Tubercular uveitis (TB-uveitis) is a condition in which Mycobacterium tuberculosis (Mtb) reaches the eye hematogenously and causes inflammation mainly in the retina and choroid. Direct detection of Mtb from within the eye is almost impossible; clinically, diagnosis emphasizes immunological tests and response to anti-tuberculosis therapy. The presence of uveitis that responds dramatically to anti-tuberculosis drugs alone is a more important clinical finding than bacterial proof.
The proportion of tubercular uveitis among infectious uveitis is reported to be about 1.4% 3). In high-burden Asian countries such as India and Indonesia, it accounts for 22.9–48.0% of infectious uveitis1). The prevalence among all uveitis patients is reported to be 0.2–10.5% in tertiary care centers worldwide 2). In Japan, the tuberculosis incidence rate is higher than in Western developed countries, especially in large cities. With the increase in travelers from high-burden countries such as China, India, and Southeast Asia, this disease should always be considered in the differential diagnosis of uveitis.
Visual impairment from tubercular uveitis can be severe. It has been reported that about one-third of patients have best-corrected visual acuity less than 3/60 1). Uveitic macular edema and secondary glaucoma occur in about 30% of patients 1). Active pulmonary tuberculosis rarely coexists with uveitis, and many cases have limited or no lung findings.
QHow common is tubercular uveitis in Japan?
A
It is said to account for about 1.4% of all infectious uveitis3). Since ocular tuberculosis can develop even without active lung lesions, if there is immunological evidence such as a positive IGRA, ocular tuberculosis should be suspected regardless of the presence of lung lesions.
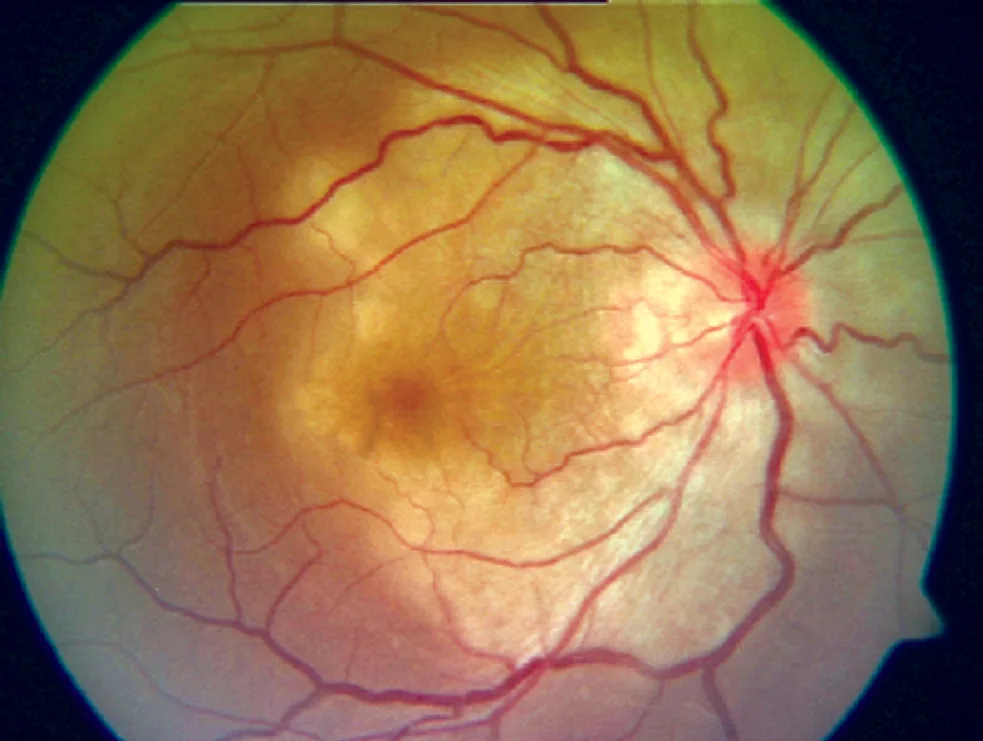
Fundus photograph of ocular tuberculosis showing multiple nodular lesions from the optic disc to the posterior pole. This corresponds to “choroidal miliary tuberculosis” discussed in section “2. Main Symptoms and Clinical Findings”.
Miliary choroidal tuberculosis: Yellow-white small exudative spots scattered under the retina. Nodules of 1/2 to 1/6 disc diameter present as multifocal choroiditis. Usually bilateral, often occurs when cell-mediated immunity is reduced, such as in AIDS. Tuberculin reaction is often negative.
Choroidal tuberculoma: A yellow-white mass larger than one disc diameter formed near the posterior pole. It is a granuloma composed of epithelioid cells and Langhans giant cells, with caseous necrosis. A very rare lesion.
Retinal vasculitis / choroiditis
Occlusive retinal phlebitis: One of the three major lesions. Presents with recurrent vitreous hemorrhage (Eales disease-like) and rapid expansion of non-perfusion areas. Retinal hemorrhage and venous sheathing are observed.
Serpiginous choroiditis: Typically spares the fovea and presents with serpiginous lesions accompanied by vitreous inflammation. In SUN 2021, ATT is recommended based on a single positive IGRA item 2).
Cystoid macular edema, papillitis, optic neuritis: Occur as complications of posterior inflammation.
In anterior uveitis, granulomatous inflammation is characteristic. Mutton fat keratic precipitates, iris Koeppe nodules and Busacca nodules, and broad-based posterior synechiae are observed 1). In the intermediate part, snowball vitreous opacities and exudates on the pars plana (snowbank) may occur.
Mycobacterium tuberculosis reaches the eye (mainly the choroid) via hematogenous dissemination from the primary lung infection, causing inflammation. The choroid has high blood flow and oxygen tension, making it a favorable environment for bacterial colonization. The following three mechanisms have been proposed 1).
Direct infection by M. tuberculosis: Bacteria that reach ocular tissues via the bloodstream directly cause inflammation. This corresponds to miliary tuberculosis and tuberculoma.
Immune response (in the absence of bacteria): An excessive immune response to extraocular tuberculous antigens triggers intraocular inflammation. It can occur even without viable bacteria in the eye. Retinal vasculitis is thought to develop through this mechanism.
Autoimmune response: Cross-reactivity (antigen mimicry) between tuberculous antigens and retinal antigens may induce anti-retinal autoimmunity 1). In active and latent TB-uveitis, the serum positivity rate for anti-retinal antibodies (ARA) is higher than in healthy individuals.
Risk factors:
Immunosuppression: AIDS, use of immunosuppressive drugs, elderly
Residence or travel history in high tuberculosis prevalence areas: Travel history to China, India, Southeast Asia
Latent tuberculosis + biologic therapy: TNF-α inhibitors carry a risk of reactivating latent tuberculosis1)
History of incarceration or institutionalization: High risk of tuberculosis exposure in closed environments
According to the uveitis clinical practice guidelines, tuberculous uveitis is diagnosed when the following four elements are met3).
Typical fundus findings
Evidence or history of systemic tuberculosis infection
Positive tuberculosis immune response (tuberculin skin test / IGRA)
Response to anti-tuberculosis drug therapy (therapeutic trial)
Since it is rare to detect tubercle bacilli from within the eye, treatment is based on a presumptive diagnosis in most cases. If inflammation subsides or worsens (some reaction to the drug) within about one week after starting oral isoniazid, it is considered effective. If there is no effect after one month, it is deemed ineffective and discontinued.
Affected by BCG vaccination; negative in miliary tuberculosis and AIDS cases
QFT (QuantiFERON® TB Gold Plus)
Measures interferon-γ production by sensitized CD4/CD8-positive T lymphocytes. Not affected by BCG.
Also positive in latent infection
T-SPOT®
ELISPOT method. Useful for detecting prior tuberculosis infection.
Has similar limitations as interferon-gamma release assays
QuantiFERON® TB Gold Plus (QFT-plus) measures interferon-γ secreted by cell-mediated immune responses of both CD4-positive and CD8-positive T lymphocytes sensitized to Mycobacterium tuberculosis, allowing assessment without the influence of BCG vaccination. Combining the tuberculin skin test and IGRA improves the sensitivity of ocular tuberculosis diagnosis 9).
During immunosuppressive therapy, the tuberculin skin test and IGRA may yield false-negative results. If possible, testing should be performed before starting immunosuppression. In non-endemic countries, the proportion of unexplained uveitis is significantly higher in IGRA-positive patients than in IGRA-negative patients (59% vs 39%) 1).
PCR testing using intraocular fluid (aqueous humor or vitreous fluid) is performed. Real-time PCR methods (e.g., targeting the IS6110 sequence) are useful, but the PCR positivity rate in systematic reviews is only 55% 1). In highly endemic countries such as India, the positivity rate can reach up to 70% when using MPB64 primers 1). Intraocular fluid PCR is considered an adjunctive test.
The Collaborative Ocular Tuberculosis Study (COTS) group has proposed an algorithm that stratifies by phenotype (serpiginous choroiditis/tuberculoma/multifocal choroiditis/vascular occlusive retinitis) and endemic/non-endemic region 2). For serpiginous choroiditis and tuberculoma, initiation of ATT is recommended if either IGRA or TST is positive. This algorithm sets different thresholds for endemic and non-endemic countries, making it clinically applicable.
Sarcoidosis: The most important differential diagnosis clinically. Both conditions present with granulomatous inflammation, and the tuberculin skin test and IGRA are important for differentiation. Misdiagnosing as sarcoidosis and administering long-term steroids may trigger fatal infections.
Behçet’s disease: Requires differentiation when retinal vasculitis is present.
Vogt-Koyanagi-Harada (VKH) disease: Requires differentiation when bilateral serous retinal detachment or choroidal thickening is present.
Toxoplasmosis: May present with similar clinical features when retinitis or vitritis is present 9).
QCan ocular tuberculosis be confirmed even if TST or QFT is positive?
A
Positive IGRA or TST indicates an immune response to Mycobacterium tuberculosis, but can also occur in latent infection, so it does not confirm ocular tuberculosis. Diagnosis is made by combining typical ocular findings, exclusion of other diseases, and treatment response1)2).
QWhat should be checked before starting biologic agents?
A
Before administration of biologic agents such as TNF-α inhibitors, screening for latent tuberculosis with chest X-ray, TST, or IGRA is mandatory1). If latent tuberculosis is positive, prophylactic chemotherapy should be given for at least one month before starting biologic agents. Even if screening is negative, attention must be paid to reactivation of tuberculosis during treatment.
The mainstay of treatment for tuberculous uveitis is multidrug antituberculosis therapy (ATT)1). ATT has been reported to reduce the recurrence rate by approximately 75%2).
An example of a prescription by brand name: Isocotin tablets (INH 100 mg) 3 tablets 3 times daily, Rifadin (RFP 150 mg) 3 capsules once daily before breakfast, Esambutol tablets (EB 250 mg) 3 tablets once daily in the morning. For prevention of peripheral neuritis, Vitamedin combination capsules B50 (VB6) are used concomitantly. Since 2008, Fabutin (rifabutin) has also been approved, adding to the options for combination therapy 3).
The standard minimum duration of treatment is 6 months, and may be extended to 9–12 months in severe cases or poor responders 1). As a therapeutic trial, if inflammation subsides or worsens about one week after starting ATT, it is considered effective. If there is no effect after one month, it is considered ineffective and discontinued. If effective, drugs such as rifampicin are added.
COTS criteria for initiating ATT 2):
Serpiginous choroiditis / tuberculoma: ATT can be initiated with only one positive IGRA/TST item.
Other clinical types: Comprehensive judgment based on clinical presentation, immunological tests, and imaging findings.
Combined use with ATT is effective for controlling posterior inflammation. Usually, it is started at the same time as or immediately after starting ATT, and tapered over 4–6 weeks. For serpiginous choroiditis, the COTS guidelines recommend concomitant use of oral corticosteroids at or shortly after initiation 2). Sub-Tenon injection of triamcinolone acetonide (Kenacort-A®) is also an option, but it is preferable to administer it after determining the effectiveness of antitubercular drugs. In prolonged or recurrent cases, addition of immunosuppressive agents is considered 2).
QHow long should anti-tuberculosis drugs be taken?
A
Standard treatment is a total of 6 months: 2 months of intensive phase plus 4 months of maintenance phase. For severe cases or poor responders, it may be extended to 9–12 months 1). Regular visual function tests (especially monitoring for ethambutol optic neurotoxicity) are essential during treatment.
Mycobacterium tuberculosis spreads hematogenously from the primary lung infection to ocular tissues. The choroid, with its high blood flow and oxygen tension, provides a favorable environment for bacterial colonization. Histologically, granulomas composed of epithelioid cells and Langhans giant cells are formed. Granulomatous inflammation with caseous necrosis is the histological picture of choroidal tuberculoma. In miliary tuberculosis, when there is a massive influx of tubercle bacilli due to cellular immunodeficiency such as in AIDS, choroidal nodules of 1/2 to 1/6 disc diameter are scattered.
In tuberculosis infection, the retinal pigment epithelium (RPE) induces an innate immune response dominated by IFN-α/β. Even in the absence of live bacteria in the eye, an excessive immune response to tuberculous antigens can cause intraocular inflammation. Retinal vasculitis is thought to result from an immune reaction to constituent proteins of M. tuberculosis.
A review by Putera et al. (2024) suggested the possibility of stratifying highly active TB-uveitis based on regulatory T cell (Treg) dysfunction and type I interferon-stimulated gene (ISG) expression. The C1q+ type I IFN signature is attracting attention as a diagnostic aid marker 1).
Involvement of autoimmune reactions via molecular mimicry between tuberculous antigens and retinal antigens has been proposed. Activation of anti-retinal autoimmune responses (IRBP T cell response) may sustain and enhance intraocular inflammation 1). It has been reported that serum anti-retinal antibody (ARA) positivity rates are higher in patients with active and latent TB-uveitis than in healthy controls.
In addition to conventional ATT, approaches that modulate the host immune response are being studied. Against the backdrop of increasing drug-resistant tuberculosis, several HDT candidate drugs are being investigated in the field of pulmonary tuberculosis, and their application to tuberculous uveitis is also attracting attention 1). Stratification of disease activity by ISG signature may improve the accuracy of future ATT indication decisions.
Putera et al. (2024) reported that the expression pattern of ISGs (type I interferon-stimulated genes) may stratify highly active TB-uveitis1). The combination of C1q and type I IFN signature is considered promising as a diagnostic aid marker, and may lead to improved accuracy of ATT indication decisions in the future.
The COTS group is continuously reviewing ATT management criteria based on multicenter data 2). In particular, guidelines for the use of immunosuppressive drugs other than steroids for persistent and recurrent cases requiring immunosuppressive treatment are being developed.
Diverse Clinical Presentations of Posterior Ocular Tuberculosis
Faneli et al. (2026) reported six cases of posterior ocular tuberculosis 5). The cases included diverse clinical types: choroidal granuloma, multifocal choroiditis, serpiginous choroiditis, and occlusive retinal vasculitis. In all cases, inflammation subsided with RIPE therapy plus steroids. Four cases had a history of incarceration, and pulmonary findings were observed in only three cases. Anti-VEGF therapy was added in one case complicated by choroidal neovascularization.
Hou et al. (2025) reported a case of a 36-year-old man with presumed ocular tuberculosis closely resembling autoimmune retinopathy 6). After worsening with steroid administration, visual acuity and macular structure markedly improved with ATT monotherapy for one month.
Babalola et al. (2025) reported an atypical case of ocular tuberculosis in a 15-year-old boy with bilateral optic atrophy and epiretinal membrane7). A family history of tuberculosis and the presence of choroidal nodules provided clues for the presumptive diagnosis.
Improvements in real-time PCR technology for intraocular fluids have increased the positivity rate when using MPB64 primers. The establishment of non-invasive diagnostic algorithms combining multimodal imaging and IGRA is also progressing. Bruzzone et al. (2024) reported a case in which QFT-plus became positive after two negative tuberculin reactions, leading to a diagnosis of tuberculous multifocal choroiditis, highlighting the importance of performing IGRA before initiating immunosuppression 8).
Putera I, Schrijver B, ten Berge JCEM, et al. The immune response in tubercular uveitis and its implications for treatment. Prog Retin Eye Res. 2024;101:101289.
Agrawal R, Testi I, Mahajan S, et al. Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis—Report 1. Ophthalmology. 2021;128(2):266-276.
Jabs DA, Belfort R Jr, Bodaghi B, et al. Classification Criteria for Tubercular Uveitis. Am J Ophthalmol. 2021;228:142-151. doi:10.1016/j.ajo.2021.03.040.
Faneli AC, Souza GM, Neto PFS, Finamor LP, Oliveira RDC, Muccioli C. Chasing shadows: case series of six posterior segment manifestations of ocular tuberculosis. AME case reports. 2026;10:50. doi:10.21037/acr-2025-91. PMID:41676170; PMCID:PMC12885848.
Hou SM, Liu Q, Zhang XH, Peng XY, Zeng HY. Presumed Ocular tuberculosis masquerading as autoimmune retinopathy. American journal of ophthalmology case reports. 2025;38:102296. doi:10.1016/j.ajoc.2025.102296. PMID:40144310; PMCID:PMC11938075.
Babalola YO. Bilateral Optic Atrophy and Epiretinal Membranes: An Atypical Presentation of Ocular Tuberculosis. Nigerian medical journal : journal of the Nigeria Medical Association. 2025;66(1):389-393. doi:10.71480/nmj.v66i1.711. PMID:40309520; PMCID:PMC12038614.
Bruzzone F, Plebani M, Koryllou A, Perreau M, Guex-Crosier Y. The Importance of QuantiFERON Gold Plus Test for the Diagnosis of Presumed Ocular Tuberculosis. Klinische Monatsblatter fur Augenheilkunde. 2024;241(4):432-434. doi:10.1055/a-2244-6657. PMID:38653273; PMCID:PMC11038820.
Bromeo AJ, Lerit SJ, Arcinue C. Ocular tuberculosis masquerading as atypical ocular toxoplasmosis. GMS ophthalmology cases. 2023;13:Doc19. doi:10.3205/oc000227. PMID:37850223; PMCID:PMC10577653.
Gupta A, Bansal R, Gupta V, et al. Ocular signs predictive of tubercular uveitis. Am J Ophthalmol. 2020;205:72-80.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}