Laser eye injury (retinal damage) refers to eye injuries caused by laser light irradiating the eyeball, resulting in damage to various tissues such as the cornea, lens, vitreous body, retina, choroid, and iris. It is continuous with the concept of photic maculopathy, with acute retinal damage due to excessive light exposure being its core.
Cosmetic lasers are based on the principle of selective photothermolysis. This principle selectively destroys target chromophores using light of specific wavelengths. The main target chromophores are melanin, hemoglobin, and water. Since these chromophores are abundant in the eye, melanin in the retinal pigment epithelium and iris, hemoglobin in blood vessels, and water in the cornea and lens absorb laser light and suffer secondary damage.
Light sources causing laser eye injuries are broadly classified into the following four categories.
Cosmetic lasers: Alexandrite (755 nm), diode (800–810 nm), Nd:YAG (1,064 nm), and CO2 (10,600 nm) lasers used for hair removal, tattoo removal, and facial resurfacing.
Laser pointers: Accidental or intentional irradiation by high-power devices (green 532 nm; Class 3B and Class 4) that have become widespread in recent years.
Medical lasers: Accidental irradiation of surgeons or patients during retinal photocoagulation, selective laser trabeculoplasty (SLT), or YAG laser posterior capsulotomy.
Industrial and military lasers: Occupational accidents involving industrial cutting lasers or military target designation lasers.
Based on international standards IEC 60825 and JIS C 6802, lasers are classified from Class 1 (safe) to Class 4 (highest risk). For Class 3B and above, direct eye exposure can cause instantaneous retinal damage. Some green laser pointers are equivalent to Class 3B or Class 4, and even a few seconds of exposure can cause irreversible sensory retinal damage.
In recent years, eye injuries from high-power green laser pointers (532 nm) have been increasing. The spread of cosmetic lasers has also contributed to the number of accidental exposure incidents. In a study of 40 people who sustained eye injuries, the rate of protective eyewear use was only 15% 1). The circulation of overseas products that do not meet JIS standards is also considered a factor in the increase in accidents.
QCan a laser pointer cause blindness?
A
High-power laser pointers equivalent to Class 3B or Class 4 (especially green 532 nm) pose a risk of instantly burning the retina if directed into the eye. According to the IEC 60825 safety classification, lasers of Class 3B and above are known to cause retinal damage upon direct exposure. In severe cases, central scotoma may persist, leading to substantial vision loss (blindness). Even commercially available laser pointers with high output are dangerous, and direct eye exposure should be absolutely avoided.
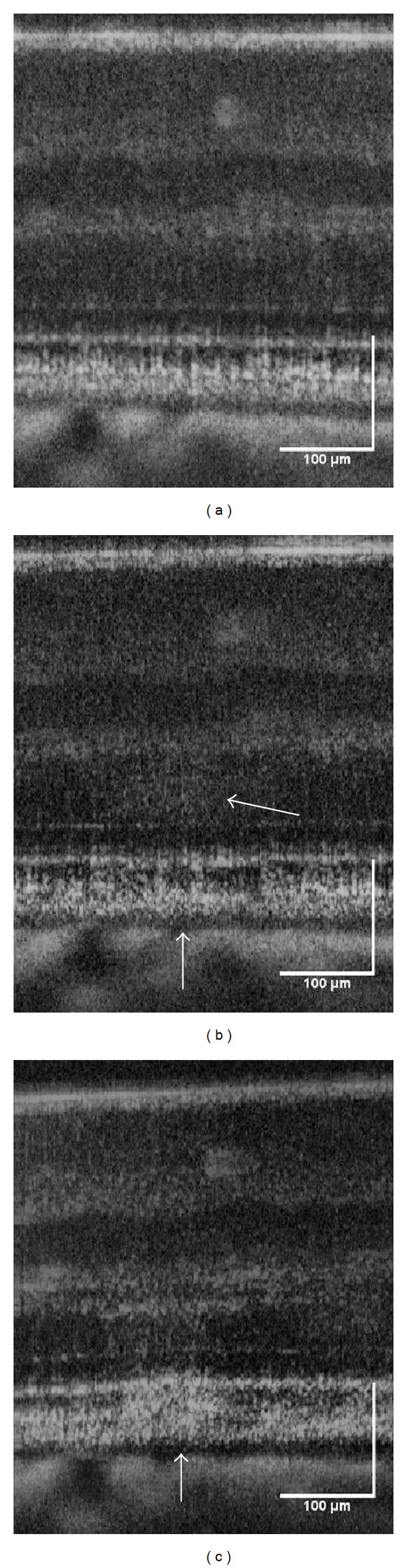
Pocock GM, Oliver JW, Specht CS, et al. High-resolution in vivo imaging of regimes of laser damage to the primate retina. J Ophthalmol. 2014;2014:516854. Figure 3. PMCID: PMC4033483. License: CC BY.
OCT B-scans before (a), approximately 10 seconds after (b), and a few minutes after (c) exposure to high-energy laser (870 mJ/cm²), showing the formation of retinal damage with increased hyperreflectivity and edema at the lesion indicated by white arrows after exposure. This corresponds to the retinal hyperreflective lesions and SD-OCT findings after photothermal damage discussed in the section “2. Main symptoms and clinical findings.”
The time course of symptom onset after laser eye injury varies depending on the damage mechanism. In the thermal type (high-power short-duration exposure), subjective symptoms and coagulation spots in the macula appear immediately after injury. In the photochemical type (low-power long-duration exposure), there is no abnormality immediately after exposure, and vision loss and macular degeneration become apparent several days later. The main subjective symptoms are as follows.
Visual abnormalities: decreased vision, blurring, central scotoma, metamorphopsia. These are the most common complaints.
Eye pain or discomfort: Often felt during the procedure or immediately after exposure.
Photophobia (glare): Occurs with iris damage or uveitis.
Damage can range from the anterior segment to the posterior segment.
Anterior Segment Findings
Corneal abnormalities: Swelling, abrasion, ulcer, epithelial defect. Corneal ulcers due to overheating of metal shields have also been reported with CO2 lasers 1).
Uveitis: Anterior uveitis is frequently observed.
Pupillary irregularity and iris atrophy: Iris melanin absorbs laser light and can cause irreversible iris damage. Accompanied by transillumination defects.
Accidental complications have been reported even when using a metal corneal shield. In CO2 laser resurfacing, insufficient cooling time between laser pulses can cause the metal shield to overheat, leading to bilateral bullous keratopathy. There is also a report that cataract formation occurs when the corneal temperature reaches 80°C for 14 seconds.
SD-OCT shows hyperreflective foci in the fovea and disruption of the ellipsoid zone (photoreceptor inner segment/outer segment junction). These findings reflect photoreceptor damage in the outer retina and correlate with visual prognosis.
QAre you protected from the laser if you keep your eyes closed?
A
The thickness of the eyelids is not sufficient to prevent laser penetration. Closing the eyes alone does not protect them; protective goggles or corneal shields appropriate for the wavelength are necessary. In particular, Nd:YAG lasers (1,064 nm) and high-power laser pointers can penetrate eyelid tissue and reach the retina.
Most laser eye injuries occur due to non-compliance with safety measures. In a study of 40 individuals who sustained eye injuries, only 15% were wearing protective eyewear1).
Although laser energy is limited by JIS C 6802, some overseas products do not meet this standard. Even a few seconds of exposure can cause irreversible damage to the sensory retina by irradiating the macula. Some home-use beauty devices and laser pointers operate beyond their rated output, so caution is necessary.
In the exposure history, it is important to obtain information on the type of light source, wavelength, output, exposure duration, and distance between the eye and the light source. Also check the type, presence, and position of any protective equipment used. In laser pointer accidents, also record the product model number, output labeling, and place of purchase.
QWhat should you do if you notice vision changes after cosmetic laser?
A
If you experience decreased vision, blurring, scotoma, floaters, etc. after the procedure, you should see an ophthalmologist immediately. The time from exposure to symptom onset is short (immediate for thermal burns, a few days for photochemical reactions), and early detailed examination is essential for assessing damage and determining treatment strategy. Evaluation of the outer retina by SD-OCT is important for judging visual prognosis.
Treatment for laser-induced eye injury varies depending on the site and extent of damage. There are no established uniform medication guidelines. The treatment plan is determined based on a detailed history and physical examination. Observation is the mainstay, and prevention is the most important measure.
Treatment of Corneal Injury
Superficial lesions: Managed with topical antibiotics, topical steroids, therapeutic contact lenses, or eye patches.
Endothelial injury: Damage to the corneal endothelium can lead to bullous changes, corneal thickening, and vision loss. Corneal transplantation may be necessary.
Treatment of Retinal Injury
Steroid therapy: Topical, injection, implant, or systemic administration is selected according to the condition. Aimed at reducing inflammation and promoting RPE healing.
Macular hole: Macular holes caused by Nd:YAG laser often do not close spontaneously, and vitrectomy is considered.
Other treatments
Iritis: Anti-inflammatory treatment with steroid eye drops and mydriatics (e.g., atropine) is performed.
Ascorbic acid: Administered topically or orally to promote fibroblast activity and reduce ocular damage.
Laser-induced retinal damage is considered to have “no effective treatment,” and the efficacy of steroid therapy is not established. Prevention through the use of protective eyewear is most important.
QCan retinal damage caused by cosmetic lasers be cured?
A
Prognosis varies depending on the extent of damage and the type of laser. In mild cases, spontaneous recovery can be expected. Anti-VEGF drugs (bevacizumab) are effective for choroidal neovascularization, with reports of visual recovery1). On the other hand, in severe damage involving macular holes from Nd:YAG laser or deep retinal atrophy, visual prognosis may be poor.
The effects of laser on living tissue are determined by irradiation power and duration, and are classified into disruption, photoablation, coagulation, hyperthermia, and photochemical reaction.
Short-wavelength blue and green lasers are more likely to cause retinal damage than longer wavelengths. When blue light is absorbed by lipofuscin in retinal pigment epithelial cells or by visual pigments in photoreceptors, reactive oxygen species such as singlet oxygen are produced. Normally, enzymes and antioxidants eliminate these reactive oxygen species, but excessive light exposure leads to peroxidation of photoreceptor membranes, resulting in photoreceptor and retinal pigment epithelial cell damage. In this photochemical type, there are no abnormalities immediately after injury; subjective symptoms and macular degeneration appear several days later.
High-power lasers cause photothermal damage through photocoagulation. They raise retinal temperature by 40–60°C, denaturing proteins. In the thermal burn type, subjective symptoms and coagulation spots in the macula are observed immediately after injury.
The mechanism of eye damage depends on the laser wavelength.
Wavelength Range
Damage Mechanism
Typical Lasers
Short wavelength (400–532 nm)
Photochemical reaction and photothermal damage
Blue diode, green laser pointer
Medium wavelength (532–755 nm)
Photothermal damage
KTP, pulsed dye laser
Long wavelength (755–1,064 nm)
Photothermal + photomechanical damage
Alexandrite, diode, Nd:YAG
Far infrared (10,600 nm)
Vaporization via water absorption
CO2
Nd:YAG laser (1,064 nm) has an invisible wavelength, making accidents more likely, and its high power can cause physical retinal damage (retinal opacity, subretinal hemorrhage, macular hole). CO2 laser (10,600 nm) is absorbed by water and causes vaporization, potentially directly damaging the cornea and lens, which are water-containing tissues 1).
A review of 21 case reports found that even with appropriate use of wavelength-specific goggles and intraocular corneal shields, severe ocular injury occurred in 33% of cases 1). Metal shields may reflect laser light, and plastic shields risk melting or igniting with long-wavelength lasers. Ocular adverse events from ablative energy devices include keratopathy, corneal damage, retinal damage, and macular neovascularization1).
In response to the increase in eye injuries from high-power laser pointers, there is a movement toward stricter regulations in various countries. In Europe, output limits based on IEC 60825-1 are being tightened, and restrictions on the sale of Class 3B and 4 products to general consumers are under discussion. Accidental irradiation of aircraft has also become an international issue, with reports of temporary visual impairment in pilots.
Research is progressing on wavelength-adaptive (tunable) laser protection filters. The challenge is optical design that maintains visible light transmittance while covering a wide wavelength range, and practical application of multi-wavelength shields for medical facilities and aesthetic clinics is anticipated.
High-resolution OCT is being studied to track retinal structural recovery after laser injury. Regeneration of the ellipsoid zone and recovery of foveal morphology have been reported to correlate with visual prognosis, and are considered useful for objective evaluation of treatment efficacy.
Sullivan DA, Rouen PA, Aragona P, et al. An update on the ocular surface and eye cosmetics and cosmetic procedures. Ocul Surf. 2024. Available in PMC 2024 July 14.
Ajudua S, Mello MJ. Shedding some light on laser pointer eye injuries. Pediatr Emerg Care. 2007;23(9):669-72. PMID: 17876263.
Kim RY, Ra H. Observation of changes after peripheral retinal injury by cosmetic laser, using wide-field scanning laser ophthalmoscope: A case report. Medicine (Baltimore). 2019;98(6):e14354. PMID: 30732166.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.