, there is no established treatment with proven efficacy for commotio retinae. The opacities usually resolve spontaneously, and observation is the basic management.
White opacities often resolve spontaneously within 1 to 2 weeks after injury. Improvement in OCT findings may continue for several months thereafter.
There are anecdotal reports of high-dose intravenous steroid administration, but its efficacy is not established and it is not currently recommended as standard treatment.
The most important aspect of observation is detection and management of complications.
An ophthalmological examination is essential. Commotio retinae itself often resolves spontaneously, but complications such as retinal tears, macular holes, angle damage, and lens dislocation may also occur. Missing these can lead to permanent visual impairment or visual field defects. In particular, regular follow-up after injury is directly linked to early detection of complications.
Blunt impact to the eye applies mechanical stress to the retina through the following mechanisms:
Contrecoup injury occurs when the shock wave passes through the eyeball and reaches the opposite retina.
Mansour et al. confirmed destruction of photoreceptor outer segments and accumulation of subretinal debris in donor eyes processed within 24 hours after injury2).
The glossy white opacity of the fundus results from abnormal light scattering caused by disrupted outer segments and debris. The essence is physical disruption of outer segment structures, not fluid accumulation (edema) within the tissue.
Repair of outer segments begins approximately 1 week after injury. Complete recovery may take more than 2 months.
In normal photoreceptor outer segments, there are 1,000–2,000 disc membranes, and about 10% of the distal outer segment is phagocytosed by the retinal pigment epithelium daily for renewal. This turnover cycle renews the entire outer segment in about 10–14 days. This physiological outer segment renewal mechanism is thought to underlie the natural resolution after trauma.
OCTA may be useful as a non-invasive follow-up tool. However, the clinical significance of prognostic prediction in commotio retinae requires further investigation.
The OCT grading system by Ahn et al. has attracted attention as a tool for predicting visual prognosis from acute-phase findings. 1) In particular, identification of severe cases (Grade 3–4) is thought to help determine the need for early intensive follow-up. Validation through future multicenter prospective studies is required.
Changes in choroidal blood flow after blunt trauma may contribute to dysfunction of the retinal pigment epithelium and photoreceptor outer segments. This hypothesis is useful for understanding the pathophysiology, but it has not yet been established as a therapeutic target.