Primary Stage
Incubation period: 10–90 days.
Chancre: Painless induration at the inoculation site. Disappears in about 4 weeks. May occur on the conjunctiva or around the eye.

Syphilitic uveitis is a condition in which Treponema pallidum enters the eye hematogenously and causes intraocular inflammation. Syphilis is a sexually transmitted infection caused by the spirochete Treponema pallidum, and symptomatic syphilis is classified into stages 1 through 4. Recently, stages 3 and 4 syphilis are rarely encountered; most cases are latent syphilis without skin or mucosal lesions. In acquired syphilis, uveitis occurs in approximately 5% of secondary syphilis cases. Due to advances in perinatal care, fresh cases of congenital syphilis with ocular involvement are almost never seen in Japan.
Globally, 5.7–6 million new syphilis infections are reported annually among individuals aged 15–49 1)5). Ocular syphilis accounts for approximately 0.6–2% of all syphilis cases 1)2) and about 10% of all infectious uveitis cases 3). A study in North Carolina found ocular syphilis in 63 of 4,232 cases (1.5%), of which 38% were diagnosed during primary or secondary syphilis 1).
In Japan, the number of syphilis infections has been increasing again, from fewer than 1,000 reported cases in 2011 to over 6,000 in 2017. Recently, the increase has been centered on patients including MSM (men who have sex with men) and those with HIV co-infection. Because of its diverse clinical presentations, syphilis is called “the great imitator” 1)5). Treatment follows neurosyphilis guidelines.
Ocular syphilis can occur at any stage, including primary, secondary, tertiary, and latent stages. It most commonly occurs during secondary acquired syphilis, with uveitis being the main manifestation. Since ocular symptoms may be the first clue to syphilis diagnosis, syphilis should always be considered in cases of uveitis of unknown cause.
Ocular manifestations of syphilis include anterior segment inflammation, uveitis, optic neuritis, and chorioretinitis, among others, and can mimic many other eye diseases. This makes diagnosis often delayed, and this diverse clinical picture is why it is called “the great imitator” 5).
It occurs via transplacental infection. Early congenital syphilis (birth to 3 months of age) presents with chorioretinitis. Late congenital syphilis is characterized by the classic Hutchinson triad (M-shaped notching of permanent teeth, sensorineural hearing loss, interstitial keratitis). In old congenital syphilis, the fundus shows a salt-and-pepper appearance (scattered chorioretinal atrophy) with proliferation of retinal pigment epithelial cells, sometimes resembling retinitis pigmentosa.
HIV co-infection is an important risk factor for ocular syphilis, and HIV testing is recommended for all patients at the time of syphilis diagnosis1). In HIV-positive individuals, uveitis is more severe and often bilateral, altering the clinical presentation. Additionally, in AIDS, serological tests may be false negative, which requires attention.
Primary Stage
Incubation period: 10–90 days.
Chancre: Painless induration at the inoculation site. Disappears in about 4 weeks. May occur on the conjunctiva or around the eye.
Secondary Stage
Onset: 4–10 weeks after the appearance of chancre.
Systemic dissemination: Hematogenous spread affects the nervous system, eyes, gastrointestinal tract, and liver. Ocular involvement occurs in about 10%. Maculopapular rash on palms and soles is seen in over 70%.
Ocular findings: Mainly uveitis, retinitis, and optic neuritis.
Latent Stage
Classification: Early (within 1 year) and late (after 1 year).
Course: About one-third of untreated cases progress to the tertiary stage. Ocular syphilis may become apparent even without symptoms.
Tertiary Stage
Cardiovascular: Aortitis, aortic aneurysm.
Neurosyphilis: Meningeal syphilis, meningovascular syphilis, tabes dorsalis, general paresis.
Ocular findings: Argyll Robertson pupil, optic atrophy, gumma.
Gumma: Benign localized granulomatous reaction. Occurs throughout the body including the choroid and iris.
Ocular findings vary greatly depending on the stage of syphilis.
| Classification | Onset time | Main ocular symptoms |
|---|---|---|
| Congenital syphilis (early) | Birth to 3 months of age | Chorioretinitis |
| Congenital syphilis (late) | School age and later | Interstitial keratitis, iritis, dacryocystitis |
| Acquired primary syphilis | 3 weeks to 3 months | Chancre of eyelid and conjunctiva |
| Acquired secondary stage | 4 to 10 weeks | Blepharitis, conjunctivitis, keratitis, iridocyclitis, iris nodules, scleritis, retinochoroiditis, vitritis, optic neuritis, retinal vasculitis, exudative retinal detachment |
| Acquired late stage | Several years to decades | Eyelid gumma, interstitial keratitis, scleritis, uveitis, optic papillitis, Argyll Robertson pupil, lens dislocation, secondary retinitis pigmentosa |
| Disease type | Frequency |
|---|---|
| Panuveitis | 75%3) |
| Chorioretinitis | 93%4) |
| Granulomatous iridocyclitis | 46%1) |
| Hypopyon | 6%2) |
Findings in ocular syphilis vary depending on the affected site. Panuveitis is the most common type (75%)3), and chorioretinitis is observed in 93% of posterior segment involvement4).
Anterior Segment Findings
Conjunctiva: Chancre in the first stage, mild conjunctivitis in the second stage, and gumma in the third stage.
Sclera: Episcleritis (more common in the second stage), scleritis (more common in the third stage). Nodular or diffuse.
Syphilitic interstitial keratitis: Immune-mediated non-ulcerative, non-suppurative interstitial keratitis. Neovascularization → ghost vessels. One of Hutchinson’s triad in congenital syphilis.
Granulomatous iridocyclitis: Most common ocular type of syphilitic uveitis (46%) 1). May leave anterior synechiae and iris atrophy. Characteristically resistant to topical steroids.
Hypopyon and keratic precipitates (KP): Bilateral hypopyon occurs in about 6% 2). May form mutton-fat KP.
Uvea and Posterior Segment
Intermediate, posterior, and panuveitis: Can present as anterior, posterior, or panuveitis. Granulomatous or non-granulomatous.
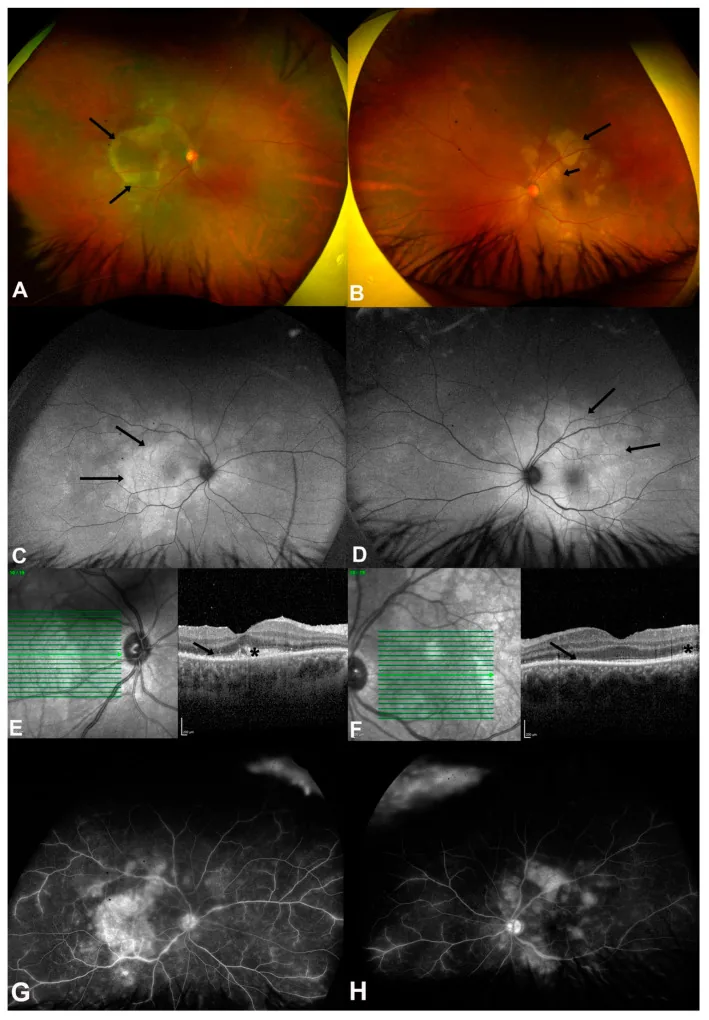
ASPPC (Acute Syphilitic Posterior Placoid Chorioretinitis): A characteristic special type in secondary syphilis. Disc-shaped, yellow lesions at the RPE level in the macula to peripapillary area. OCT shows disruption and hyperreflective elevation of the outer retina and RPE 3). FAF shows hyperfluorescent and hypofluorescent patches. Responds well to antibiotic treatment.
Retinal vasculitis and retinitis: Arteritis is considered characteristic, but phlebitis is also common and may lead to sheathing 9). Non-perfusion areas can lead to proliferative changes. “Ground-glass retinal infiltration” and “small creamy retinal surface deposits” are characteristic findings 1)5).
Severe vitreous opacities: Often resolve rapidly within a few days after administration of penicillin antibiotics.
Optic Nerve and Neuro-ophthalmology
Optic neuritis: Unilateral or bilateral. Anterior or retrobulbar optic neuritis, papilledema, neuroretinitis, optic atrophy. Optic nerve involvement is seen in 12–78% of ocular syphilis 3). Delayed treatment leads to optic atrophy and affects visual prognosis.
Argyll Robertson pupil: Miosis, loss of light reflex but preserved near response. More common in the third stage but can appear earlier 5).
Ocular motility abnormalities: In the third stage, caused by superior orbital fissure syndrome, brainstem infarction, or compression by aneurysm. Diplopia occurs when neurosyphilis is present.
ASPPC (Acute Syphilitic Posterior Placoid Chorioretinitis) is a posterior segment finding highly specific to syphilis, characterized by the formation of large, placoid yellow-white lesions in the posterior pole 5). Fluorescein angiography shows characteristic early hypofluorescence and late hyperfluorescence. OCT reveals disruption and hyperreflective elevation of the outer retina and RPE, and it responds well to antibiotic treatment.
In uveitis of unknown cause, always consider syphilis and maintain a high index of suspicion. When investigating the cause of uveitis, serological testing for syphilis should always be performed.
In clinical practice, non-treponemal tests and specific treponemal tests are used in combination.
| Type of Test | Representative Tests | Features and Uses |
|---|---|---|
| Non-treponemal tests (STS) | RPR (rapid plasma reagin), VDRL | High sensitivity, positive early. Biological false positives possible. Parallels infection activity → used for screening and treatment efficacy assessment |
| Treponemal tests (TP antigen method) | TPHA, FTA-ABS, TP-PA, EIA | Positive confirms syphilis. Remains positive long after treatment → unsuitable for treatment assessment |
Detection of syphilis antibodies in vitreous fluid by EIA shows high accuracy with sensitivity 90.9% and specificity 100%4). It is useful for diagnosis even in HIV-coinfected cases where serum tests may be false negative.
| Test | Sensitivity | Specificity |
|---|---|---|
| Serum EIA | High sensitivity (screening) | High specificity |
| Vitreous EIA | 90.9%4) | 100%4) |
In ocular syphilis, CSF examination is recommended to evaluate for neurosyphilis 4). If isolated ocular symptoms, confirmed ocular abnormalities, and positive treponemal tests are present, CSF examination before treatment is not considered mandatory 3). Lumbar puncture is performed when optic neuritis, ocular muscle palsy, or cranial nerve symptoms are suspected.
It is useful in HIV-coinfected patients, where serum syphilis tests are prone to false negatives, and in cases where syphilitic uveitis is strongly suspected despite negative serology 4). Vitreous EIA has 100% specificity, and a positive result provides diagnostic evidence for syphilitic uveitis.
Differential diagnoses include sarcoidosis, tuberculous uveitis, acute retinal necrosis (ARN)/PORN, APMPPE, serpiginous choroiditis, cytomegalovirus retinitis, toxoplasma retinitis, Behçet’s disease, and intraocular lymphoma 4)7). Since direct detection of T. pallidum in the eye is not possible, integrated assessment of serological tests and clinical findings is crucial 10). Special attention is needed in HIV-positive patients, as serological tests may be false negative in AIDS.
Oral antisyphilitic therapy (for mild cases or outpatient management):
Neurosyphilis and ocular syphilis (inpatient intravenous therapy):
Syphilitic uveitis is often associated with neurosyphilis, and high-dose penicillin intravenous therapy is standard. First-line treatment is intravenous aqueous penicillin G.
| Regimen | Dose and route |
|---|---|
| Aqueous crystalline penicillin G (first-line) | 18–24 million units/day (3–4 million units IV every 4 hours or continuous infusion) for 10–14 days1)2)3)5) |
| Procaine penicillin G (alternative) | 2.4 million units IM once daily plus probenecid 500 mg orally 4 times daily for 10–14 days1)2) |
| Ceftriaxone (alternative) | 1–2 g IM or IV once daily for 14 days1)4)6) |
The treatment success rate is reported to be approximately 90%3).
Nwaobi et al. (2023) reported a 46-year-old man with ocular syphilis (RPR 1:64, TPHA 1:512) who received neurosyphilis treatment with IV PCG 4 million units q4h, and vision recovered after 6 months2).
The course of RPR (lipoidal antigen test) is used as a reference. A decrease in antibody titer to ≤8-fold or ≤1/4 of the initial value is considered evidence of antisyphilitic effect 10). Recurrence is possible after treatment, so regular RPR monitoring should be continued.
Penicillin desensitization is recommended as the first choice 1)7).
Cubelo et al. (2022) reported that a 24-year-old HIV-positive man with PCG allergy received doxycycline 100 mg BID for 14 days, and RPR decreased from 1:1,024 to 1:32 7). PCG desensitization was subsequently performed.
It develops as a reaction to inflammatory lipoproteins derived from Treponema pallidum that are killed within 24 hours of starting treatment. Ophthalmologically, it may be seen as a recurrence of iritis (flare-up of inflammation).
Penicillin desensitization is recommended first. If this is difficult, alternatives include ceftriaxone (1–2 g once daily for 14 days) or doxycycline (200 mg/day for 28 days) 1)7). However, evidence for these alternatives in ocular syphilis is limited compared to penicillin.
Treatment should be continued without interruption. Systemic symptoms such as fever and headache are managed symptomatically with antipyretics and analgesics. Ocular symptoms (including vision loss, optic disc swelling, etc.) are usually temporary and improve with continued treatment 1).
Steroids are considered as adjunctive therapy only when inflammation persists after adequate antibiotic administration. Administering steroids without immunosuppression prior to treatment is contraindicated because it can lead to exacerbation of syphilis 5).
T. pallidum disseminates hematogenously from the primary infection site and reaches systemic organs including ocular tissues. It crosses the blood-retinal barrier and causes inflammation in the choroid, retina, and vitreous. Ocular syphilis can occur at any stage from primary to late syphilis, but posterior segment involvement is more common after the secondary stage.
Treponema pallidum induces production of IL-1β, IL-6, IL-12, and TNF-α via TLR2/TLR4/TLR5-dependent signaling, causing tissue damage similar to delayed-type hypersensitivity reactions 1). CD4+ cells and macrophages dominate primary lesions, while CD8+ cells dominate secondary lesions. IFN-γ production activates and recruits macrophages.
In syphilitic interstitial keratitis, the main pathology is not direct infection by T. pallidum itself, but an immune response to treponemal antigens (lymphocyte infiltration and vascular invasion into the corneal stroma). Therefore, it responds to steroids but may not resolve with penicillin alone.
Treponema pallidum has slow proliferation and the ability to invade immune-privileged tissues such as the eye, CNS, and placenta 1). Apoptosis of CD4+ cells via the Fas-associated death pathway leads to incomplete immune clearance and establishment of chronic infection.
In HIV-positive patients, progression of ocular syphilis after the secondary stage is accelerated. Bilateral involvement is more frequent in HIV-positive patients (62%) compared to HIV-negative patients (38%) (study of 96 cases) 1). In AIDS, serological tests may be false-negative, requiring caution in diagnosis.
In HIV-positive patients with ocular syphilis, IRIS (immune reconstitution inflammatory syndrome) may occur after initiation of antiretroviral therapy (ART), causing transient worsening of inflammation 11).
In a review by Pipito et al. (2023), IRIS cases had low CD4 cell counts before ART (median 196/μL), which recovered to 318/μL after ART 11). In cases with low CD4, there is also a risk of false-negative syphilis serology 11).
Response to penicillin antibiotics is generally good, and vitreous opacity often resolves rapidly within a few days of administration. The treatment success rate is reported to be approximately 90% 3). In cases complicated by optic neuritis, delayed treatment can lead to optic atrophy, affecting visual prognosis. In HIV-coinfected cases, the risk of relapse after treatment is high, and long-term monitoring of RPR trends is necessary.
If inflammation worsens around 28 days after ART initiation, suspect IRIS. Differentiate between unmasking and paradoxical types, and if syphilis treatment is insufficient, prioritize penicillin G therapy 11). Addition of steroids should be considered after establishing anti-syphilitic treatment.
Anti-VEGF therapy for inflammatory choroidal neovascularization (iCNV): iCNV associated with ocular syphilis is an extremely rare condition. In a report by Świerczyńska et al. (2021), intravitreal injection of aflibercept stabilized disease activity in about one-third of cases with a single injection, and stabilized vision in about two-thirds with two injections 6). iCNV does not resolve with antibiotic therapy alone, and additional intravitreal anti-VEGF injection was effective.
Venous-predominant syphilitic retinal vasculitis: Although syphilitic retinal vasculitis is usually arteritic or mixed, cases with predominant phlebitis have been reported in HIV-coinfected patients. Mammo et al. (2022) reported a case of a 53-year-old HIV-positive male with panuveitis predominantly involving phlebitis, treated with IV PCG 4 million units for 14 days × 2 courses 9). After treatment, it progressed to paravenous pigmentary retinopathy.
Improved diagnostic accuracy with multimodal imaging: The combination of EDI-OCT, ultra-widefield autofluorescence (FAF), and ICG is expected to improve the diagnostic accuracy of ocular syphilis1)3). ICG detects choroidal dark dots, hot spots, and blurred choroidal vessels. Accumulation of these multimodal imaging findings may contribute to differentiation from sarcoidosis and tuberculosis.
Advances in diagnostic techniques using intraocular fluids: Detection of syphilis antibodies by EIA in vitreous fluid (sensitivity 90.9%, specificity 100%) has high diagnostic value in serologically false-negative cases and refractory posterior uveitis4). Especially in HIV-coinfected or immunocompromised patients, where serological diagnosis is less reliable, intraocular fluid testing is becoming an important adjunctive diagnostic method.
Optimization of IRIS management: Research is progressing on the mechanism of IRIS associated with ART initiation and optimal management strategies11). Optimizing the timing of antisyphilitic treatment and ART for prevention and treatment of IRIS remains a future challenge.