In 1906, Austrian ophthalmologist Ernst Fuchs reported 38 cases presenting with iris heterochromia, cyclitis, and cataract. Fuchs heterochromic iridocyclitis (FHI) is also called Fuchs uveitis syndrome (FUS). It is a unilateral uveitis characterized by the triad of iris heterochromia, iridocyclitis, and cataract, commonly occurring in the 20s to 40s with no gender difference.
FHI is reported to account for 2–11% of all uveitis cases 2). In a survey from the Uveitis Clinical Practice Guidelines (3,055 cases), it accounted for 0.5% (15 cases) 3). The prevalence may be underestimated; in Japanese individuals, heterochromia is less noticeable due to brown irises, leading to delayed diagnosis 7). Most cases are unilateral, with bilateral involvement in only about 10–13% 2).
FHI itself follows a benign course unless secondary glaucoma develops, and often does not require treatment. However, secondary glaucoma is the most vision-threatening complication of FHI, and its incidence increases with longer follow-up.
QWhy is FHI difficult to diagnose in Japanese patients?
A
Because Japanese individuals have brown irises, differences in iris color between eyes are less apparent. Instead of simple heterochromia, attention should be paid to the iris collarette and iris crypts becoming less distinct compared to the healthy eye, and to diffuse iris atrophy centered on the minor iris circle. Comparing with the fellow eye before dilation is a key diagnostic point.
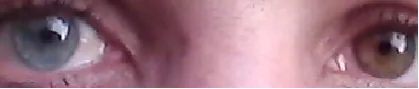
Difference in iris color between both eyes (heterochromia iridis). The affected eye shows decreased iris pigment due to iris stromal atrophy, resulting in a lighter iris color compared to the fellow eye. This is one of the three main signs of FHI.
Unlike other forms of anterior uveitis, FHI patients do not experience pain, redness, or photophobia. Many patients remain asymptomatic for years before seeking medical attention.
Vision loss due to cataract: FHI is often discovered as rapidly progressive unilateral cataract in young individuals.
Floaters: Caused by vitreous opacities due to inflammatory debris, mainly in the anterior vitreous.
Present in 75–90% of patients. Usually, the lighter-colored eye is the affected one. In Japanese individuals, due to brown irises, it appears as diffuse iris atrophy. It is important to compare with the fellow eye without dilation.
Stellate Keratic Precipitates (KPs)
White, fine stellate keratic precipitates diffusely distributed over the entire corneal endothelium. Unlike other types of uveitis, they are evenly distributed up to the superior cornea. This is the most specific finding for diagnosis.
Iridocyclitis and Cataract
Anterior chamber inflammation is chronic and mild. Cataract progresses faster than in other uveitis. Posterior synechiae do not occur (most important differentiating feature). Koeppe/Busacca iris nodules may be present.
Heterochromia iridis: Seen in 75–90% of patients 2). Usually, the lighter-colored eye is the affected eye. “Reverse heterochromia” has also been reported, where the anterior iris stroma disappears and the dark pigment epithelium becomes exposed.
Iris atrophy: Diffuse iris atrophy with loss of iris crypts, resulting in a smooth stromal structure (moth-eaten appearance). Atrophy often precedes heterochromia. In Japanese and other Asian patients, heterochromia is often not obvious due to brown irises; it is important to focus on the color tone of the pupillary zone (inner iris ring) relative to the iris collarette. Comparison with the fellow eye without dilation is important.
Iris nodules: Koeppe nodules (at the pupillary margin) or Busacca nodules (in the iris stroma) may be seen 3). However, posterior synechiae do not occur.
Detailed Findings of KP, Anterior Chamber, and Angle
Stellate KP: White, fine stellate, interconnected by fibrin bridges 2). Unlike typical uveitis where KP are concentrated in the inferior Arlt triangle, in FHI they are diffusely distributed over the entire corneal endothelium. Cystoid macular edema (CME) is usually absent.
Angle neovascularization: Gonioscopy often reveals new vessels crossing the trabecular meshwork2). These fragile vessels may rupture with anterior chamber paracentesis or gonioscopic compression, causing hyphema from the opposite angle (Amsler sign).
Posterior subcapsular cataract (PSC): Accounts for about three-quarters of lens opacities in FHI patients 2). Cataract progresses faster than in other uveitis.
Russell bodies: Small, highly refractive crystals on the iris surface, which are aggregates of globular immunoglobulins 2).
Chorioretinal scars: Seen in 7–65% of cases, but a definitive association with toxoplasmosis has not been proven.
Secondary glaucoma (10–59%): Open-angle type. The most vision-threatening complication2)
Amsler sign: Bleeding from the angle during anterior chamber paracentesis. Due to fragility of angle neovascularization
Vitreous opacity: Mild to moderate. Severe cases require vitrectomy
QIf there is posterior synechia, is it not FHI?
A
That is correct. In FHI, posterior synechia does not occur as a rule, and the presence of posterior synechia is an important finding against FHI. If posterior synechia is observed, differentiation from other diseases such as sarcoidosis, herpetic iritis, and CMV iridocyclitis is necessary.
The exact etiology of FHI remains unknown and is considered multifactorial. Historically, many hypotheses have been proposed, including degenerative disease, Toxoplasma/HSV infection, immune abnormality, and vascular abnormality (from Amsler sign), but most are now refuted.
HSV, Chikungunya virus: Viral DNA/RNA has been isolated from aqueous humor in some reports, but these remain at the case report level
Sympathetic dysfunction hypothesis: A theory assuming decreased innervation to iris stromal melanocytes, but among 1,746 cases, only 25 (1.4%) were associated with Horner syndrome, making it unlikely
Toxoplasmosis: The prevalence of chorioretinal scars is high, but a significant association with humoral or cellular immunity has not been proven
In recent years, the association with rubella virus has gained attention as the most plausible hypothesis. A review by Mohamed & Zamir (2005) suggested that persistent low-grade intraocular infection may occur after fetal or childhood rubella infection7). de Groot-Mijnes et al. (2006) detected rubella virus RNA (genome) by PCR in aqueous humor of FHI patients and confirmed intraocular antibody production using the Goldmann-Witmer coefficient. Intraocular antibody production against RV was found in 48 of 64 European cases (75%)8). The declining incidence of FHI in regions with rubella vaccination also supports the rubella hypothesis.
In Asia, CMV infection has been reported as FHI-like inflammation. Chee & Jap (2008) compared CMV-positive FHI-like anterior uveitis with CMV-negative FHI and Posner-Schlossman syndrome, showing that high intraocular pressure and anterior chamber cells are common, but FHI findings (stellate KP, iris atrophy) are similar to CMV-negative cases9). The International Task Force on CMV Anterior Uveitis (TITAN 2024) emphasized that identification of CMV-DNA by aqueous humor PCR is useful for differentiation4).
The reported frequency of secondary glaucoma associated with FHI ranges widely from 10% to 59%, with higher rates in long-term follow-up 2). The uveitis clinical practice guidelines report 10–20% 3). The following factors have been reported to increase risk:
The diagnosis of FHI is based on a combination of clinical findings. There is no definitive diagnostic test. The diagnostic criteria proposed by La Hey et al. (1994) 10) are often referenced. Diagnosis is made only after excluding other diseases.
Comparison with the fellow eye without dilation: Essential for confirming iris atrophy. Atrophy becomes unclear after dilation.
Anterior chamber PCR: Useful for identifying rubella virus and CMV DNA. Particularly used for CMV differentiation when accompanied by high intraocular pressure9)
Fluoresceiniris angiography: Evaluation of iris vascular abnormalities and Amsler sign
Gonioscopy: Confirmation of open angle and neovascularization
Although not mandatory in all cases, anterior chamber PCR is useful when accompanied by high intraocular pressure, when differentiation between steroids and antiviral drugs is needed for treatment, or when differentiation between CMV and FHI is difficult9). Particularly in Asians, there are many reports of CMV-positive FHI-like inflammation, and differentiation can change treatment strategy.
The anterior chamber symptoms of FHI hardly respond to steroid eye drops, and long-term use increases the risk of steroid-induced cataract and steroid-induced glaucoma. The uveitis treatment guidelines state that “observation without steroid eye drops” is the principle3). Since posterior synechiae do not occur, mydriatics are also unnecessary.
Cataracts associated with FHI have better surgical outcomes compared to other uveitis. The uveitis treatment guidelines state that “even if active inflammation is present, cataract surgery rarely exacerbates inflammation”3).
Phacoemulsification + posterior chamber IOL implantation is standard. Postoperative inflammation is relatively mild
During surgery, attention should be paid to Amsler’s sign (bleeding from the angle), and low intraocular pressure perfusion and adequate use of viscoelastic materials are recommended
Heterochromia may progress after surgery, so preoperative explanation is necessary
If there is a possibility of filtration surgery for secondary glaucoma, perform cataract surgery via corneal incision while preserving the superior conjunctiva.
When intraocular pressure control is insufficient with medication, surgical treatment is necessary. The 5th edition of the Japanese Glaucoma Practice Guidelines recommends trabeculectomy (with antimetabolites) or tube shunt surgery for uveitic glaucoma5).
Surgical outcomes for uveitic glaucoma including FHI are shown below.
Trabeculectomy (with MMC): In uveitic eyes, the success rate tends to be lower due to subconjunctival scarring. 1-year success rate 58–90.9%, 4-year success rate 62.3%2)
Glaucoma drainage device (GDD): Options include Ahmed valve, Baerveldt implant, and Molteno implant. Particularly for Baerveldt, a favorable 2-year success rate of 91.7% has been reported2). It is especially useful in cases with conjunctival scarring.
GATT: Limited efficacy for FUS-related glaucoma (all 4 cases unsuccessful in Yuksel Elgin 2025)1)
Cyclophotocoagulation (diode, Nd:YAG laser): Suppresses aqueous humor production but carries a risk of exacerbating inflammation. It is considered a last resort for eyes with poor visual prognosis2)
In principle, they should not be used. Mild anterior chamber reaction in FHI hardly responds to steroid eye drops, and long-term use increases the risk of steroid-induced cataract and steroid-induced glaucoma. Since posterior synechiae do not occur, mydriatics are also unnecessary. The Uveitis Clinical Practice Guidelines also state that “unnecessary treatment should not be performed” 3).
The theory that persistent low-grade infection is established in the anterior chamber after rubella infection during the fetal or childhood period is currently the most supported 7, 8). Evidence includes detection of rubella virus RNA in aqueous humor, demonstration of intraocular antibody production by the Goldmann-Witmer coefficient, and a decreasing trend of FHI in regions where rubella vaccination is widespread 8).
CD8+ T cell-dominant chronic T cell-mediated inflammation induces stellate keratic precipitates, iris atrophy, and neovascularization
Persistent immune attack on iris melanocytes causes depigmentation (iris atrophy)
Secondary glaucoma associated with FHI is of the open-angle type, and the following mechanisms contribute to elevated intraocular pressure2).
Trabeculitis: Inflammatory cell infiltration predominantly by lymphocytes and plasma cells. Accumulation of inflammatory cells and debris, along with secondary scarring, obstructs the aqueous outflow pathway 6)
Angle neovascularization (rubeosis): Fragile vessels cause Amsler’s sign (hyphema)
Irreversible scarring of the posterior trabecular meshwork: Reason why trabeculotomy procedures such as GATT are less effective 1)
Collapse of Schlemm’s canal: Permanently increased resistance to aqueous outflow
Irreversible structural changes: In many cases, glaucoma persists even after inflammation subsides, suggesting that not only reversible inflammatory obstruction but also irreversible structural changes in the trabecular meshwork occur.
In FHI, posterior synechiae, peripheral anterior synechiae (PAS), and pupillary block are usually absent, so angle-closure mechanism is not common; the main cause is trabecular meshwork damage in open-angle glaucoma5). Typically, glaucoma in FHI tends to persist even after inflammation subsides and does not respond to steroids 2). This helps differentiate it from steroid-induced glaucoma.
Gonioscopy reveals an open angle and neovascularization crossing the trabecular meshwork2). Irisfluorescein angiography may show leakage from iris vessels or ischemic changes.
General mechanisms of intraocular pressure elevation in uveitis
For reference, the following mechanisms may also be involved in intraocular pressure elevation associated with uveitis2):
Accumulation of inflammatory debris in the trabecular meshwork
Trabecular meshwork edema
Angle nodules
Peripheral anterior synechiae (PAS)
Steroid medications
Neovascularization
Pupillary block due to posterior synechiae
Among these, posterior synechiae, PAS, and pupillary block are usually not involved in FHI; trabeculitis and structural changes are the main causes of intraocular pressure elevation.
Chronic low-grade inflammation causes degeneration of lens epithelial cells, leading to posterior subcapsular cataract (PSC). About three-quarters of lens opacities in FHI patients are posterior subcapsular, and progression is faster than in other types of uveitis. Cataracts progress even without steroid treatment, so regular follow-up is necessary.
Yuksel Elgin & Hepokur (2025) reported GATT for FUS-related glaucoma in 4 cases. All surgeries were unsuccessful, with 3 cases requiring trabeculectomy with MMC and 1 case requiring diode laser cyclophotocoagulation after an average of 6 months 1). In FUS glaucoma, scarring of the posterior trabecular meshwork is the main cause, suggesting that GATT may not achieve sufficient intraocular pressure reduction.
Etiological Elucidation by Multiplex PCR of Aqueous Humor
Advances in multiplex PCR technology have enabled accurate detection and differentiation of rubella virus, CMV, and HSV in the anterior chamber. The usefulness of antiviral therapy (ganciclovir eye drops, valganciclovir oral) is being investigated in Asian CMV anterior uveitis4).
Prospects for Minimally Invasive Glaucoma Surgery (MIGS)
Implant devices such as iStent and Hydrus are at risk of occlusion by inflammatory debris, but preliminary promising results have been reported for canaloplasty. Establishing a MIGS algorithm specific to FHI glaucoma remains a challenge.
Continuous monitoring of epidemiological changes in FHI associated with rubella vaccination is ongoing, with reports of a decreasing trend in FHI incidence among younger generations 7).
Large-scale studies to clarify the superiority of GDD versus filtration surgery in FHI-related glaucoma
Elucidation of the etiological role of rubella virus and CMV, and investigation of the usefulness of antiviral therapy
Establishment of a FHI-specific glaucoma treatment algorithm
QIs minimally invasive glaucoma surgery (MIGS) effective for FHI glaucoma?
A
At present, the effectiveness of MIGS for FHI glaucoma is considered limited. In a report of 4 GATT cases, all were unsuccessful 1). In FHI glaucoma, scarring of the posterior trabecular meshwork may be involved, and angle surgery alone may not provide sufficient effect. Implant devices such as iStent and Xen are at risk of occlusion by inflammatory debris.
Yuksel Elgin C, Hepokur M.. Highlighting the limited efficacy of gonioscopy-assisted transluminal trabeculectomy in Fuchs uveitis syndrome: a case series. BMC Ophthalmol. 2025;25(1):180. doi:10.1186/s12886-025-04035-6. PMID:40197273; PMCID:PMC11978193.
Bodh SA, Kumar V, Raina UK, Ghosh B, Thakar M.. Inflammatory glaucoma. Oman J Ophthalmol. 2011;4(1):3-9. doi:10.4103/0974-620x.77655. PMID:21713239; PMCID:PMC3110445.
Chee SP, Jap A, Engelen S, et al. CMV anterior uveitis: what we have learnt. The International Taskforce for Anterior segment Novel therapies (TITAN) report 2. Graefes Arch Clin Exp Ophthalmol. 2024;262(5):1415-1428.
European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. The British journal of ophthalmology. 2021;105(Suppl 1):1-169. doi:10.1136/bjophthalmol-2021-egsguidelines. PMID:34675001.
Mohamed Q, Zamir E.. Update on Fuchs’ uveitis syndrome. Curr Opin Ophthalmol. 2005;16(6):356-363. doi:10.1097/01.icu.0000187056.29563.8d. PMID:16264346.
de Groot-Mijnes JD, de Visser L, Rothova A, Schuller M, van Loon AM, Weersink AJ.. Rubella virus is associated with fuchs heterochromic iridocyclitis. Am J Ophthalmol. 2006;141(1):212-214. doi:10.1016/j.ajo.2005.07.078. PMID:16387009.
Soon-Phaik Chee, Aliza Jap. Presumed Fuchs Heterochromic Iridocyclitis and Posner-Schlossman Syndrome: Comparison of Cytomegalovirus-Positive and Negative Eyes. American Journal of Ophthalmology. 2008;146(6):883-889.e1. doi:10.1016/j.ajo.2008.09.001.
La Hey E, de Jong PT, Kijlstra A.. Fuchs’ heterochromic cyclitis: review of the literature on the pathogenetic mechanisms. Br J Ophthalmol. 1994;78(4):307-312. doi:10.1136/bjo.78.4.307. PMID:8199120; PMCID:PMC504771.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}