Uveitic glaucoma (UG) is a disease in which persistent or recurrent elevation of intraocular pressure associated with uveitis leads to glaucomatous optic neuropathy and visual field loss. It involves open-angle mechanisms primarily due to trabecular meshwork obstruction by inflammatory products, and angle-closure mechanisms primarily due to increased outflow resistance from peripheral anterior synechiae (PAS). Mixed types with both mechanisms are common 1, 2).
In 1813, Joseph Beer first reported the association between uveitis and glaucoma as “arthritic iritis” 1). In 1891, Priestley Smith published the first modern classification 1).
The incidence of uveitis is 17–52.4 per 100,000 population 2). The incidence of secondary glaucoma in uveitis patients is 10–20%, reaching 46% in chronic uveitis1, 2). In adults with non-infectious uveitis, the annual incidence of intraocular pressure ≥21 mmHg (OHT) is 14.4%, and ≥30 mmHg is 5.1%/year 2). Glaucoma is the most common cause of permanent vision loss in anterior uveitis, accounting for 30.1% 2).
The following diseases have a particularly high risk of developing UG.
Posner-Schlossman syndrome (PSS): Unilateral, recurrent iritis with acute intraocular pressure elevation. During attacks, IOP reaches ≥40 mmHg, rarely exceeding 60 mmHg. Corneal edema is mild relative to the IOP elevation, and during remission, the affected eye often has lower IOP than the fellow eye. The angle is open, with no PAS or nodules. CMV is detected in the aqueous humor in some cases, overlapping partially with CMV iritis.
Herpetic uveitis (HSV keratouveitis): IOP elevation occurs in 28%, glaucomatous damage in 10%, and IOP elevation persists for an average of 2 months 1).
Fuchs heterochromic iridocyclitis (FHIC): Typically occurs at age 20–40, usually unilateral (13% bilateral) 1). Characterized by diffuse distribution of fine white keratic precipitates. In Japanese patients, heterochromia is inconspicuous, and diffuse iris atrophy is common. Glaucoma complication rate ranges from 13–59%, increasing with long-term follow-up.
Juvenile idiopathic arthritis (JIA)-associated uveitis: In children, asymptomatic chronic anterior uveitis is predominant, often leading to delayed detection. JIA-associated uveitis has a significantly higher glaucoma incidence than idiopathic uveitis9).
Not all uveitis patients develop glaucoma. Overall, secondary glaucoma occurs in 10–20%. However, in chronic uveitis it reaches 46% 1), so regular IOP measurement and follow-up are essential. Pediatric uveitis associated with juvenile idiopathic arthritis often progresses asymptomatically, requiring regular screening 8).
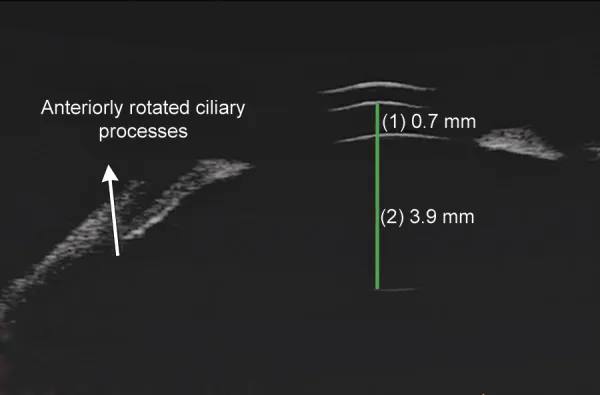
Parivadhini A, et al. Management of Secondary Angle Closure Glaucoma. J Curr Glaucoma Pract. 2014. Figure 1C. PMCID: PMC4741163. License: CC BY.
Ultrasound biomicroscopy (UBM) image shows forward rotation of ciliary processes and associated shallow anterior chamber. This corresponds to “forward rotation of ciliary processes” discussed in section “2. Main symptoms and clinical findings”.
In JIA-associated uveitis and some cases of FHIC, subjective symptoms are often minimal, and elevated intraocular pressure and inflammatory findings are frequently discovered only during regular examinations.
Cornea: Keratic precipitates (KP; fine/mutton-fat), band keratopathy (chronic cases), dendritic lesions (herpetic)1). In FHIC, fine white KP are diffusely distributed; in PSS, small to medium-sized non-pigmented KP are seen sparsely from the central cornea downward.
Anterior chamber: Flare and cells. Fibrin and hypopyon in severe inflammation.
Iris: Stromal atrophy, iris nodules (Koeppe nodules / Busacca nodules), posterior synechiae, peripheral anterior synechiae (PAS), iris neovascularization (NVI) 1). In FHIC, diffuse iris atrophy leads to heterochromia. If posterior synechiae are circumferential, pupillary block occurs, resulting in iris bombé.
Angle: PAS (tent-like closure), angle nodules, trabecular meshworkhyperemia, neovascularization. In PSS, the angle is open, and the angle pigmentation of the affected eye is often lighter than that of the fellow eye.
Lens: Anterior capsule pigmentation, posterior subcapsular cataract1). In FHIC, complicated cataract progresses faster than in other uveitis.
Even if active inflammatory findings are scarce at examination, always check for signs of past inflammation. Keratic precipitates, PAS, angle nodules, and iris atrophy are important findings suggesting previous inflammation. Inquiring about the history of steroid eye drop use is also essential for differential diagnosis.
Intraocular pressure (IOP) varies depending on the degree and mechanism of inflammation. IOP decreases when ciliary body function is reduced, and increases when aqueous outflow is obstructed. During an attack of PSS, IOP can reach 40–70 mmHg, but during remission it is often lower than that of the fellow eye.
IOP elevation in UG involves both open-angle and closed-angle mechanisms, and mixed types also exist 1, 2). Gonioscopic angle observation is essential for estimating the mechanism (see “Diagnosis and Examination Methods” section).
The main mechanisms of intraocular pressure elevation are classified into the following seven categories.
Steroids can cause UG in up to 42% of cases2). Risk factors for steroid-induced intraocular pressure elevation include a history of primary open-angle glaucoma (POAG), family history of glaucoma, rheumatoid arthritis (RA), children/elderly, and diabetes2).
Comparing fluocinolone implants with systemic therapy, the incidence of glaucoma over 6.9 years was 40% vs 8%, significantly higher with implants2). Differentiation from steroid-induced glaucoma is crucial for determining treatment strategy1, 3).
Approximately half of pediatric non-infectious uveitis cases are JIA-associated, and the JIA group has a statistically significantly higher incidence of glaucoma compared to the idiopathic uveitis group9). In the same study, a higher proportion of children with JIA-associated uveitis required trabeculectomy9). With the introduction of biologics (monoclonal anti-TNFα antibodies such as adalimumab), visual prognosis and complication rates have been improving in recent years9).
QCan steroid eye drops cause glaucoma?
A
Yes. Up to 42% of UG is attributed to steroids 2). In particular, with fluocinolone acetonide implants, 40% developed glaucoma over 6.9 years of observation (compared to 8% with systemic therapy) 2). Regular intraocular pressure measurement is essential during steroid use.
Diagnosis of UG requires both diagnosis of uveitis and elucidation of the mechanism of intraocular pressure elevation. Differentiation from steroid-induced glaucoma is particularly important 3).
Slit-lamp microscopy: Evaluate keratic precipitates (KP), anterior chamber flare/cells, and iris findings. Assess the degree of active inflammation.
Gonioscopy: Essential. Detect peripheral anterior synechiae (PAS), angle nodules, and neovascularization1, 2). Even if anterior chamber inflammation has subsided, signs of past inflammation (KP, PAS) can be identified.
Optical coherence tomography (OCT): Serial measurement of RNFL and ganglion cell layer (GCL) thickness. Since active uveitis may cause RNFL thickening leading to false-negative results, measurement during the quiescent phase is recommended 2).
OCT angiography: Allows evaluation of decreased vessel density in the optic nerve head and macula (currently at the pilot study stage) 2).
Anterior segment OCT (AS-OCT): Used for quantitative assessment of corneal thickness, iris, ciliary body, and angle 2). Since it cannot evaluate color information, gonioscopy is preferred for detecting angle nodules and neovascularization.
Ultrasound biomicroscopy (UBM): Useful when anterior segment observation is difficult due to corneal opacity, or when evaluation of the ciliary body is needed 2).
Systemic Examinations and Intraocular Fluid Analysis (Search for Cause)
ANA: Many JIA-associated uveitis cases are positive, and it is also used to determine screening intervals 8).
Aqueous humor PCR: Detection of HSV, VZV, CMV, and rubella virus. When CMV anterior uveitis is suspected, about 73% of international experts support diagnostic anterior chamber paracentesis7). If recurrent ocular hypertension occurs with a PSS-like clinical picture, consider CMV.
Since JIA-associated uveitis often progresses asymptomatically, screening by collaboration between pediatric rheumatologists and ophthalmologists is essential 8). Risk factors include oligoarticular or extended JIA, positive antinuclear antibody (ANA), age at onset ≤6 years, JIA duration ≤4 years, and no use of methotrexate or anti-TNFα agents 8). High-risk children should undergo ophthalmic screening every 3 months, moderate-risk every 6 months, and low-risk every 12 months 8).
If there is a history of steroid use, open angle, no angle abnormalities, and no other cause of elevated intraocular pressure, suspect steroid-induced glaucoma1, 3). Discontinuing or reducing steroids and observing changes in intraocular pressure is useful for differentiation.
In the treatment of UG, inflammation control is the top priority and should be performed in parallel with intraocular pressure reduction. Treatment of the underlying disease (anti-inflammatory therapy) is the highest priority, and we often encounter situations where differentiation from steroid-induced glaucoma is difficult due to long-term corticosteroid administration 3).
Biologics: Monoclonal anti-TNFα antibodies such as adalimumab improve inflammation control and visual prognosis in pediatric non-infectious uveitis including JIA-associated uveitis9).
Fluocinolone implant: The incidence of glaucoma is significantly higher compared to systemic therapy (40% vs 8%), so careful consideration of indications is needed in cases with high glaucoma risk2).
CMV-positive PSS: Antiviral therapy with valganciclovir/ganciclovir improves control. Early initiation of antiviral therapy (within 700 days) reduces the need for subsequent glaucoma surgery2). International expert consensus recommends 0.15% ganciclovir gel 3–4 times daily for about 1 month as initial treatment for CMV anterior uveitis, with valganciclovir 900 mg twice daily for 2–3 weeks if needed7). Maintenance therapy continues with ganciclovir gel 0.15% twice daily for up to 12 months7).
Miotics (pilocarpine) are contraindicated due to risks of promoting posterior synechiae, disrupting the blood-aqueous barrier (BAB), and worsening inflammation1). Omidenepag (EP2 receptor agonist) should also be used cautiously in inflamed eyes.
Drug class
Representative drug
Notes
Beta-blockers
Timolol, carteolol
First-line. Suppress aqueous humor production. Be aware of systemic side effects7)
Risk of inflammation exacerbation and CME. Useful in quiet eyes2)
Rho-kinase inhibitors
Ripasudil
Also suggested to have anti-inflammatory effects2)
Hyperosmotic agents
D-mannitol (intravenous)
Temporary intraocular pressure reduction in acute phase
Among PGAs, bimatoprost is reported to have a lower risk of inflammation than latanoprost2). For intraocular pressure management in CMV anterior uveitis, 79% of international experts choose beta-blockers as first-line therapy7). The sequence of IOP-lowering medications is considered in the order: beta-blockers/CAI eye drops → oral CAI → intravenous D-mannitol.
Nd:YAG laser peripheral iridotomy (LPI): Used for pupillary block. In UG, 62% become non-functional after 85 days, so performing at two or more sites is recommended2). Performing LPI during active inflammation tends to cause fibrin exudation and re-occlusion; therefore, it should be performed after inflammation has subsided as much as possible. In cases of repeated occlusion or under active inflammation, surgical peripheral iridectomy is indicated.
Approximately 30% of UG patients require surgery, and up to one-third undergo reoperation 2). Surgery is generally performed during the quiescent phase of inflammation. Since postoperative inflammation recurrence is the main cause of surgical failure, at least 3 months of inflammation control before surgery is desirable.
Trabeculectomy (TLE)
Indications: Cases where intraocular pressure is inadequately controlled with medication.
Features: Filtration surgery with mitomycin C (MMC-TLE) is standard. The scleral flap is securely sutured, and intraocular pressure is adjusted postoperatively with laser suture lysis.
Outcomes: MMC-TLE during the quiescent phase of inflammation has been reported to achieve outcomes comparable to primary open-angle glaucoma1, 10). Success rates: 91.7% at 12 months, 82.2% at 36 months, 66.5% at 120 months 2).
Cautions: Postoperative inflammation recurrence is the main cause of surgical failure. Be alert for hypotony due to overfiltration and reduced ciliary body function. When differentiation from steroid-induced glaucoma is difficult, outflow reconstruction surgery (trabeculotomy) may be chosen 3).
Surgical management of angle-closure UG: Goniosynechialysis (GSL) is performed for peripheral anterior synechiae, but the effect is inconsistent and PAS often recurs, making it difficult to achieve intraocular pressure reduction with GSL alone. GSL is usually combined with trabeculectomy or cataract surgery.
Cyclophotocoagulation: Last resort when other surgeries fail. Risk of hypotony 19%, phthisis bulbi2).
QCan pilocarpine eye drops be used for uveitic glaucoma?
A
No. Pilocarpine (miotic) is contraindicated in uveitic glaucoma1). It promotes posterior synechiae, disrupts the blood-aqueous barrier, and may worsen inflammation. Beta-blockers and CAIs are first-line for IOP reduction.
QHow many surgeries may be needed for uveitic glaucoma?
A
Up to one-third of UG patients require reoperation2). Postoperative inflammation recurrence is the main cause of surgical failure, and it is important to plan surgery during the quiescent phase. Tube shunt surgery is often chosen for reoperation.
The mechanisms of intraocular pressure elevation in UG are broadly classified into open-angle and angle-closure types. Mixed types with both mechanisms are also common 1, 2).
Open-Angle Mechanisms
Physical obstruction of the trabecular meshwork: Disruption of the blood-aqueous barrier (BAB) allows inflammatory cells and proteins to enter the anterior chamber, obstructing the trabecular meshwork1).
Trabeculitis: Swelling of the trabecular lamellae and endothelial cells narrows the pores. Chronic inflammation can lead to irreversible scarring 1). This is prominent in FHIC.
Schlemm’s canal collapse: Trabeculitis due to mononuclear cell infiltration can collapse Schlemm’s canal, causing intraocular pressure elevation 1).
Steroid-induced: Increased extracellular matrix production and cytoskeletal changes in trabecular meshwork cells increase outflow resistance.
Increased aqueous humor secretion: PGE1- and PGE2-mediated increased aqueous secretion and increased aqueous viscosity due to BAB disruption also contribute 1).
Angle-Closure Mechanisms
Pupillary block: When posterior synechiae involve the entire circumference, pupillary block occurs, leading to iris bombé and peripheral anterior synechiae (PAS), resulting in angle closure 1).
Ciliary body swelling: Inflammation-induced swelling and forward rotation of the ciliary body can close the angle 2).
Chronic PAS formation: Chronic inflammation leads to progressive PAS formation, resulting in chronic angle closure. 80% of patients with Vogt-Koyanagi-Harada disease (VKH) develop angle closure 2).
Angle neovascularization: Chronic inflammation can cause angle neovascularization, forming a fibrovascular membrane that closes the angle 1).
Acute (usually reversible): Primarily involves accumulation of inflammatory material in the trabecular spaces, trabecular lamellar edema, and ciliary body swelling 1). Intraocular pressure may normalize with resolution of inflammation.
Chronic (irreversible): Scar formation and membrane overgrowth in the anterior chamber angle occur1). Even after inflammation subsides, the condition requiring intraocular pressure-lowering medications or surgery persists.
7. Latest Research and Future Perspectives (Investigational Reports)
In a review by Halkiadakis et al. (2024), the XEN63 gel stent, which has a larger lumen (63 μm vs 45 μm) than XEN45, was reported to achieve an intraocular pressure of 16 mmHg at one year in refractory uveitic glaucoma2).
For occlusion of the XEN63 gel stent, a technique to restore patency via ab-externo revision using a 10-0 nylon probe has been reported5).
Tube exposure occurs in 7–14.3% of cases as a postoperative complication4). For Ahmed valve exposure with corneal melting and iris prolapse, repair using a multilayer closure technique (pericardial patch + capsule autograft + Tenon’s capsule transposition + conjunctival advancement) and limbal reconstruction with corneoscleral allograft have been reported4, 6).
Armstrong et al. (2024) reported a surgical technique combining tube exchange in the same quadrant with multilayer closure for cases of recurrent tube re-exposure, showing promising preliminary results6).
Ripasudil (Rho-kinase inhibitor) has shown efficacy in uveitic glaucoma in eyes using steroids, and its potential anti-inflammatory effects have also been reported2).
Micropulse cyclophotocoagulation is less invasive than conventional cyclophotocoagulation, and its safety in uveitic glaucoma has been reported2). It may reduce the risk of complications (hypotony, phthisis) associated with standard cyclophotocoagulation.
Early introduction of biologics (e.g., anti-TNFα antibodies) in pediatric non-infectious uveitis may suppress the risk of developing cystoid macular edema and glaucoma through improved inflammation control9). Recent cohort studies report that one-third of cases use biologics, with improved visual prognosis and complication rates compared to earlier cohorts9).
OCT angiography evaluation of optic disc and macular vessel density in UG is in a pilot study phase aiming for application in glaucoma diagnosis 2). Additionally, Mendelian randomization studies have reported a possible genetic causal relationship between uveitis and glaucoma2).
SonamA Bodh, Vasu Kumar, UshaK Raina, B Ghosh, Meenakshi Thakar. Inflammatory glaucoma. Oman J Ophthalmol. 2011;4(1):3. doi:10.4103/0974-620x.77655.
Halkiadakis I, Konstantopoulou K, Tzimis V, Papadopoulos N, Chatzistefanou K, Markomichelakis NN. Update on Diagnosis and Treatment of Uveitic Glaucoma. Journal of clinical medicine. 2024;13(5). doi:10.3390/jcm13051185. PMID:38592059; PMCID:PMC10931771.
Kandarakis SA, Doumazos L, Timpilis M, Karageorgiou G, Petrou P, Georgalas I. Limbal reconstruction in uveitic glaucoma patient with exposed Ahmed valve coincident with corneal melting and iris prolapse using multiple corneoscleral allografts. Romanian journal of ophthalmology. 2024;68(1):60-64. doi:10.22336/rjo.2024.12. PMID:38617728; PMCID:PMC11007568.
Marchese V, Randazzo V, Badalamenti R, Anastasi M. Reviving XEN63 Gel Stent Patency in Uveitic Glaucoma: A Novel Approach Using 10-0 Nylon Probe. Journal of current glaucoma practice. 2024;18(2):74-78. doi:10.5005/jp-journals-10078-1445. PMID:39144734; PMCID:PMC11320764.
Armstrong M, Wang J, Gorla M, Qiu M. Same-quadrant tube exchange and multiple-layer closure for recurrent tube erosion: Surgical technique description and preliminary results. American journal of ophthalmology case reports. 2024;36:102138. doi:10.1016/j.ajoc.2024.102138. PMID:39188856; PMCID:PMC11347064.
Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, et al. The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 2-global current practice patterns for the management of Cytomegalovirus anterior uveitis. Eye (Lond). 2024;38(1):68-75. doi:10.1038/s41433-023-02631-8. PMID:37419958; PMCID:PMC10764804.
Leinonen S. A Nordic screening guideline for juvenile idiopathic arthritis-related uveitis. Acta Ophthalmol. 2023;101(4):465-468. doi:10.1111/aos.15299. PMID:36458735.
Cann M, Ramanan AV, Crawford A, et al. Outcomes of non-infectious Paediatric uveitis in the era of biologic therapy. Pediatr Rheumatol Online J. 2022;20(1):47.
Kaburaki T, Koshino T, Kawashima H, Numaga J, Tomidokoro A, Shirato S, et al. Initial trabeculectomy with mitomycin C in eyes with uveitic glaucoma with inactive uveitis. Eye (London, England). 2009;23(7):1509-17. doi:10.1038/eye.2009.117-cme. PMID:19521438.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.