Uveitic macular edema (UME) is a condition in which fluid accumulates in the macula due to uveitis. Uveitis accounts for up to 15% of all causes of blindness in developed countries 2). The most frequent complication is UME, which causes visual impairment in about one-third of uveitis patients 2).
Approximately 8.3% of patients with non-infectious uveitis develop UME 1). Cystoid macular edema (CME) is observed in 10–70% of uveitis patients, with reported rates of 5.1% in anterior uveitis and 40.7% in intermediate uveitis5). Sarcoidosis, intermediate uveitis, and Behçet’s disease are types particularly associated with UME.
Cystoid macular edema refers to a condition in which tissue fluid accumulates in the intercellular spaces of retinal neurons in the macula, leading to cystoid edema. In uveitis, cystoid macular edema occurs through disruption of the blood-retinal barrier (BRB), characterized by cystoid changes in the outer plexiform layer and inner nuclear layer. The cyst walls are formed by Müller cells and axon fibers. Postoperative cystoid macular edema after cataract or vitreous surgery is called Irvine-Gass syndrome and is distinguished from uveitic macular edema 7).
Edema may persist even after inflammation is controlled, so intervention for both inflammation and edema is necessary 2). If infectious uveitis is the underlying cause, treatment of the causative pathogen should be prioritized. Uveitis clinical practice guidelines classify cystoid macular edema as a serious complication of active uveitis and recommend early therapeutic intervention 7).
QCan macular edema persist even after uveitis inflammation subsides?
A
Macular edema may persist even after inflammation subsides. Therefore, additional treatment targeting the edema itself may be necessary. For details, see the section on “Standard Treatment.”
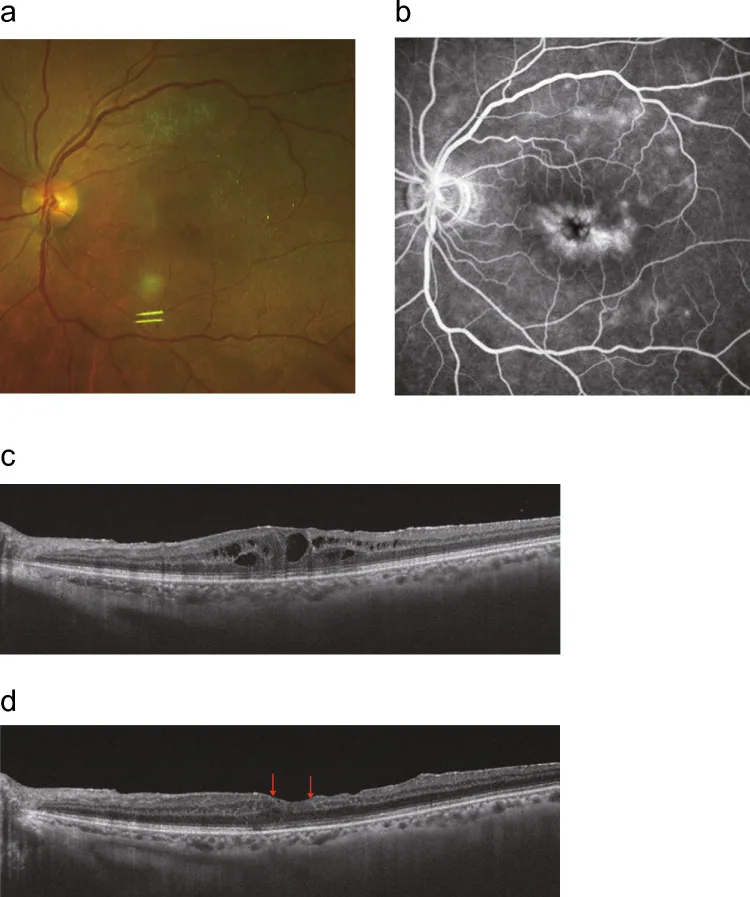
Takeda A, et al. Recent advances in the diagnosis and treatment of refractory ocular inflammatory diseases: focus on uveitic macular edema, acute retinal necrosis, and vitreoretinal lymphoma. Jpn J Ophthalmol. 2026. Figure 1. PMCID: PMC12948802. License: CC BY.
Multi-panel image showing uveitic macular edema on fundus photography, fluorescein angiography, and OCT. Macular leakage on FA and cystoid spaces on OCT illustrate the main clinical and diagnostic findings.
The main subjective symptom of UME is decreased central vision.
Decreased vision: Central vision is impaired due to fluid accumulation in the macula. It often progresses slowly.
Blurred vision: The entire visual field appears hazy due to retinal structural changes from macular edema.
Metamorphopsia (distortion): Straight lines appear bent due to macular deformation.
Central scotoma: In severe cases, a dark area is perceived in the center of the visual field.
In uveitis, vision loss can also occur due to cell infiltration in the anterior chamber or vitreous, corneal opacity, and complicated cataract. If vision loss is greater than expected from these findings, cystoid macular edema should be suspected. Vision loss is often moderate to severe, and detailed evaluation of the macula is essential.
OCT: Non-invasively visualizes cross-sections of the macula. It can detect retinal thickening, cyst formation, and serous retinal detachment. UME is often diagnosed when central subfield thickness (CST) is 300 μm or more 2). It is also essential for evaluating treatment response and tracking changes in thickness over time.
Fluorescein angiography (FA): Useful for detecting increased permeability of retinal vessels and neovascularization. In cystoid macular edema, it shows a petaloid pattern of fluorescein leakage and pooling centered on the fovea in the late phase.
Indocyanine green angiography (ICG): Used to evaluate choroidal circulation. It is useful for assessing choroidal lesions in sarcoidosis and Vogt-Koyanagi-Harada disease.
QHow often should I undergo OCT during regular check-ups?
A
During follow-up of UME, OCT evaluation of the macula is essential. The attending physician determines the frequency based on inflammatory activity and treatment stage, but during treatment, examinations every 1 to 3 months are common.
Treatment of UME is complex, and the optimal method varies for each patient 1). For infectious uveitis, treatment of the cause is prioritized, and for non-infectious UME, treatment centered on steroids is performed. The uveitis treatment guidelines recommend sub-Tenon steroid injection for persistent cystoid macular edema, and vitrectomy as an option for steroid-resistant refractory cases 7).
Steroid eye drops: Used for mild UME associated with anterior uveitis. Betamethasone or dexamethasone eye drops are administered 3 to 6 times daily, adjusted according to the degree of inflammation. The effect on posterior segment lesions is limited 1).
Mydriatic agents: Tropicamide/phenylephrine eye drops are used concomitantly to prevent posterior synechiae.
NSAID eye drops: Useful for macular edema in pseudophakic eyes, but their efficacy for UME has not been clearly demonstrated 1).
This is the first local procedure performed to control chronic posterior segment inflammation, and is well indicated for macular edema, retinal vasculitis, and vitreous opacity.
Posterior sub-Tenon injection of triamcinolone acetonide: Effective for persistent uveitis involving the posterior segment, such as cystoid macular edema. Used when inflammatory changes in the posterior pole are severe 7).
Procedure: Puncture the conjunctival fornix in the inferotemporal quadrant and inject 20 mg/0.5 mL of triamcinolone acetonide into the posterior sub-Tenon space using a 24-25G blunt or sharp needle. Injection from the superior approach carries a risk of ptosis, so inferotemporal puncture is recommended. The drug remains in the sub-Tenon space for about 3 months after injection, with peak effect around 1 month.
For cystoid macular edema associated with sarcoidosis and Behçet’s disease, posterior sub-Tenon injection of Kenacort-A 40 mg/mL (triamcinolone acetonide) 0.5 mL is performed (off-label use).
Caution is needed for increased intraocular pressure (occurring in 15–20% of patients), and posterior injection may reduce the risk of elevated IOP1).
QIs it safe to repeat sub-Tenon injections?
A
Uveitic macular edema may recur, so multiple injections may be necessary. When repeated, it is recommended to space them at least 2 months apart. However, intraocular pressure should be measured each time, and the presence of elevated IOP or cataracts should be checked before administration. If elevated IOP becomes a problem, consider switching to other treatments such as intravitreal injection.
Intravitreal triamcinolone acetonide injection: A dose of 4 mg improves visual acuity in about 50% of patients 1). Cataract progression is related to the number of injections, occurring almost certainly after 4-5 injections. Increased intraocular pressure is observed in 20-45% of patients, but can be managed with eye drops in most cases 1).
Dexamethasone intravitreal implant (Ozurdex): This is a polymer implant that releases 0.7 mg of dexamethasone slowly. In the HURON trial (Phase III), 42% of the Ozurdex 0.7 mg group achieved a vitreous haze score of zero at 26 weeks (placebo 12%, p<0.001) 9). At 8 weeks, significant reduction in central foveal thickness and improvement in vitreous haze were confirmed 9).
In a systematic review and meta-analysis by Fan et al. (2023), after a single DEX implant, BCVA improved by -0.15 logMAR at 1 month, -0.22 logMAR at 3 months, and -0.24 logMAR at 6 months 3). Central macular thickness (CMT) decreased by -179.77 μm at 1 month, -179.13 μm at 3 months, and -140.25 μm at 6 months.
The incidence of increased intraocular pressure (IOP >21 mmHg) after DEX implant was 13.6%, and cataract formation was 5.4%, both manageable with eye drops 3).
In the POINT trial, periocular triamcinolone (PTA), intravitreal triamcinolone (ITA), and intravitreal DEX implant (IDI) were directly compared, with central foveal thickness reduction rates of 23%, 39%, and 46%, respectively 1). Intravitreal administration was superior to periocular administration, but the risk of increased intraocular pressure was also higher in the intravitreal groups.
Fluocinolone acetonide intravitreal implant: There are Iluvien (0.19 mg, lasting 36 months) and Retisert (0.59 mg, lasting 30 months). Long-term effects are obtained, but cataract surgery is required in 73.8% (Iluvien) to over 90% (Retisert) of phakic eyes, and glaucoma surgery was needed in 11.9% and 40%, respectively 1).
Triamcinolone acetonide suprachoroidal injection suspension (Xipere; SCS-TA) is the first drug approved for the treatment of UME and also the first approved formulation for suprachoroidal administration 2).
The suprachoroidal space (SCS) is a potential space located between the choroid and sclera, where drugs are selectively distributed to the posterior segment of the eye2). In animal studies, suprachoroidal administration resulted in 12-fold higher drug exposure to the posterior segment compared to intravitreal injection, while exposure to the anterior segment was reduced by 96%2). This property reduces the risk of cataract and elevated intraocular pressure.
In the PEACHTREE trial (Phase III), 46.9% of patients in the SCS-TA 4 mg group achieved a ≥15-letter improvement in BCVA at 24 weeks (sham group 15.6%, p<0.001)2). The mean reduction in central foveal thickness was 152.6 μm vs. 17.9 μm (p<0.001), with significant differences observed from week 4.
In the MAGNOLIA extension study, 50% of the SCS-TA group did not require rescue therapy for up to 9 months after the second injection2). The median time to rescue over 48 weeks was 257 days in the SCS-TA group and 55.5 days in the sham group.
SCS-TA has demonstrated efficacy regardless of concomitant systemic steroid use, anatomical location of uveitis, or disease duration2). The incidence of steroid-related intraocular pressure elevation in non-rescue patients was 10.8%, lower than the 21.7% in sham patients who received rescue therapy2).
Systemic corticosteroids: For bilateral or severe UME, start prednisolone at 0.5–1 mg/kg1). In Vogt-Koyanagi-Harada disease, steroid pulse therapy is used. Due to side effects, taper slowly over at least 6 months.
Immunosuppressants: Cyclosporine (Neoral 3–5 mg/kg/day) is added when steroid tapering is difficult. Monitoring of blood concentration (trough 50–200 ng/mL) and renal function is required. In Behçet’s disease, colchicine (0.5–1.5 mg/day) is the first-line treatment for suppressing inflammatory attacks.
Anti-TNF-α antibody (infliximab): Used for severe Behçet’s disease with recurrent attacks despite colchicine and cyclosporine. Usually administered intravenously at 5 mg/kg every 2 months.
Juvenile idiopathic arthritis (JIA)-associated uveitis: For UME associated with chronic iridocyclitis, stepwise treatment including methotrexate and biologic agents (adalimumab) is recommended 4). The IOIS report recommends methotrexate, azathioprine, and mycophenolate mofetil as first-line immunosuppressive agents for uveitis with UME 8). Adalimumab has been reported to achieve 97.7% CME control in JIA-associated uveitis with cystoid macular edema that is insufficiently responsive to methotrexate8).
VEGF inhibitors are used off-label for UME 1). They are first-line when choroidal neovascularization is present. They are a strong option for patients who are steroid-intolerant or steroid responders (prone to increased intraocular pressure). However, a clear dosing regimen for UME has not been established 1).
Vitrectomy is indicated for drug-resistant cases or steroid-resistant cystoid macular edema7). Vitrectomy combined with internal limiting membrane peeling or cystotomy is performed for persistent cystoid macular edema. Epiretinal membrane, macular hole, and vitreous hemorrhage are also surgical indications. Surgery is preferably performed when inflammation is quiescent, and perioperative steroid supplementation should be considered.
Because inflammation may worsen postoperatively, the risk-benefit ratio should be carefully assessed 1). After vitrectomy, the half-life of triamcinolone is shortened from 18.6 days to 3.2 days, so long-acting agents are recommended 1).
QWhat to do if intraocular pressure increases with steroid treatment?
A
First, try to manage with topical antihypertensive eye drops. In many cases, it can be controlled with drops. If drops and oral medications are insufficient, glaucoma surgery such as trabeculotomy is considered. Trabeculotomy is particularly effective for steroid-induced glaucoma.
Under normal conditions, the BRB is maintained by tight junctions of retinal vascular endothelial cells (inner) and retinal pigment epithelial cells (outer). In uveitis, inflammatory cytokines (TNF-α, IL-1β, IL-6) reduce the expression of tight junction proteins (ZO-1, occludin, claudin), increasing vascular permeability 5). VEGF also promotes vascular permeability and neovascularization2). Fluid accumulation occurs mainly in the inner nuclear layer and Henle fiber layer, observed as cystoid changes in the outer plexiform layer and inner granular layer.
Traction of the posterior vitreous membrane on the macula can also contribute to the development of UME. In epiretinal membrane and vitreomacular traction syndrome, vitreous traction can cause macular edema. Vitreous opacities and vitreous fibrosis associated with uveitis are prone to cause traction on the macula.
Triamcinolone acetonide binds to intracellular glucocorticoid receptors, promoting lipocortin production and suppressing the release of pro-inflammatory arachidonic acid 2). It inhibits immune cell infiltration and activation, reduces VEGF expression, thereby improving vascular permeability and reducing edema 2). If treatment is effective and edema resolves, visual improvement can be expected; however, in chronic uveitis, recurrence or persistence of edema may worsen visual prognosis.
In a study by Muya et al. using rabbits, SCS-TA showed lower glide force and less variability during injection compared to intravitreal triamcinolone formulations 2). This facilitates safe drug delivery to the suprachoroidal space. After suprachoroidal administration, high concentrations in the posterior segment were maintained for the first two months, reaching levels equivalent to intravitreal administration by the third month.
In a trial by Mackensen et al., the group receiving interferon beta (44 mg subcutaneously three times per week) showed a mean decrease in macular thickness of 206 μm, while the methotrexate group (20 mg subcutaneously once weekly) showed an increase of 47 μm (p<0.0001) 1). Interferon alfa-2a has been reported to have an efficacy rate of over 80% for refractory UME including Behçet’s disease.
In a prospective study of 15 patients by Taylor et al., intravitreal methotrexate 400 μg reduced mean macular thickness from 425 μm to 275 μm 1). One-third of patients experienced recurrence at a median of 4 months, but reinjection showed similar efficacy to the initial treatment.
Octreotide (100 μg subcutaneously three times daily, or long-acting 20 mg intramuscularly once monthly) has been reported to resolve edema in 7 of 9 eyes with chronic UME resistant to conventional therapy 6). Development of topical intraocular formulations is also ongoing.
Intravitreal sirolimus (mTOR inhibitor) did not achieve statistical significance for UME reduction in the SAVE-2 trial, but marked improvement was observed in some patients 1). Appropriate patient selection remains a future challenge.
Faricimab (anti-VEGF-A/Ang-2 dual inhibitor) targets both VEGF and angiopoietin-2, with expected synergistic effects on retinal vascular stabilization and permeability suppression. After approval for diabetic macular edema and wet AMD, its application to uveitic macular edema is under investigation. It is attracting attention as a new therapeutic development leveraging the multifaceted actions of anti-VEGF agents.
QIs suprachoroidal injection available in Japan?
A
SCS-TA (Xipere) was approved in the United States in 2021, but as of March 2026, it is not approved in Japan. For domestic availability, future regulatory trends need to be confirmed.
Teper SJ.. Update on the Management of Uveitic Macular Edema. J Clin Med. 2021;10(18):4133. doi:10.3390/jcm10184133. PMID:34575244; PMCID:PMC8470573.
Fung S, Syed YY. Suprachoroidal Space Triamcinolone Acetonide: A Review in Uveitic Macular Edema. Drugs. 2022;82(13):1403-1410. doi:10.1007/s40265-022-01763-7. PMID:36018461; PMCID:PMC9512860.
Fan S, Shi XY, Zhao CF, Chen Z, Ying J, Yu SP, et al. Efficacy and safety of single-dose intravitreal dexamethasone implant in non-infectious uveitic macular edema: A systematic review and meta-analysis. Frontiers in medicine. 2023;10:1126724. doi:10.3389/fmed.2023.1126724. PMID:36873888; PMCID:PMC9982842.
Angeles-Han ST, Lo MS, Henderson LA, Lerman MA, Abramson L, Cooper AM, Parsa MF, Zemel LS, Ronis T, Beukelman T, Cox E, Sen HN, Holland GN, Brunner HI, Lasky A, Rabinovich CE, Juvenile Idiopathic Arthritis Disease-Specific and Uveitis Subcommittee of the Childhood Arthritis Rheumatology and Research Alliance. Childhood Arthritis and Rheumatology Research Alliance Consensus Treatment Plans for Juvenile Idiopathic Arthritis-Associated and Idiopathic Chronic Anterior Uveitis. Arthritis Care Res (Hoboken). 2019;71(4):482-491. doi:10.1002/acr.23610. PMID:29806733; PMCID:PMC6261704.
Haydinger CD, Ferreira LB, Williams KA, Smith JR. Mechanisms of macular edema. Front Med (Lausanne). 2023;10:1128811. doi:10.3389/fmed.2023.1128811. PMID:36960343; PMCID:PMC10027768.
Jasmin A Branford, Bahram Bodaghi, Lisia Barros Ferreira, Peter J McCluskey, Jennifer E Thorne, Janet M Matthews, International Study Group for Systemic Immunomodulatory Drug Treatment of Non‐Infectious Uveitis, Justine R Smith. Use of immunomodulatory treatment for non-infectious uveitis: an International Ocular Inflammation Society report of real-world practice. Br J Ophthalmol. 2024;109(4):482-489. doi:10.1136/bjo-2024-326239.
Lowder C, Belfort R Jr, Lightman S, et al. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis (HURON). Arch Ophthalmol. 2011;129(5):545-553. doi:10.1001/archophthalmol.2010.339.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.