Sympathetic ophthalmia (SO) is a rare autoimmune disease that causes bilateral granulomatous panuveitis following perforating ocular trauma or intraocular surgery in one eye. Trauma or surgery exposes uveal tissue to the immune system, triggering an autoimmune reaction against melanin proteins.
The injured or operated eye is called the exciting eye, and the contralateral eye is called the sympathizing eye. This concept has been known since the time of Hippocrates, with the earliest literature dating back to the 1500s. The modern concept was established by Mackenzie in the 1840s. 8)
After surgery involving perforation of the eyeball wall
0.01–0.05%4)
More common after multiple surgeries
After vitreoretinal surgery
0.01–0.06%7)
UK/Ireland prospective survey
There is no racial difference, and it occurs in various age groups. A prospective surveillance in the UK and Ireland by Kilmartin et al. (2000) confirmed that it is an extremely rare disease with an annual incidence of 0.03 per million population.7)
The interval from injury to onset is most commonly 2 weeks to several months. A retrospective study of 32 cases by Chan et al. (1995) reported a range of 5 days to 66 years, indicating the possibility of onset after a long period.5) In recent years, due to improvements in surgical instruments and techniques resulting in smaller incisions, postoperative cases have been decreasing.9)
QWhat types of surgery can cause it?
A
Virtually any intraocular surgery can be a cause. It is particularly common after multiple surgeries such as retinal detachment repair and vitrectomy. Cyclodestructive procedures are reported to have a slightly higher incidence. With recent small-incision vitrectomy (25–27G), the incidence is extremely low. 9)
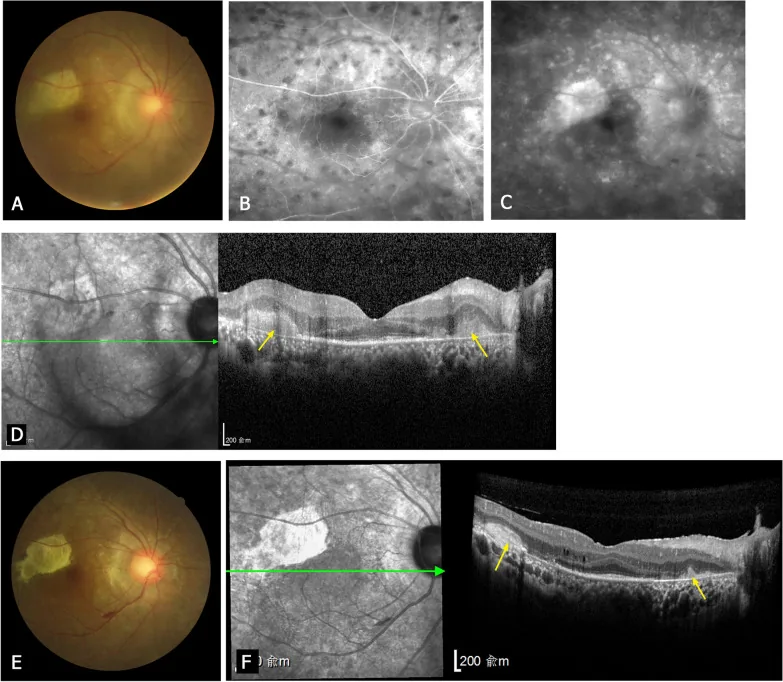
Zhuang H, et al. Clinical classification, visual outcomes, and optical coherence tomographic features of 48 patients with posterior sympathetic ophthalmia. Orphanet J Rare Dis. 2022. Figure 3. PMCID: PMC8895912. License: CC BY.
Multimodal imaging of posterior segment findings in sympathetic ophthalmia. The fundus shows yellowish-white chorioretinal inflammatory lesions and vitreous opacities, and inflammatory lesions are also confirmed on fluorescein angiography and OCT. This corresponds to the posterior segment findings of sympathetic ophthalmia discussed in the section “Main Symptoms and Clinical Findings.”
In the early stage, headache, hearing loss, tinnitus, and bilateral visual loss and metamorphopsia appear. Decreased near vision is often an early symptom.
Blurred vision and visual loss: Occur bilaterally. Onset may be insidious or acute.
Eye pain and redness: Pain accompanied by ciliary injection.
Extraocular symptoms include meningeal irritation (headache, nausea, nuchal rigidity), inner ear symptoms (sensorineural hearing loss, tinnitus, vertigo), and skin symptoms (vitiligo, alopecia, poliosis). These may present the same extraocular findings as Vogt-Koyanagi-Harada disease.
Dalen-Fuchs nodules: Yellowish-white nodules between the retinal pigment epithelium and Bruch’s membrane (a pathological feature shared with Vogt-Koyanagi-Harada disease).
Recovery and Chronic Phase Findings
Sunset glow fundus: Fundus changes due to depigmentation of the choroidal melanin.
Multiple peripheral patchy atrophic lesions: Occur frequently during the convalescent stage.
Secondary cataract and secondary glaucoma: Caused by chronic inflammation and steroid use.
Intraocular pressure may be elevated due to inflammatory glaucoma or decreased due to ciliary body dysfunction. Large cohort studies report that visual acuity of 20/200 or worse occurs in approximately 30–40% of patients at the final visit. 4)
QWhat is the difference from Harada disease?
A
The pathology is the same as Harada disease, but the triggering event differs. Harada disease has no preceding ocular trauma and has a higher rate of systemic findings (cerebrospinal fluid pleocytosis, skin symptoms). In Harada disease, posterior findings precede anterior inflammation. In sympathetic ophthalmia, trauma or surgical scars in the exciting eye are key to diagnosis.
The pathology of sympathetic ophthalmia is considered identical to that of Vogt-Koyanagi-Harada (VKH) disease. Ocular trauma or surgery exposing the uvea triggers recognition of uveal tissue by the systemic immune system, leading to a T-cell-mediated autoimmune disease against self-melanin proteins.
Main risk factors:
Perforating ocular trauma: Trauma involving prolapse or exposure of uveal tissue is most typical. In a study by Galor et al. (2009), trauma was the most common cause of the exciting eye. 4)
Intraocular surgery (involving perforation of the eyeball wall):
Vitrectomy and retinal detachment surgery (higher risk with multiple procedures)
HLA-related genetic predisposition: Association with HLA-DRB1*04, HLA-DR4, and HLA-DQ4 has been reported. 8)
Immune checkpoint inhibitor (ICI)-related sympathetic ophthalmia: Cases of recurrence after pembrolizumab administration have been reported. Particular caution is needed in patients with a history of ocular trauma and malignant tumors. 2)
Diagnosis is made comprehensively based on a history of penetrating ocular trauma or intraocular surgery, ocular findings, imaging findings, and extraocular symptoms. Even if the trauma history is unclear, scar traces on the eyeball during examination can provide diagnostic clues.
OCT (Optical Coherence Tomography): Evaluates choroidal thickening, serous retinal detachment, and optic disc edema. EDI-OCT shows a marked increase in choroidal thickness (>400 μm) in the acute phase. 8)
FA (Fluorescein Angiography): Multiple pinpoint leaks in the posterior pole (leopard-skin pattern), subretinal fluid accumulation.
ICGA (Indocyanine Green Angiography): Detection of choroidal granulomas as hypofluorescent spots.
OCT-A (Optical Coherence Tomography Angiography): Evaluates blood flow abnormalities in the choriocapillaris. Expected to be useful for disease monitoring. 8)
Exclusion of infectious uveitis (tuberculosis, syphilis) is essential before starting immunosuppressive therapy. 3)
QWill the disease not develop if the injured eye is removed?
A
There is a classic report that removal of the exciting eye within two weeks of injury prevents chronic uveitis in the sympathizing eye and leads to a good prognosis. 5) However, with advances in modern immunosuppressive therapy, cases that do not require removal are increasing. 8) Removal after onset is not thought to improve inflammation in the sympathizing eye. The decision to remove should be made on a case-by-case basis.
Sympathetic ophthalmia shares the same pathology as Harada disease, and treatment follows the VKH protocol. 3) Once infection is ruled out, immunomodulatory therapy should be started promptly.
60 mg/day → reduce by 10 mg every 4 days → 40 mg/4 weeks → 20 mg/4 weeks → 10 mg/4 weeks → 5 mg/4 weeks
Discontinue over 6 months or more
High-dose steroids rapidly resolve serous retinal detachment, and a study by Galor et al. (2009) reported that final visual acuity of 20/40 or better was achieved in approximately 50% of cases. 4) Oral steroids should be tapered slowly and discontinued over at least 6 months even without recurrence.
In cases with repeated recurrence during steroid tapering, immunosuppressive drugs are used in combination.
Cyclosporine (Neoral): 3–5 mg/kg/day in two divided doses. Target trough level 50–200 ng/mL. Regular monitoring of renal and liver function is required.
Methotrexate (MTX): 7.5–25 mg/week. In the FAST trial VKH subanalysis, MTX showed equivalent or superior efficacy to MMF in improving visual acuity and SRD in the acute phase. 10)
Adalimumab: 40 mg every 2 weeks subcutaneously. Approved for non-infectious uveitis.
Infliximab: 5 mg/kg intravenously (sympathetic ophthalmia is off-label).
Before initiating TNF inhibitors, screening for tuberculosis and hepatitis B is mandatory, following the uveitis treatment guidelines and TNF inhibitor usage guidelines. 3)
There is debate regarding enucleation of the exciting eye. Classic reports suggest that enucleation within 2 weeks of onset may help prevent chronicity in the sympathizing eye. 5) However, with advances in modern immunosuppressive therapy, many cases do not require enucleation. 8, 9)Conditions to consider enucleation:
The exciting eye has very poor vision with no hope of recovery
And the sympathizing eye has severe, uncontrollable uveitis
Recent meta-analyses have not provided consistent evidence for the effect of enucleation after onset, and a neutral judgment is required. 8, 9)
QShould the exciting eye be enucleated?
A
With modern treatment, enucleation is not always necessary. The exciting eye may retain some vision and can sometimes be preserved with appropriate steroid therapy. Enucleation is considered only under specific conditions: when the exciting eye has very poor vision with no hope of recovery and the sympathizing eye has severe inflammation. It is important to discuss with your doctor and make a careful decision.
The pathogenesis of sympathetic ophthalmia overlaps with that of Vogt-Koyanagi-Harada disease in many aspects. The eye is an immune-privileged organ, and antigens within the uvea are normally not easily recognized by the systemic immune system. 1) Perforating trauma or intraocular surgery disrupts this immune privilege, exposing intraocular antigens such as melanin proteins to the immune system.
Immune response:
CD4+ Th1/Th17 cells predominantly infiltrate and produce IFN-γ and IL-17.
CD8+ cytotoxic T cells subsequently infiltrate and target melanocytes (tyrosinase, TRP-1, TRP-2, gp100). 8)
Disruption of the blood-ocular barrier and blood-retinal barrier induces an autoimmune response against intraocular antigens. 1)
HLA-DR4 and HLA-DRB1*04-related genetic predisposition increases susceptibility. 8)
Histopathological features:
Dalen-Fuchs nodules: Clusters of pigment-containing epithelioid cells located between the retinal pigment epithelium and Bruch’s membrane. They form granulomas with lymphocytes and multinucleated giant cells.
Preservation of the choriocapillaris: In Vogt-Koyanagi-Harada disease, inflammation spreads to the choriocapillaris, but in sympathetic ophthalmia, it is usually preserved.
No retinal involvement: The inflammatory process typically does not extend to the retina.
In the anterior segment, the iris thickens with nodular infiltration.
When immune checkpoint inhibitors (ICIs) are used, it has been suggested that a history of exposure to intraocular antigens may trigger unintended reactivation of T cells. 2)
7. Latest Research and Future Perspectives (Research-stage Reports)
In the VKH subanalysis of the FAST Uveitis Trial (double-blind RCT) by Acharya et al. (2024), MTX showed equal or greater efficacy compared to MMF in improving acute chorioretinal findings (serous retinal detachment, choroidal thickening). 10) Since sympathetic ophthalmia shares the same pathophysiology as VKH, the findings of this trial may be applicable to the selection of immunosuppressive drugs for sympathetic ophthalmia.
OCT-A, which enables quantitative assessment of choriocapillaris blood flow, is being studied as a biomarker to detect potential disease activity after clinical inflammation has subsided. 8) Longitudinal monitoring of choroidal thickness using EDI-OCT is also expected as a predictor of recurrence.
Changes in Incidence in the Era of Small Incision Surgery
With the widespread use of 27G and 25G vitrectomy, the postoperative incidence has significantly decreased compared to conventional open incision surgery. In a review by Patel et al. (2022), improvements in modern surgical techniques are considered the main reason for the reduced incidence. 9) On the other hand, post-traumatic incidence remains difficult to reduce without trauma prevention, and caution is still required.
Experience with biologics such as adalimumab and infliximab has been accumulating in refractory cases of VKH and sympathetic ophthalmia. 6) However, evidence is mainly from case reports and small series, and drug selection should be individualized based on inflammation severity, recurrence, and systemic comorbidities.
New Challenges of ICI-Associated Sympathetic Ophthalmia
Recurrence of sympathetic ophthalmia after pembrolizumab administration has been reported, posing a new clinical challenge in the era of cancer immunotherapy. 2) Enhanced ophthalmic monitoring is recommended when initiating ICI in patients with a history of ocular trauma.
Agarwal M, Radosavljevic A, Tyagi M, Pichi F, Al Dhanhani AA, Agarwal A, Cunningham ET Jr. Sympathetic Ophthalmia - An Overview. Ocul Immunol Inflamm. 2023;31(4):793-809. doi:10.1080/09273948.2022.2058554.
Lee J, Shin JY, Lee JS, Lee SC, Hong MH, Lee CS. Recurrent Sympathetic Ophthalmia with Annular Choroidal Detachment after Pembrolizumab Treatment: A Case Report. Ocul Immunol Inflamm. 2020;28(6):864-867. doi:10.1080/09273948.2019.1604975.
Anat Galor, Janet L. Davis, Harry W. Flynn, William J. Feuer, Sander R. Dubovy, Vikram Setlur, Muge R. Kesen, Debra A. Goldstein, et al. Sympathetic Ophthalmia: Incidence of Ocular Complications and Vision Loss in the Sympathizing Eye. American Journal of Ophthalmology. 2009;148(5):704-710.e2. doi:10.1016/j.ajo.2009.05.033.
Chan CC, Roberge RG, Whitcup SM, Nussenblatt RB. 32 cases of sympathetic ophthalmia. A retrospective study at the National Eye Institute, Bethesda, Md., from 1982 to 1992. Archives of ophthalmology (Chicago, Ill. : 1960). 1995;113(5):597-600. doi:10.1001/archopht.1995.01100050065032. PMID:7748129.
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clin Ophthalmol. 2021;15:4201-4218. doi:10.2147/OPTH.S289688. PMID:34707340. PMCID:PMC8542579. https://pmc.ncbi.nlm.nih.gov/articles/PMC8542579/
Kilmartin DJ, Dick AD, Forrester JV.. Prospective surveillance of sympathetic ophthalmia in the UK and Republic of Ireland. Br J Ophthalmol. 2000;84(3):259-263. doi:10.1136/bjo.84.3.259. PMID:10684834; PMCID:PMC1723405.
Chu XK, Chan CC.. Sympathetic ophthalmia: to the twenty-first century and beyond. J Ophthalmic Inflamm Infect. 2013;3(1):49. doi:10.1186/1869-5760-3-49. PMID:23724856; PMCID:PMC3679835.
Patel SS, Hariprasad SM. Sympathetic ophthalmia: a mini-review. Semin Ophthalmol. 2022;37(3):313-321.
Nisha R. Acharya, Sivakumar R. Rathinam, Radhika Thundikandy, Anuradha Kanakath, S. Bala Murugan, R. Vedhanayaki, John A. Gonzales, Lyndell L. Lim, et al. Outcomes in Patients With Vogt–Koyanagi–Harada Disease From the First-Line Antimetabolites for Steroid-Sparing Treatment Uveitis Trial. American Journal of Ophthalmology. 2024;267:100-111. doi:10.1016/j.ajo.2024.06.004.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.