In 1910, Otmar Purtscher first reported it in a middle-aged patient with head trauma from a fall from a tree. It is a rare disease, a retinal vascular occlusive disease associated with trauma. It is classified as a remote traumatic retinopathy caused by trauma to areas other than the eye, such as head, neck, or chest contusions.
Similar conditions associated with systemic diseases, surgical procedures such as retrobulbar anesthesia, acute pancreatitis, thrombotic thrombocytopenic purpura, renal failure, or connective tissue disease are distinguished as Purtscher-like retinopathy. Fundus findings are common to both, and the pathophysiology is similar.
The estimated incidence is 0.24 per million per year, with possible underreporting4)6). About 60% are bilateral, and occasionally unilateral cases occur. When caused by acute pancreatitis, almost all cases are bilateral. Lesions are confined to the posterior pole (peripapillary and macular area) in 83–92% of cases. Trauma is the most frequent cause, followed by acute pancreatitis.
The causes of Purtscher-like retinopathy are diverse. In addition to acute pancreatitis, renal failure, collagen disease, pregnancy-induced hypertension/HELLP syndrome, fat embolism syndrome, Valsalva maneuver, hemolytic uremic syndrome, shaken baby syndrome, retrobulbar anesthesia, and steroid injections, cases have been reported in recent years due to COVID-19 infection1)9), hypertensive emergency2), filler injection3), ischemic colitis4), vaccination5), and C3 glomerulopathy8).
QWhat is the difference between Purtscher retinopathy and Purtscher-like retinopathy?
A
Cases caused by trauma such as head injury, chest compression, or long bone fracture are called Purtscher retinopathy. Cases caused by systemic diseases without trauma, such as acute pancreatitis or renal failure, are called Purtscher-like retinopathy. The fundus findings are common to both, and the treatment strategy is the same.
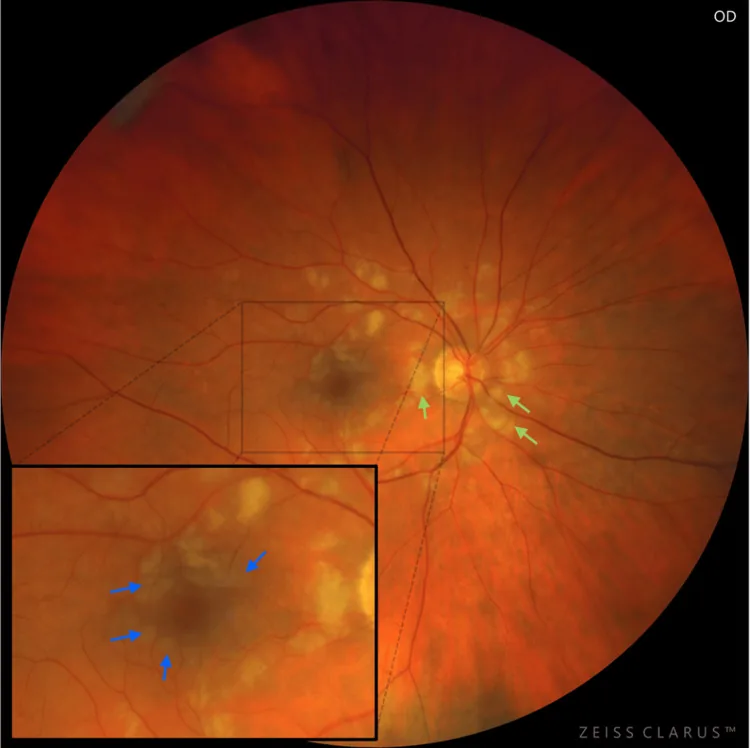
Skulimowski B, Liberski S, Nikratowicz D, Gotz-Wieckowska A. Purtscher-Like Retinopathy Secondary to an Appendiceal Neuroendocrine Neoplasm Complicated by a Periappendiceal Abscess. Cureus. 2025;17(6):e85752. Figure 1. PMCID: PMC12247013. License: CC BY.
Fundus photograph of the right eye shows polygonal Purtscher flecken (blue arrows: retinal inner layer whitening with borders within 50 μm of vessels and a clear area adjacent to vessels = perivascular sparing) centered on the macula, and the optic disc and vascular arcades are surrounded by cotton-wool spots (CWS) (green arrows). This corresponds to the typical posterior pole fundus findings of Purtscher flecken and cotton-wool spots discussed in the section “2. Main Symptoms and Clinical Findings.”
Visual impairment develops hours to days after the onset of trauma or related disease. The degree of visual impairment varies from very mild to hand motion vision. Visual field defects may also occur, presenting as central scotoma, paracentral scotoma, or arcuate scotoma.
Painless vision loss: The most important clinical symptom. It appears simultaneously with the event or after a delay of several hours to several days4).
Degree of vision loss: Varies from very mild to hand motion vision.
Visual field defects: Accompanied by central scotoma, paracentral scotoma, or arcuate scotoma, but peripheral vision is usually preserved.
Findings localized to the posterior pole (peripapillary and macular area) are characteristic.
Purtscher flecken
Shape: Polygonal, well-demarcated whitening.
Location: Inner retinal layers between arterioles and venules. Seen around retinal arteries.
Border: Clear border within 50 μm from the vessel. Perivascular sparing, where the retina around the vessel remains clear, is typical.
Frequency: Observed in about 63% of cases.
Pathophysiology: Inner retinal whitening due to precapillary arteriolar occlusion in the capillary bed.
Soft Exudate (Cotton-Wool Spot)
Shape: Fluffy white patch with indistinct borders.
Location: Focal infarction within the nerve fiber layer (NFL). Common around the optic disc.
Border: Indistinct and irregular.
Frequency: The most common finding, observed in 93% of cases.
Pathophysiology: Due to microinfarction within the NFL.
Intraretinal hemorrhage: Seen in 80–90% of cases. Takes various forms such as flame-shaped, blot-shaped, and dot-shaped.
Pseudo-cherry-red spot: The fovea appears as a small round red spot compared to the surrounding retina, similar to the cherry-red spot in central retinal artery occlusion (CRAO), but in this disease it is a “pseudo” cherry-red spot. Differentiation is necessary.
Macular edema / serous retinal detachment: Observed in some cases.
Retinal venous dilation and tortuosity / optic disc edema: May be associated.
Lesions are classified into three zones (A, B, C) based on the extent of involvement. Two-thirds of cases involve only zone A, and zone C involvement is rare.
At the 2-month follow-up after onset, the following findings have been reported: normal fundus in 40%, optic atrophy in 64%, RPE mottling in 23%, retinal thinning in 14%, and retinal artery narrowing in 4%. Optic atrophy and retinal atrophy may persist.
QWhen do symptoms appear? Immediately after trauma?
A
Vision loss often occurs not immediately after trauma or systemic disease onset, but after a delay of several hours to several days. There is no eye pain. If vision gradually worsens after trauma, this condition should be considered.
Head trauma: The oldest known cause. Traffic accidents, falls, blows, etc.
Chest compression: A sudden increase in intrathoracic pressure due to strong compressive trauma. Crush syndrome, chest crush by heavy objects.
Long bone fracture: Can develop due to fat embolism syndrome.
Purtscher-like retinopathy (non-traumatic)
Acute pancreatitis: The most frequent non-traumatic cause. Almost always bilateral.
Renal failure / C3 glomerulopathy: Activation of the alternative complement pathway is involved 6)8).
COVID-19 infection: Can develop even in mild cases due to complement activation and coagulation abnormalities 1)9).
Valsalva maneuver / defecation: Venous return disturbance due to increased intrathoracic pressure 7).
Other non-traumatic causes include collagen diseases / connective tissue diseases (SLE, dermatomyositis, scleroderma), pregnancy-induced hypertension / HELLP syndrome, fat embolism syndrome, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, childbirth (amniotic fluid embolism), retrobulbar anesthesia, and shaken baby syndrome. In recent years, cases have also been reported after filler injection (including non-facial) 3), ischemic colitis 4), and after herpes zoster vaccine (Shingrix) administration 5).
QCan COVID-19 infection also cause Purtscher-like retinopathy?
A
It has been reported that even mild COVID-19 can cause retinal microvascular occlusion due to complement activation and coagulation abnormalities, leading to Purtscher-like retinopathy 1). A mechanism by which high concentrations of C5a due to cytokine storm promote thrombus formation has also been considered 9).
Agrawal et al. criteria require all of the following: ① presence of associated disease, ② unilateral/bilateral Purtscher flecken and/or superficial CWS, ③ limitation to the posterior pole, ④ no direct ocular trauma, ⑤ no emboli in retinal vessels, ⑥ minimal hemorrhage.
Miguel’s updated criteria (3 or more of 5 criteria) are shown below4).
Criterion
Description
Criterion 1
Presence of Purtscher flecken
Criterion 2
Few to moderate retinal hemorrhages
Criterion 3
Soft exudates (limited to posterior pole)
Criterion 4
Presence of an explainable etiology
Criterion 5
Complementary examination findings consistent with the diagnosis
Fundus examination: First choice. Confirm white spots, hemorrhages, and Purtscher flecken in the posterior pole.
FA (Fluorescein angiography): Obstruction due to emboli in retinal arterioles and capillaries is observed. Delayed leakage of contrast agent in the late phase and fluorescence leakage from the optic nerve are characteristic. Choroidal hypofluorescence may persist up to 5 months after diagnosis. ICGA also shows hypofluorescence, suggesting involvement of the choroidal vasculature.
OCT: In the acute phase, hyperreflectivity of the inner retinal layers and macular edema are observed. As a PAMM (paracentral acute middle maculopathy) finding, a hyperreflective band in the inner nuclear layer (INL) may be seen on SD-OCT, indicating involvement of deep and intermediate retinal capillaries 2)3)5). In the late phase, atrophy of the outer retinal layers and loss of photoreceptors occur, which is important for prognosis.
mfERG (multifocal electroretinogram): Reduced amplitudes of both a-wave and b-wave are observed. This provides evidence of involvement of both outer and inner retinal layers.
Central retinal artery occlusion (CRAO): Differentiated by the presence of intravascular emboli. Cherry-red spot is genuine, but in this disease it is a pseudo-cherry-red spot.
Commotio retinae (retinal concussion): Localized circulatory disturbance due to blunt ocular trauma presents with well-demarcated white lesions. It differs in that direct ocular trauma is the trigger.
QHow to distinguish Purtscher flecken from soft exudates?
A
Purtscher flecken are polygonal, occur in the capillary bed between arterioles and venules, and have clear borders within 50 μm of the vessel. Soft exudates are fluffy white spots with indistinct borders, caused by focal infarction in the NFL 2). Both may coexist in the same fundus.
There are no evidence-based treatment guidelines. Most cases are managed with observation, but steroid therapy may be used in some cases. Treatment of the underlying disease (e.g., acute pancreatitis, fractures) is the highest priority.
Even without treatment, many cases resolve within a few months. Steroid therapy, antiplatelet therapy, and fibrinolytic therapy are sometimes used, but their effectiveness is unknown. A systematic review by Miguel et al. found no significant difference in visual improvement between the high-dose steroid group and the untreated group. A systematic review by Xia et al. (2017) also reported no difference in visual improvement with glucocorticoid therapy 4)5). Lesions tend to resolve spontaneously within 1 to 3 months 4).
High-dose intravenous steroids are the most commonly reported treatment, but evidence from prospective trials is not established. Mechanisms include stabilization of damaged neural membranes and microvascular channels, and suppression of granulocyte aggregation and complement activation. Case reports have used a tapering dose starting from prednisolone 60 mg 1)6).
Multiple systematic reviews have shown no significant difference in visual improvement between steroid-treated and untreated groups4)5). Treatment of the underlying disease is the highest priority, and lesions tend to resolve spontaneously within 1–3 months. The efficacy of steroid therapy, antiplatelet therapy, and fibrinolytic therapy is unknown, and evidence from prospective trials has not been established.
The main etiology is occlusion due to embolism of retinal arteriolar precapillaries. Damage to the vascular endothelium by multiple factors is involved in the pathogenesis.
The following mechanisms are hypothesized for Purtscher’s traumatic retinopathy:
Venous reflux due to neck/chest compression: Causes damage to venous and capillary endothelium.
Increased cavernous sinus pressure: Causes damage to venous and capillary endothelium due to increased venous pressure.
Reflex retinal arteriolar spasm: Causes damage to arterial and capillary endothelium.
Embolism: In fractures, fat; in chest trauma, air; in acute pancreatitis, leukocyte emboli.
The type of embolus varies depending on the causative disease. Fat (long bone fractures), pancreatic proteases (acute pancreatitis), leukocyte aggregation (leukoembolization), air, platelets, and fibrin have been reported.
Findings vary depending on embolus size. Large emboli cause confluent whitening similar to branch retinal artery occlusion, small ones cause soft exudates, and intermediate ones cause Purtscher flecken.
Activation of C5 and complement plays an important role with secondary lymphatic leakage. A pathway of complement activation → leukocyte aggregation (up to 50 μm) → precapillary occlusion has been suggested5)8).
Purtscher flecken are caused by occlusion of precapillary arterioles approximately 45 μm in diameter. A clear zone corresponding to the capillary-free area of 50 μm on both sides of retinal arteries and arterioles is formed.
Data are scarce. In a fatal case of acute pancreatitis reported by Kincaid et al., localized edema, cystic spaces, and disruption of normal structure were observed in the inner retina. Proteinaceous material (presumed recanalized thrombus) was found in the arteriolar lumen, with loss of photoreceptor outer segments, but the RPE and choroid were normal.
7. Latest research and future perspectives (research-stage reports)
There is a case report showing the efficacy of eculizumab (C5 inhibitor) in Purtscher-like retinopathy associated with atypical hemolytic uremic syndrome 8). Based on the common pathophysiology of C3 glomerulopathy and complement dysregulation, its potential application in treating Purtscher-like retinopathy has been suggested.
Teru et al. (2025) first reported Purtscher-like retinopathy after acute ischemic colitis 4). A 72-year-old woman developed bilateral vision loss the day after hospitalization for abdominal pain and bloody stools. It improved spontaneously two weeks later with only treatment for colitis (metronidazole and ciprofloxacin).
Pee et al. (2023) reported the first case of Purtscher-like retinopathy and PAMM complicated by bilateral CF, alveolar hemorrhage, and cerebral infarction after injection of approximately 500 mL of breast hyaluronic acid filler 3). SD-OCT showed hyperreflective bands in the inner nuclear layer, and inner retinal disorganization persisted at 10 months.
Application of OCTA (Optical Coherence Tomography Angiography)
Shroff et al. (2022) reported a case of unilateral Purtscher-like retinopathy after COVID-19 in which SS-OCTA revealed vascular dropout and flow deficits 9). It was shown that acute-phase flow deficits persist into the chronic phase, and OCTA is attracting attention as a tool for quantitatively assessing vessel density in the superficial and deep capillary plexuses.
Research is progressing on the correlation between acute-phase OCT findings (extent, severity, and depth of inner layer hyperreflectivity) and long-term visual function prognosis. It has been reported that the extent of inner layer atrophy and thinning of the macular ganglion cell layer may be indicators of poor prognosis, and the construction of an objective prognostic prediction model using OCT is expected.
Kalavar M, El Khatib B, Suelves AM, Yanoga F.. Purtscher-like retinopathy in patients with COVID-19. Am J Ophthalmol Case Rep. 2023;32:101915. doi:10.1016/j.ajoc.2023.101915. PMID:37663997; PMCID:PMC10474068.
Woodward R, Zheng Y, Fekrat S.. Asymmetric Purtscher-Like Retinopathy Caused by a Hypertensive Emergency and Undiagnosed Type 2 Diabetes. J Vitreoretin Dis. 2023;7(5):459-462. doi:10.1177/24741264231177130. PMID:37706084; PMCID:PMC10496805.
Pee XK, Low A, Ab Kahar MEPI, Mohamed SO, Chong YJ.. Purtscher-like retinopathy and paracentral acute middle maculopathy following breast filler injection. BMC Ophthalmol. 2023;23(1):444. doi:10.1186/s12886-023-03186-8. PMID:37932684; PMCID:PMC10629129.
Teru S, Christensen CA, Brown J. Purtscher-Like Retinopathy After Acute Ischemic Colitis. Journal of vitreoretinal diseases. 2025;9(4):523-526. doi:10.1177/24741264251338038. PMID:40330082; PMCID:PMC12049366.
Anderson HE, Sood S, Golshani C. Acute Unilateral Vision Loss Following Recombinant Zoster (Shingrix) Vaccination: A Case of Presumptive Purtscher-Like Retinopathy. Journal of vitreoretinal diseases. 2026. doi:10.1177/24741264261418512. PMID:41631100; PMCID:PMC12861412.
Pinto C, Fernandes T, Gouveia P, Sousa K.. Purtscher-like retinopathy: Ocular findings in a young woman with chronic kidney disease. Am J Ophthalmol Case Rep. 2022;25:101301. doi:10.1016/j.ajoc.2022.101301. PMID:35146191; PMCID:PMC8801352.
Sokol JT, Castillejos A, Sobrin L.. Purtscher-like retinopathy following a bowel movement. Am J Ophthalmol Case Rep. 2022;26:101560. doi:10.1016/j.ajoc.2022.101560. PMID:35572612; PMCID:PMC9092188.
Zaidi M, Mishra K, Nguyen HV, Miller PP, Ghoraba H, Karaca I, Matsumiya W, Nguyen QD, Leung LB.. C3 glomerulopathy associated with both hypertensive retinopathy and purtscher-like retinopathy. Am J Ophthalmol Case Rep. 2022;27:101683. doi:10.1016/j.ajoc.2022.101683. PMID:36016724; PMCID:PMC9395975.
Shroff D, Kumar S, Naidu A, Gupta C.. Unilateral Purtscher-like retinopathy post-COVID-19. Indian J Ophthalmol. 2022;70(10):3710-3712. doi:10.4103/ijo.ijo_1486_22. PMID:36190079; PMCID:PMC9789798.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.