Cytomegalovirus (CMV) is a DNA virus belonging to the herpesvirus family. Cytomegalovirus corneal endotheliitis is a disease in which reactivation of this cytomegalovirus causes inflammation of the corneal endothelial cells 4). It is characterized by corneal edema with keratic precipitates (KPs) and elevated intraocular pressure. It is usually unilateral and can occur in immunocompetent individuals.
The seroprevalence of cytomegalovirus is high worldwide, ranging from 45% to 100%. After primary infection, the virus establishes latent infection in the trabecular meshwork and ciliary body. Most ocular symptoms in immunocompetent individuals are due to reactivation of latent virus. The Japanese Corneal Endotheliitis Study reported 109 cases. It is more common in middle-aged and older men (mean age 66.9 years, 80.2% male), with many reports from Asian countries.
Corneal endotheliitis is classified into four types based on the distribution pattern of KPs 4): linear, sectoral, disciform, and diffuse. In cytomegalovirus, coin-shaped or linear KPs are characteristic 4). In the Japanese Corneal Endotheliitis Study, coin-shaped KPs were observed in 70.6% of cases.
QHow does cytomegalovirus corneal endotheliitis differ from cytomegalovirus anterior uveitis?
A
Cytomegalovirus corneal endotheliitis and cytomegalovirus anterior uveitis are both disease spectra resulting from reactivation of cytomegalovirus. Corneal endotheliitis is primarily characterized by KPs and corneal edema, while anterior uveitis is primarily characterized by inflammation in the anterior chamber. The two often coexist, and elevated intraocular pressure is a common feature. It has become clear that some cases of Posner-Schlossman syndrome and Fuchs heterochromic iridocyclitis are caused by cytomegalovirus. An international Delphi survey also agreed that unilaterality and elevated intraocular pressure are specific findings of cytomegalovirus anterior segment infection 3).
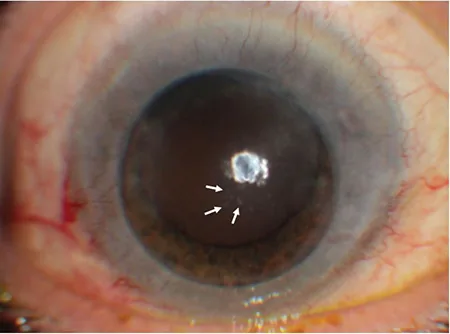
Büyüktepe TÇ, Karaca EE, Özdek Ş. Cytomegalovirus Endotheliitis After Penetrating Keratoplasty. Turk J Ophthalmol. 2020 Oct 30;50(5):304-307. Figure 3. PMCID: PMC7610052. License: CC BY.
Round, white keratic precipitates cluster near the center of the cornea, accompanied by surrounding stromal edema. This shows the coin-shaped KPs and surrounding edema characteristic of CMV corneal endotheliitis.
The main complaints are decreased vision and photophobia in one eye. When corneal edema leads to blister formation, eye pain and foreign body sensation may occur. Symptoms are nonspecific, making it difficult to differentiate from other intraocular inflammations. Recurrent episodes are characteristic. Treatment with steroid eye drops alone does not improve the condition or provides only temporary improvement.
Small to medium-sized non-granulomatous KPs are arranged in a coin-like or linear pattern 4). They commonly occur in Arlt’s triangle but can also appear in other areas. In typical cases, corneal edema starts from the periphery and progresses toward the center 4). Corneal infiltration and neovascularization are absent 4). Over time, the coin-shaped lesions lose their distinct morphology and become difficult to distinguish from ordinary KPs 4). Therefore, this finding is not essential for diagnosis.
Anterior chamber and intraocular pressure findings
Anterior chamber inflammation is mild compared to corneal findings 4). Elevated intraocular pressure occurs secondary to trabeculitis and may progress to secondary glaucoma4). Posterior synechiae are rare. A decrease in corneal endothelial cells is observed. In advanced cases, irreversible corneal endothelial dysfunction may develop 4).
In vivo confocal microscopy (IVCM) reveals characteristic findings on the corneal endothelial surface. Large endothelial cells with a central hyperreflective area and a surrounding hyporeflective halo, resembling an “owl’s eye,” are observed. This finding is specific to cytomegalovirus infection and is also useful for monitoring treatment response.
Reactivation of cytomegalovirus is the main cause. Both viral infection and immune response are involved in the pathogenesis 4). In vitro studies using cultured cells have confirmed that human cytomegalovirus infects and replicates in corneal endothelial cells and trabecular meshwork cells 4).
Risk factors include a history of corneal transplantation and local immunosuppression due to steroid eye drops. Reports are more frequent from Asian countries, particularly Japan and China, suggesting a racial predisposition.
Detection of cytomegalovirus DNA by PCR testing of aqueous humor is essential for definitive diagnosis 4). At the same time, it is necessary to confirm that HSV DNA and VZV DNA are negative 4). PCR testing may show viral load falling below the detection limit in the later stages of the disease 4). Therefore, testing early in the infection is desirable. Measurement of copy number by real-time PCR is useful for assessing treatment response 4).
According to the diagnostic criteria of the Corneal Endotheliitis Study Group, this condition is classified as type 2 4). Endotheliitis with positive cytomegalovirus DNA and coin-shaped lesions/linear keratic precipitates is typical cytomegalovirus corneal endotheliitis 4). Cases with local corneal edema with keratic precipitates plus two of the following findings—recurrent anterior uveitis, high intraocular pressure, secondary glaucoma, or decreased corneal endothelial cell count—are classified as atypical cytomegalovirus corneal endotheliitis 4).
QWhy is cytomegalovirus corneal endotheliitis often missed?
A
Initial findings of intraocular inflammation are often treated only with steroid eye drops. Because steroids temporarily improve inflammation, it is difficult to reach a diagnosis of cytomegalovirus. Steroid monotherapy can suppress local immunity and worsen viral activity. In fact, a case has been reported in which a patient was treated with methotrexate and steroids for several years as HLA-B27-positive anterior uveitis, and cytomegalovirus was first detected by aqueous humor PCR1). In unilateral hypertensive anterior uveitis that does not respond to steroids, PCR testing should be actively performed1).
Steroids: 0.1% fluorometholone eye drops are used concomitantly4). 77% of specialists start 1% prednisolone acetate 4 times daily for 1-2 weeks and then taper3).
Systemic Treatment
First-line: Valganciclovir 900 mg twice daily (treatment dose) tapered to 900 mg once daily4)
Maintenance therapy: Valganciclovir 450 mg once or twice daily for up to 12 months3)
If recurrence occurs twice or more per year: 88% of specialists recommend long-term topical antiviral therapy3).
Results of an international Delphi survey (75 specialists) showed that 70% chose ganciclovir gel 0.15% as first-line topical treatment3). 78% chose oral valganciclovir as first-line systemic treatment3). Opinions were divided on the timing of systemic administration: 33% for routine combination, 48% only for severe or refractory cases3).
Treatment Stage
Regimen
Acute phase (topical)
GCV 0.15% gel 3-5 times daily3)
Acute phase (systemic)
VGCV 900 mg twice daily4)
Maintenance phase (topical)
GCV 0.15% gel twice daily3)
Maintenance phase (systemic)
VGCV 450 mg 1-2 times daily3)
For cases with elevated intraocular pressure, glaucoma eye drops are used concomitantly4). 79% of specialists choose beta-blockers as first-line therapy3). Tapering of steroid eye drops over up to 12 months is supported by 84% of specialists3).
Self-prepared ganciclovir eye drops are made by dissolving intravenous ganciclovir in saline in a clean room of the pharmacy department4). Because they are easily degraded, storage in a cool, dark place and use within 1-2 weeks is recommended4).
In the Japanese Corneal Endotheliitis Study, combined systemic and topical therapy was most effective, but no statistically significant difference was observed. After treatment, 36% experienced recurrence, and 5.8% did not respond to any treatment. Because it is a chronic and recurrent disease, regular follow-up is necessary during dose reduction or after discontinuation4). If an increase in KP or elevated intraocular pressure is observed, treatment should be resumed4). 92% of specialists consider clinical monitoring sufficient for evaluating treatment efficacy3).
For cases that progress to irreversible corneal edema (bullous keratopathy), corneal endothelial transplantation such as DSAEK is performed4). Because reactivation of cytomegalovirus after transplantation is a concern, maintenance antiviral therapy is important4).
If intraocular pressure control is insufficient for secondary glaucoma, glaucoma surgery should be considered. A 61-year-old man who had been misdiagnosed with HLA-B27 anterior uveitis underwent simultaneous cataract surgery and trabeculectomy1). Intraoperative aqueous humor PCR detected a high level of cytomegalovirus DNA at 3×10⁶ copies/mL 1). One month after starting valganciclovir, visual acuity recovered to 20/20 and corneal edema completely resolved 1).
QWhat is the monitoring for side effects of systemic antiviral therapy?
A
During systemic administration of valganciclovir, there is a risk of renal dysfunction and blood abnormalities (bone marrow suppression, pancytopenia). In a Delphi survey, 87% of experts recommended monitoring serum creatinine and blood counts 2 to 4 times per year 3). If there is a history of renal impairment, dose adjustment and more frequent monitoring are required. If bone marrow suppression or nephrotoxicity occurs, systemic administration should be discontinued.
The pathophysiology of cytomegalovirus in the eye is presumed to be similar to HSV corneal endotheliitis. Latent cytomegalovirus forms reservoirs in the trabecular meshwork and ciliary body. It periodically reactivates, releasing small amounts of virus into the anterior chamber. It has been proposed that anterior chamber-associated immune deviation (ACAID) may be involved in the pathogenesis of cytomegalovirus corneal endotheliitis.
Histologically, it is characterized by mild stromal edema with loss of corneal endothelial cells. No significant inflammatory infiltration is observed in the corneal stroma. There is a significant correlation between the cytomegalovirus viral load in the anterior chamber and the severity of anterior segment inflammation. The grade of anterior chamber cells, intraocular pressure elevation, corneal endothelial cell loss, and recurrence frequency correlate with viral load.
QWhat happens if cytomegalovirus corneal endotheliitis develops after LASIK surgery?
A
In cytomegalovirus corneal endotheliitis after LASIK, corneal endothelial dysfunction and elevated intraocular pressure cause fluid accumulation between the flap layers. This condition is called interface fluid syndrome (IFS) 2). In IFS, Goldmann applanation tonometry over the flap shows falsely low values, so measurement on the peripheral cornea outside the flap is recommended 2). In a reported case of a 35-year-old woman, she had been followed for 16 years as Posner-Schlossman syndrome2). Nine years after LASIK, she developed IFS, and aqueous humor PCR detected cytomegalovirus DNA (26×10⁹ copies/mL) 2). IFS resolved one week after starting valganciclovir 2). Trabeculectomy was performed for poor intraocular pressure control 2).
In an international Delphi survey on the management of cytomegalovirus anterior segment infection, consensus was not reached on many items from diagnosis to treatment 3). In particular, opinions among experts differ regarding the criteria for systemic antiviral drug administration and treatment duration 3). For cases complicated by endotheliitis, a regimen of 0.5–2% topical ganciclovir 6 or more times daily for 4 weeks, or valganciclovir 900–1,800 mg twice daily for 4 weeks, is recommended by meta-analysis 3).
The biggest challenge in treating this disease is the lack of an approved therapeutic drug covered by insurance 4). Without appropriate antiviral therapy, severe visual impairment due to bullous keratopathy or secondary glaucoma may occur 4). Regulatory approval and insurance coverage of a safe therapeutic drug are desired 4).
Tendolkar S, Murthy SI, Bhatia P, Senthil S. Cytomegalovirus endotheliitis with recurrent anterior uveitis and secondary glaucoma misdiagnosed as HLA-B27 uveitis. BMJ Case Rep. 2021;14(2):e240061. doi:10.1136/bcr-2020-240061. PMID:33608341; PMCID:PMC7898841.
Tendolkar S, Murthy SI, Chandran K, Joseph J. Acute interface fluid syndrome after laser in situ keratomileusis in a case of cytomegalovirus (CMV) endotheliitis and secondary glaucoma. BMJ Case Rep. 2021;14:e236742. doi:10.1136/bcr-2020-236742.
Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, et al. The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 2-global current practice patterns for the management of Cytomegalovirus anterior uveitis. Eye (Lond). 2024;38(1):68-75. doi:10.1038/s41433-023-02631-8. PMID:37419958; PMCID:PMC10764804.