Cytomegalovirus (CMV, human herpesvirus type 5) is a DNA virus belonging to the Herpesviridae family. In adults over 40 years of age, the seropositivity rate reaches 80–85%.
In immunocompromised individuals, it is well known to cause necrotizing retinitis (CMV retinitis). In recent years, CMV-induced iridocyclitis and corneal endotheliitis have also been observed in immunocompetent individuals, often accompanied by elevated intraocular pressure and recurrent or persistent inflammation. The Uveitis Clinical Practice Guidelines list CMV as an independent cause of herpetic anterior uveitis alongside HSV and VZV 3).
CMV anterior uveitis is more frequently reported in Asia, with case series from Japan, China, and Singapore leading the way. High CMV seroprevalence and possible genetic susceptibility have been suggested.
Most reported cases occur in males, with a bimodal age distribution. Recurrent acute type is more common in the 30s–50s, while chronic hypertensive type tends to occur in the 50s–70s.
Posner-Schlossman syndrome (PSS) is a unilateral, recurrent iritis with acute intraocular pressure elevation, long considered idiopathic. Reports of CMV detection in the aqueous humor of PSS patients have led to the view that it may be the same disease as or overlap with CMV anterior uveitis 3). Both conditions share features such as mild anterior chamber inflammation with elevated IOP. Classic PSS without CMV involvement often has a good prognosis without corneal endothelial damage, but in CMV-confirmed cases, endothelial cell loss can become problematic.
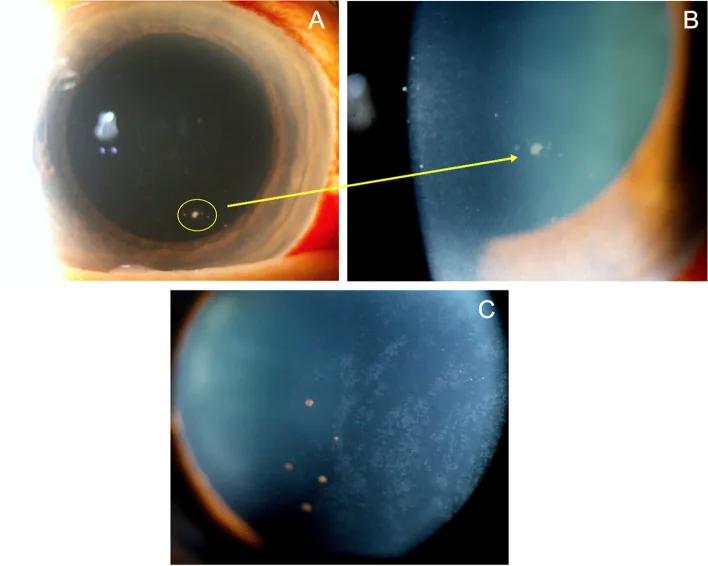
Caplash S, et al. Mimickers of anterior uveitis, scleritis and misdiagnoses- tips and tricks for the cornea specialist. J Ophthalmic Inflamm Infect. 2024. Figure 3. PMCID: PMC11004105. License: CC BY.
Slit-lamp photograph showing multiple white coin-shaped keratic precipitates on the corneal endothelium. This represents typical inflammatory findings seen in CMV corneal endotheliitis and anterior uveitis.
CMV anterior uveitis often has a more insidious onset and chronic course compared to HSV and VZV. It is frequently misdiagnosed because it lacks the typical corneal hypoesthesia, vesicles, and skin rash seen in herpes infections1).
Intraocular pressure: Marked elevation of 40–60 mmHg (sometimes over 60 mmHg)
Anterior chamber inflammation: Relatively mild (cells 2+ or less)
KP: Small to medium-sized gray-white granulomatous KP without pigment
Course: Episodic with repeated remissions and relapses
Intraocular pressure characteristics: During remission, the intraocular pressure is lower than that of the fellow eye. The angle is open, with no peripheral anterior synechiae.
FUS type (Fuchs uveitis syndrome-like)
Age of onset: 40s to 60s
Intraocular pressure: Chronic mild to moderate elevation
Elevated intraocular pressure: Observed in 95.31% of PCR-positive CMV anterior uveitis cases 1)
Iris atrophy: Patchy iris atrophy (present in 34.14%). Depigmentation on the corneal endothelial side is also characteristic 1)
Coin-shaped KP (KP corrals): A characteristic pattern where KP are arranged in a circular or ring-like shape. Strongly suggestive of CMV ocular infection.
Linear KP: Horizontal linear or map-like deposits characteristic of corneal endotheliitis. Often appear in combination with KP corrals.
Corneal endotheliitis: Nodular endothelial lesions, progressive decrease in endothelial cell count. Accompanied by localized corneal stromal edema.
Posterior synechiae are rare: The frequency of posterior synechiae is lower compared to HSV and VZV.
Corneal edema: Characteristically very mild relative to the degree of intraocular pressure elevation
QHow do you differentiate CMV anterior uveitis from varicella-zoster virus uveitis?
A
VZV uveitis, decreased corneal sensation, a zoster-like rash, and sectoral iris atrophy are clues for differentiation, but these are absent in CMV anterior uveitis. Coin-shaped KP (KP corrals) and linear KP are characteristic findings of CMV corneal endotheliitis. Lack of response to acyclovir or valacyclovir treatment is also a strong reason to suspect CMV. For definitive diagnosis, quantitative PCR testing of aqueous humor is essential; qualitative PCR can yield false positives, so quantitative methods must be used1).
CMV latently infects myeloid progenitor cells (monocytes/macrophage precursors). By mechanisms not fully understood, the virus reactivates in macrophages and dendritic cells of the anterior segment, releasing interferon-γ and interferon-β, leading to anterior segment inflammation. Infection at other sites may also induce CMV reactivation in circulating monocytes.
Medications that may trigger reactivation (reported):
Dexamethasone eye drops (reactivation due to local immunosuppression)
Anterior chamber paracentesis (aqueous humor collection) is a relatively short procedure performed under local anesthesia in an outpatient setting. It is an important test to identify the causative virus of infectious uveitis, and when performed properly, the risk of complications is low. It is an essential step for the definitive diagnosis of CMV anterior uveitis, and 73.3% of world experts always perform it in suspected cases 1). Starting treatment without a definitive diagnosis carries the risk of continuing acyclovir-type drugs that are not effective against CMV.
78% of specialists choose oral valganciclovir as systemic therapy 1)
Note: Complete blood count and serum creatinine must be monitored every 2 weeks
Management of recurrence: Recurrence occurs in up to 80% after dose reduction or discontinuation. In case of recurrence, restart at the initial dose and taper more slowly (supported by 88% of specialists) 1).
Steroids should be used only under antiviral coverage (supported by 71%) 1). Steroid use without antiviral therapy carries a risk of worsening corneal endothelial cell damage.
First choice: Prednisolone acetate ophthalmic suspension 1% (chosen by 71%) 1)
Initial dosing: 4 times daily for 1–2 weeks, then taper according to clinical response
Duration of maintenance: 84% of specialists support tapering over up to 12 months 1)
Routes to avoid: Periocular and systemic steroids (88% support avoidance) 1)
Since intraocular pressure during an attack can rise to 40 mmHg or higher (sometimes 60 mmHg or higher), prompt management of intraocular pressure is necessary.
First-line: Beta-blocker eye drops (supported by 79% of specialists) 1)
Second-line: Alpha agonists or carbonic anhydrase inhibitors (eye drops or oral)
Prostaglandin-related drugs are generally avoided (concern for worsening herpes infection) 1)
If intraocular pressure elevation is severe, oral carbonic anhydrase inhibitors may also be added.
If intraocular pressure control is insufficient with medication, glaucoma surgery (such as trabeculectomy) may be required. If left untreated, more than 25% will require glaucoma surgery within 4 years. Cataract surgery can also be performed once inflammation is adequately controlled.
QIs acyclovir effective for CMV anterior uveitis?
A
No, it is not effective. CMV is not susceptible to acyclovir, valacyclovir, or penciclovir, so ineffectiveness of these drugs is an important sign of CMV infection. Ganciclovir (topical or systemic) or valganciclovir are first-line drugs; if CMV anterior uveitis is suspected, a change in antiviral medication is necessary.
After primary infection, CMV establishes latency in myeloid progenitor cells (monocyte/macrophage precursors). Reactivation of the virus in macrophages and dendritic cells of the anterior segment leads to anterior segment inflammation. It has also been suggested that infection at other sites may induce CMV reactivation in circulating monocytes. Upon reactivation, interferon-γ and interferon-β are released, initiating the inflammatory cascade.
Effects on Corneal Endothelial Cells and Pathophysiology of Endotheliitis
Linear KP (keratic precipitates): Horizontal linear or map-like deposits reflecting localized viral infection and inflammation of endothelial cells.
Coin-shaped KP (KP corrals): Characteristic pattern of inflammatory cells accumulating in a ring-like fashion around activated endothelial cells.
Progressive decrease in endothelial cell density: Direct infection-induced cell death combined with secondary inflammatory damage leads to a gradual decline in endothelial cell count over time.
Corneal decompensation: When endothelial cell count falls below the compensatory threshold, corneal stromal edema and opacity occur, potentially requiring corneal transplantation.
Without treatment, progressive loss of endothelial cell density continues, with risk of eventual progression to bullous keratopathy.
Angle obstruction by inflammatory cells and debris: Transient blockage of outflow pathways during inflammation.
Peripheral anterior synechiae formation: Repeated inflammation leads to anterior synechiae in the angle.
Steroid-induced intraocular pressure elevation: The therapeutic agent itself can contribute to increased IOP.
In the PSS type, normal to slightly low intraocular pressure is often maintained during the interictal period, but with repeated attacks, irreversible damage to the trabecular meshwork accumulates, leading to chronic ocular hypertension and glaucomatous visual field loss.
In a 66-year-old immunocompetent woman with recurrent hypertensive anterior uveitis, anterior chamber paracentesis revealed CMV-DNA in the aqueous humor at 25,675 copies/mL. Combination therapy with topical ganciclovir 0.15% (4 times daily), oral valacyclovir 1 g (twice daily), and topical steroids resulted in resolution of inflammation and intraocular pressure control, stabilizing at a final IOP of 12 mmHg 2).
In a two-round Delphi survey involving 100 international uveitis specialists from 21 countries, 75 (75%) completed the survey 1). Although many areas in the diagnosis and treatment of CMV anterior uveitis lacked consensus, the following key agreements were reached:
Treatment: 85% agreed to initiate topical antiviral therapy; 70% chose ganciclovir gel 0.15%
Long-term management: 84% supported tapering topical steroids over up to 12 months
However, international consensus on treatment and diagnostic criteria for PCR-negative cases remains unestablished, and further evidence accumulation is needed 1).
International unification of diagnostic criteria: Discrepancy between research criteria (PCR mandatory) and clinical criteria (sensitivity priority)
Comparison of topical vs. systemic therapy: Oral valganciclovir has been reported to be advantageous for corneal endothelial cell protection, but stepwise transition from topical to systemic therapy may increase recurrence risk
Optimization of long-term prophylactic therapy: Overcoming the high recurrence rate (up to 80%) after discontinuation
Corneal endothelial cell protection strategies: Maintaining endothelial cell density through early intervention and avoiding corneal transplantation
Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, et al. The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 2-global current practice patterns for the management of Cytomegalovirus anterior uveitis. Eye (Lond). 2024;38(1):68-75. doi:10.1038/s41433-023-02631-8. PMID:37419958; PMCID:PMC10764804.
Romano J, Godinho G, Chaves J, Oliveira N, Sousa JP.. Cytomegalovirus-Induced Hypertensive Anterior Uveitis: Diagnostic Challenge in an Immunocompetent Patient. Cureus. 2024;16(1):e52826. doi:10.7759/cureus.52826. PMID:38406050; PMCID:PMC10884362.