Human herpesvirus 5, commonly known as cytomegalovirus (CMV), is the largest virus of the Herpesviridae family with a double-stranded DNA genome. It has affinity for a wide range of tissues in the human body. Primary infection, reinfection, or reactivation in the retina leads to CMV retinitis, characterized by full-thickness retinal necrosis and edema.
The CMV antibody seroprevalence is high at 70–90%, with most individuals acquiring asymptomatic infection in early childhood. CMV retinitis in adults is predominantly an opportunistic infection associated with viral reactivation1).
If a mother experiences primary infection or reactivation during early pregnancy, 20–40% of cases result in transplacental infection of the fetus, leading to congenital CMV infection as part of TORCH syndrome, which can include CMV retinitis.
Epidemiology:
The incidence increased sharply during the AIDS epidemic of the 1980s–1990s. With the widespread use of ART (antiretroviral therapy), the incidence has significantly decreased, but it remains an important ocular complication in AIDS patients and post-transplant patients4, 5, 6).
In the 2002 national survey of the Uveitis Clinical Practice Guidelines, CMV retinitis accounted for 0.8% (24 cases), and in the 2009 survey, 1.0% (37 cases)1).
In recent years, with the widespread use of biologics, CAR-T cell therapy, and intensive chemotherapy, reports of CMV retinitis in non-AIDS immunocompromised patients have been increasing 7, 9).
QCan CMV retinitis occur even in immunocompetent individuals?
A
In principle, it is rare in healthy immunocompetent individuals. However, in recent years, reports of CMV anterior segment syndrome presenting as anterior uveitis or corneal endotheliitis in immunocompetent individuals have been increasing (see separate section “CMV anterior uveitis”). CMV retinitis (posterior lesion) is primarily an opportunistic infection in immunocompromised hosts 1) and is extremely rare in healthy individuals. Long-term steroid use, diabetes-related immune dysfunction, and immunosenescence are considered background factors 11, 12).
QCan a patient with undiagnosed HIV infection present with CMV retinitis?
A
Yes. A retrospective study reported that 15% of HIV-positive CMV retinitis patients visited an ophthalmologist before HIV diagnosis, and in 9%, CMV retinitis was the only AIDS-defining illness 13). When CMV retinitis is suspected, HIV testing should be actively performed.
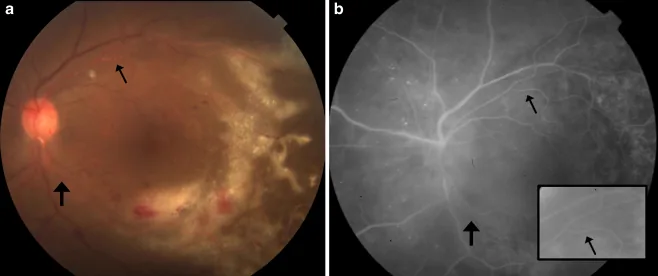
Patel A, et al. Kyrieleis plaques in cytomegalovirus retinitis. J Ophthalmic Inflamm Infect. 2011. Figure 1. PMCID: PMC3223340. License: CC BY.
Left: Fundus photograph showing yellow-white granular retinitis lesions extending near the macula, with retinal hemorrhages and white deposits along retinal arteries. Right: Fluorescein angiography shows vascular findings in the same area, illustrating the clinical picture of CMV retinitis.
Symptoms vary depending on the location and size of the lesion.
When the macula is involved: Rapid vision loss occurs
Early peripheral lesions: Often asymptomatic
After progression: Visual field defects and floaters appear
Characteristically, anterior chamber inflammation and vitritis are almost absent in the early stage, and these findings appear as the lesion expands, which is an important distinguishing point from ARN.
CMV retinitis is classified into three types based on characteristic fundus findings. In clinical practice, these types often coexist, and the location and size of the lesions are more important for prognosis prediction.
Peripheral granular type
Features: White granular exudates accumulate in a fan-shaped pattern with little to no hemorrhage.
Impact on vision: Vision is relatively preserved if the macula is spared.
Course: The most common type. It progresses gradually from the periphery toward the center.
Posterior pole vasculitis type
Features: Yellow-white exudates with retinal hemorrhage and edema appear along the vessels of the posterior pole. Extensive necrosis and hemorrhage described as “pizza pie” are characteristic.
Impact on vision: Vision loss is significant because the macula and optic nerve are affected.
Course: This type has the worst visual prognosis. Prompt treatment initiation is important.
Frosted branch angiitis type
Features: Retinal vessels, especially large ones, show white sheathing resembling frosted branch angiitis (FBA).
Frequency: A relatively rare type. It may appear as a sign of CMV-IRIS10).
Note: In clinical practice, the three types often coexist, and the location and size of the lesions are important for prognosis prediction.
Zone classification of lesions is important for determining the urgency of treatment.
Zone
Range
Clinical significance
Zone 1
Within 1 disc diameter of the optic disc, within 2 disc diameters of the macula
Start treatment immediately
Zone 2
From the equator to the ampulla of the vortex veins
Consider treatment
Zone 3
Most peripheral area
Observation may be acceptable
Retinal detachment (RD) is a serious complication. The larger the lesion area, the higher the risk of rhegmatogenous retinal detachment. Although the incidence has decreased since the introduction of ART, long-term vigilance is still required after treatment 3).
Tang et al. (2021) reported an HIV patient who developed frosted branch angiitis 35 days after starting HAART 10). Aqueous humor IL-6 was markedly elevated at 2,845 pg/mL and IL-8 at 967.8 pg/mL, indicating FBA as an unmasking type of IRIS. Inflammation improved with antiviral therapy alone.
In areas of healed CMV retinitis, the full thickness of the retina becomes necrotic and thins in a lace-like pattern. When vitreous traction is added, multiple tears easily occur, leading to retinal detachment. Therefore, long-term follow-up is necessary even after retinitis has subsided.
QWhy is retinal detachment common in CMV retinitis?
A
The necrotic full-thickness retina becomes thin and lace-like. Vitreous traction on this area easily causes multiple tears. The edge of the necrosis is particularly thin and at high risk for tear formation. Even after retinitis is controlled with treatment, the thinned retina remains, requiring long-term follow-up.
CMV retinitis is predominantly an opportunistic infection in immunocompromised individuals. The starting point for diagnosis is to identify underlying diseases that cause immunodeficiency, such as acquired immunodeficiency syndrome (AIDS), or a history of drug administration in adult patients 1).
Main risk factors:
AIDS: Patients with CD4-positive T lymphocyte count below 50/mm³. It was once the most common cause of CMV retinitis1)
After organ transplantation: Immunosuppressive therapy following hematopoietic stem cell transplantation, kidney transplantation, or liver transplantation
Malignancies: Chemotherapy for leukemia or lymphoma, high-dose steroid therapy
After CAR-T cell therapy: Case reports have been observed in the context of severe immunosuppression 8)
Intravitreal steroid injection: Nine cases have been reported after dexamethasone sustained-release implant (Ozurdex®), with an average onset of 2.6 months after injection 12)
Diabetes: Involves disruption of the blood-retinal barrier and increased CMV viral load 12)
Severe COVID-19: Interaction with CMV latency and reactivation has been reported 14)
Congenital infection: 20-40% transplacental infection when the mother has primary infection or reactivation in early pregnancy
Although there are no clear diagnostic criteria for CMV retinitis, clinical diagnosis is possible based on the characteristic retinal lesions combined with patient background (immunocompromised state) and fundus findings.
Confirmation of three types (peripheral granular, posterior pole vasculitic, and dendritic vasculitic). Early stages show minimal anterior chamber inflammation and vitritis.
Intraocular Fluid Quantitative PCR (Real-time)
High sensitivity and specificity; used for definitive diagnosis. May not be detected in early stages without anterior chamber inflammatory cells1)
Multiplex PCR (Advanced Medical Care)
Comprehensive detection of multiple viruses from a small sample. Useful for differentiation from ARN1)
CMV Antigenemia Assay / Blood PCR
Used as supplementary diagnostic reference. Ocular local PCR is preferred for definitive diagnosis.
Patient Background Confirmation
CD4 count, history of immunosuppressant use, ART treatment status, etc.
probable: characteristic fundus findings only (with immunocompromised background)
Next-generation sequencing (NGS) has been reported as an adjunctive diagnostic tool for cases difficult to diagnose by PCR, and has been used in post-CAR-T cases8). In HIV-negative immunosuppressed patients, diagnosis is often delayed; do not rule out based solely on serology, but combine ocular findings and intraocular fluid testing7, 9).
For differentiation from cotton-wool spots, lesion size is helpful. Lesions smaller than 750 μm suggest cotton-wool spots, while those larger suggest CMV retinitis.
Differential diagnoses:
Acute retinal necrosis (ARN): occurs in healthy individuals, with severe anterior inflammation, vitritis, and occlusive vasculitis
Intraocular lymphoma: glassy vitreous opacities, detection of lymphoma cells
HIV retinopathy: cotton-wool spots (<750 μm), no inflammation
QWhat is the most important test for diagnosing CMV retinitis?
A
Clinical diagnosis is based on characteristic fundus findings (any of the three disease types) and patient background (immunocompromised state). For definitive diagnosis, quantitative real-time PCR of intraocular fluid (aqueous humor or vitreous fluid) has the best sensitivity and specificity 1). Multiplex PCR (advanced medical care) has the advantage of being able to differentiate multiple viruses from a small sample, and is particularly useful for differentiating from ARN.
Intravenous ganciclovir is the first-line anti-CMV therapy. Depending on the location and size of the lesion and the presence or absence of side effects, oral valganciclovir, intravenous foscarnet, or intravitreal injection may be used alone or in combination. CMV retinitis is likely to involve potential multi-organ CMV infection, and the basis of antiviral therapy is systemic treatment.
4 tablets (1,800 mg) divided into 2 doses after meals
2 tablets (900 mg) once daily after meals
Foscarnet intravenous infusion
Foscavir injection (24 mg/mL)
90 mg/kg/dose twice daily
90 mg/kg/dose once daily
Induction therapy is generally administered for 2 to 3 weeks. Thereafter, maintenance therapy is continued. Foscarnet is an alternative when ganciclovir causes severe bone marrow suppression, but attention to nephrotoxicity is required.
When there are issues with side effects or when the lesion is located in the posterior pole, intravitreal injection of GCV or foscarnet may be performed (off-label).
Ganciclovir intravitreal injection: Induction dose 400 μg twice weekly (or 800 μg once weekly), maintenance dose 400 μg once weekly. Overseas, 2,000 μg once weekly may be used.
Foscarnet and cidofovir are second-line drugs when GCV/VGCV is intolerant or resistant. Cidofovir is administered once weekly (induction) then every 2 weeks (maintenance). Side effects include ocular hypotension (up to 50%), anterior uveitis, and nephrotoxicity; probenecid premedication is required.
After starting HAART, as CD4 counts recover, an excessive immune response to residual CMV antigens may occur (develops in 10–17% of CMV cases, mostly within 3 months of starting HAART). Management is as follows:
Continue antiviral therapy
For significant inflammation, add moderate-dose systemic steroids
After induction therapy, maintenance therapy is continued. In HIV/AIDS patients, continue antiviral therapy for at least 6 months; if CD4-positive T-cell count >100 cells/μL is maintained for 4–6 months, consider discontinuation. Follow-up: dilated fundus examination once a week during induction, every 2 weeks during maintenance, and once a month after stabilization.
Surgical Treatment for Complicated Retinal Detachment
If rhegmatogenous retinal detachment occurs, surgical treatment is indicated. Depending on the size of the lesion and extent of detachment, combine the following:
Vitrectomy
Endophotocoagulation
Scleral buckling
Long-acting gas or silicone oil tamponade
If treated at the appropriate time, the prognosis is not as poor as that of acute retinal necrosis.
The fundamental treatment is to reverse immunosuppression. In HIV-infected patients, initiating and continuing ART to restore CD4 counts is the cornerstone for preventing recurrence of CMV retinitis. Caution is needed for the development of immune recovery uveitis (IRU) after starting ART (see “Pathophysiology and detailed mechanism” section).
QAre acyclovir and valacyclovir ineffective for CMV retinitis?
A
They are ineffective. CMV has low sensitivity to acyclovir and valacyclovir; drugs for HSV/VZV are insufficient. Ganciclovir or valganciclovir are first-line for CMV. When ganciclovir cannot be used due to bone marrow suppression, foscarnet is an alternative.
CMV is the largest double-stranded DNA virus in the Herpesviridae family. After primary infection, it establishes latency in myeloid progenitor cells, monocytes, and macrophages. When immune function declines, the virus reactivates and spreads hematogenously to the eye, causing CMV retinitis.
CMV infects all layers of the retina, causing retinal necrosis primarily through direct viral cytopathic effects. Unlike ARN, immune-mediated inflammation is weak, and inflammatory signs are inconspicuous due to the weak immune response. This explains why anterior chamber inflammation and vitritis are rarely seen in the early stage.
CMV produces viral interleukin-10 (cmvIL-10) to suppress immunity, the pp65 protein inhibits the cGAS-STING signaling pathway, and MHC-I-like molecules evade NK cell attack 14). These immune evasion mechanisms form the basis for chronic persistent infection. CMV has also been shown to upregulate ACE2 receptor expression, potentially facilitating co-infection with SARS-CoV-2 14).
Coinfection with CMV and VZV/EBV has a worse prognosis than single infection.
Kondo et al. (2025) reported a case of bilateral CMV retinitis coinfected with EBV and VZV 15). Quantitative PCR showed high levels of CMV 6.7×10⁷ copies/mL and VZV 1.3×10⁸ copies/mL, leading to retinal detachment in both eyes.
When CD4-positive T lymphocyte counts rise rapidly after starting ART, existing opportunistic infections may worsen or new lesions may appear. This is called immune reconstitution inflammatory syndrome (IRIS). In ophthalmology, IRU is known to occur in eyes with a history of quiescent CMV retinitis after ART initiation, presenting as vitritis 1).
Pathogenesis of IRU: The prevailing theory is that when ART restores CMV-specific T-cell responses, residual CMV antigens that are slightly replicated in cells at the edge of already quiescent CMV retinitis lesions become unmasked by the immune response, leading to uveitis. The “unmasking type” of IRIS is a condition in which previously controlled infection becomes apparent shortly after starting HAART 10).
Symptoms and diagnosis of IRU: In addition to initial lesions such as iridocyclitis and vitritis, secondary macular edema and cataracts may occur. A history of ART initiation and an increase in CD4-positive T lymphocyte count are essential for diagnosis.
Treatment of IRU: Varies depending on severity and timing. Cases range from spontaneous remission with observation to those requiring discontinuation of ART, systemic steroids, or surgical treatment. However, the basic approach is to restart anti-CMV therapy against the residual pathogen 1).
While CMV retinitis in AIDS patients has greatly decreased due to the spread of ART, reports are increasing in non-AIDS immunosuppressed patients such as those after organ transplantation, CAR-T cell therapy, or use of biologic agents 7, 9). The causes of immunodeficiency are diversifying, and standardization of indications, duration, and drug selection for CMV prophylaxis is a challenge. Attention to delayed diagnosis is needed in HIV-negative patients 7, 9).
In drug-resistant and recurrent CMV retinitis, understanding the host immune response is important in addition to antiviral drugs. Li et al. (2022) reported that in immunocompetent patients with CMV retinitis, recruitment of CMV-specific T cells may be insufficient 16), and elucidation of local immune evasion mechanisms may lead to future treatment development. Currently, T-cell-related therapies are at the research stage and are not standard treatment.
Letermovir and maribavir are novel antiviral drugs that have shown efficacy against GCV/foscarnet-resistant CMV. In particular, maribavir has received FDA approval for refractory/resistant CMV infection after HSCT. Evidence for CMV retinitis is still limited, but application to multidrug-resistant cases is expected.
Zu et al. (2022) reported the world’s first case of CMV retinitis after CAR-T cell therapy 8). Severe humoral immunodeficiency caused by CAR-T therapy was thought to promote CMV reactivation, and NGS was used for diagnosis. This suggests the need for postoperative CMV screening and ophthalmic monitoring in patients receiving CAR-T therapy.
CMV may promote co-infection with SARS-CoV-2 by increasing ACE2 expression 14). Cases of CMV reactivation after severe COVID-19 have also been reported 14). Ophthalmic evaluation should be considered during severe COVID-19 in immunosuppressed patients.
Identification of host genetic polymorphisms affecting CMV susceptibility is progressing 14). In the future, genetic screening of high-risk patients may be used for preventive strategies.
Long-term follow-up by the Studies of Ocular Complications of AIDS (SOCA) shows that while visual prognosis for CMV retinitis patients has improved in the ART era, macular edema, cataract, and proliferative vitreoretinopathy due to IRU remain major causes of vision loss 3).
In recent years, CMV-induced iridocyclitis and corneal endotheliitis (CMV anterior uveitis) have been reported in immunocompetent individuals, expanding the intraocular spectrum of CMV infection. The TITAN Report 2 provides an international consensus on the management of CMV anterior uveitis, and further evidence accumulation is expected 2).
Research on early intervention to improve long-term outcomes of ophthalmic complications (CMV retinitis, optic atrophy) in congenital CMV infection is progressing. Early initiation of antiviral therapy may improve visual prognosis.
Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, et al. The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 2-global current practice patterns for the management of Cytomegalovirus anterior uveitis. Eye (Lond). 2024;38(1):68-75. doi:10.1038/s41433-023-02631-8. PMID:37419958; PMCID:PMC10764804.
Jabs DA, Ahuja A, Van Natta ML, et al. Long-term outcomes of cytomegalovirus retinitis in the era of modern antiretroviral therapy: Results from a United States Cohort. Ophthalmology. 2015;122(7):1452-1463. doi:10.1016/j.ophtha.2015.02.033.
Holland GN.. AIDS and ophthalmology: the first quarter century. Am J Ophthalmol. 2008;145(3):397-408. doi:10.1016/j.ajo.2007.12.001. PMID:18282490.
Douglas A. Jabs. Cytomegalovirus Retinitis and the Acquired Immunodeficiency Syndrome—Bench to Bedside: LXVII Edward Jackson Memorial Lecture. American Journal of Ophthalmology. 2011;151(2):198-216.e1. doi:10.1016/j.ajo.2010.10.018.
Heiden D, Ford N, Wilson D, Rodriguez WR, Margolis T, Janssens B, Bedelu M, Tun N, Goemaere E, Saranchuk P, Sabapathy K, Smithuis F, Luyirika E, Drew WL.. Cytomegalovirus retinitis: the neglected disease of the AIDS pandemic. PLoS Med. 2007;4(12):e334. doi:10.1371/journal.pmed.0040334. PMID:18052600; PMCID:PMC2100142.
Yeh S, Albini TA, Moshfeghi AA, et al. Cytomegalovirus retinitis in an era of CMV prophylaxis and non-AIDS immunosuppression. Ophthalmic Surg Lasers Imaging Retina. 2014;45(4):309-313.
Zu C, Xu Y, Wang Y, et al. Cytomegalovirus retinitis and retinal detachment following chimeric antigen receptor T cell therapy for relapsed/refractory multiple myeloma. Curr Oncol. 2022;29(2):901-907. doi:10.3390/curroncol29020044. PMID: 35200544; PMCID: PMC8870699.
Downes KM, Tarasewicz D, Weisberg LJ, Cunningham ET Jr. Good syndrome and other causes of cytomegalovirus retinitis in HIV-negative patients-case report and comprehensive review of the literature. J Ophthalmic Inflamm Infect. 2016;6(1):3. doi:10.1186/s12348-016-0070-7. PMID:26809342. PMCID:PMC4726639.
Tang S, Zhao N, Wang LY, et al. Frosted branch angiitis due to cytomegalovirus-associated unmasking immune reconstitution inflammatory syndrome: a case report and literature review. BMC Infect Dis. 2021;21:613. doi:10.1186/s12879-021-06311-4. PMCID: PMC8236202.
Ruchi Shukla, Ashutosh K Mishra, Archana Verma, Pragati Garg, Shrinkhal LNU. A Rare Case of Cytomegalovirus Retinitis in a Young Immunocompetent Patient. Cureus. 2023. doi:10.7759/cureus.44948.
Marissa K. Shoji, Jesse D. Sengillo, Akaanksh Shetty, Joshua Uhr, Jayanth Sridhar. Cytomegalovirus Retinitis Associated With Intravitreal Dexamethasone Implant Injection. Journal of VitreoRetinal Diseases. 2023;8(2):215-219. doi:10.1177/24741264231221325.
Ferreira Tátá C, Ramires T, Piteira M, Matono R, Guz C.. Cytomegalovirus Retinitis as a Sole Manifestation of HIV Infection. Cureus. 2021;13(10):e18642. doi:10.7759/cureus.18642. PMID:34786237; PMCID:PMC8580125.
Stoicescu ER, et al. CMV retinitis in the context of SARS-CoV-2 infection: a case study and comprehensive review of viral interactions. Pathogens. 2024;13(11):938. doi:10.3390/pathogens13110938. PMID: 39599491.
Kondo H, Egawa M, Yanai R, Mitamura Y. Bilateral cytomegalovirus retinitis with co-infection of Epstein-Barr virus and varicella-zoster virus: a rare case. Cureus. 2025;17(12):e99893. doi:10.7759/cureus.99893. PMID: 41583226; PMCID: PMC12824466.
Li N, Sun G, Zhu L, Ding K, Liu H, Zhu X, et al. Cytomegalovirus-Specific T Cells from Third-Party Donors Successfully Treated Refractory Cytomegalovirus Retinitis after Unrelated Umbilical Cord Blood Transplantation. J Immunol Res. 2022;2022:6285510. doi:10.1155/2022/6285510. PMID:36426138. PMCID:PMC9681565.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.