When malignant lymphoma first occurs in the eye without systemic lymphoma, it is called primary intraocular lymphoma (PIOL). Since it often forms lesions in the retina and vitreous, it is also recently referred to as vitreoretinal lymphoma (VRL). Because the malignant lymphocytes infiltrate the eye and present uveitis-like ocular findings, it is known as one of the classic masquerade syndromes. Many cases are complicated by central nervous system lymphoma (PCNSL) and often follow a fatal course.
Most primary intraocular lymphomas are histologically diffuse large B-cell lymphoma (DLBCL). They are highly malignant and differ greatly in pathology and prognosis from low-grade MALT lymphoma, which is more common in the ocular adnexa. Most malignant lymphomas in the ophthalmic field are non-Hodgkin lymphomas, and PIOL falls into this category.
QIf uveitis does not respond to steroids, what should be suspected?
A
When uveitis does not respond to steroid treatment (eye drops or oral), primary intraocular lymphoma (PIOL) must always be considered as a key differential diagnosis. PIOL is also called “masquerade syndrome” and presents findings very similar to inflammatory uveitis. Furthermore, steroids may temporarily lyse lymphoma cells and improve symptoms, leading to false-negative results in subsequent biopsies. Particularly suspect PIOL when vitreous opacity is severe but visual acuity is good. Measurement of the IL-10/IL-6 ratio and vitreous biopsy for definitive diagnosis are essential.
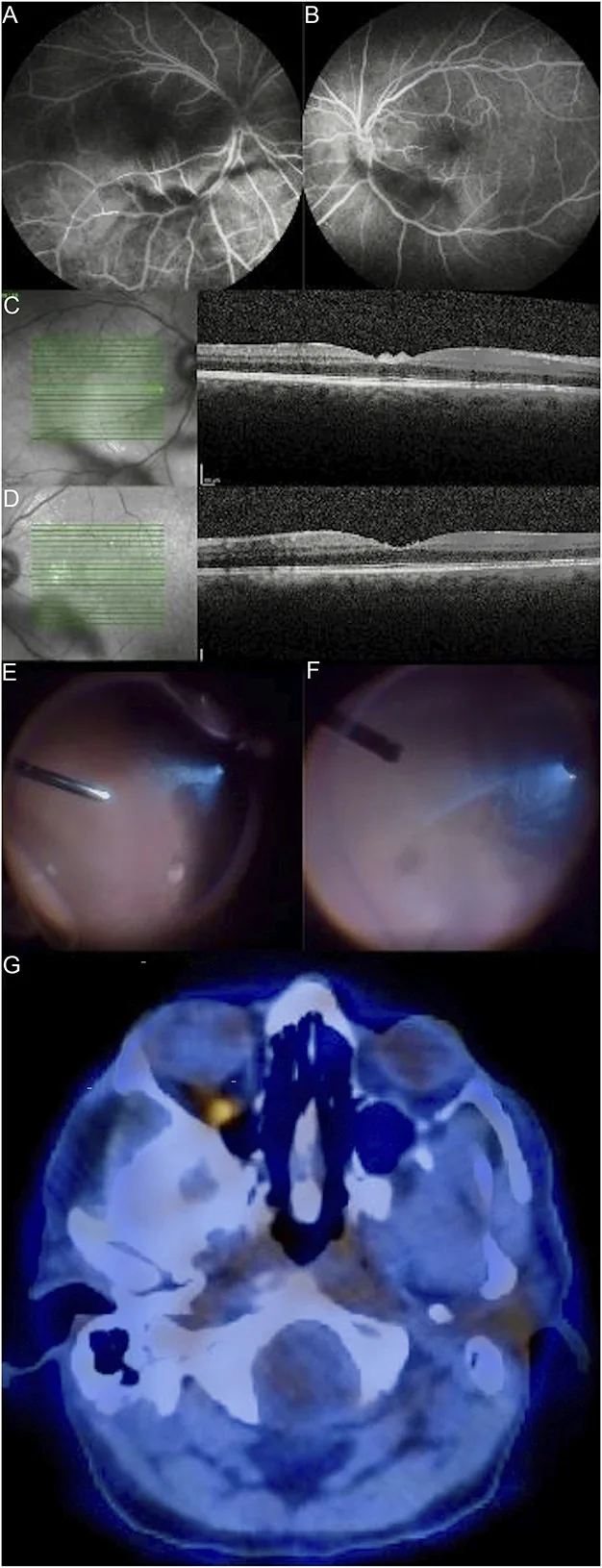
Naia L, Tavares M, Ferreira C, et al. Primary vitreoretinal lymphoma masquerading as refractory uveitis-just go with the flow. Porto Biomed J. 2024;9(5):268. Figure 1. PMID: 39403702; PMCID: PMC11469907; DOI: 10.1097/j.pbj.0000000000000268. License: CC BY 4.0.
Fluorescein angiography (A, B) and optical coherence tomography (C, D) of the right and left eyes show moderate vitritis. In the specimen from vitrectomy (fourth column), sheet-like clusters of homogeneous large cells exhibit an “aurora borealis” pattern. This corresponds to the band-like and cord-like vitreous opacities discussed in the section “2. Main symptoms and clinical findings”.
Blurred vision is the most common subjective symptom. Visual acuity that is disproportionately good relative to the severity of vitreous opacities is an important clue for suspecting this disease.
Characteristics of vitreous opacities
Band-like and cord-like pattern: A unique pattern radiating from the posterior pole to the periphery.
Aurora-like opacities: High cell density, and dynamic observation reveals vitreous opacities described as “aurora-like”.
Irregularly sized cells: High-density lymphoma cells are present in varying sizes.
Discrepancy with preserved vision: Visual acuity is good relative to the severity of opacities, which is key to suspecting this disease.
Retinal and RPE findings
Yellow-white patchy lesions: Lymphoma cells infiltrate beneath the retinal pigment epithelium (RPE) and Bruch’s membrane, forming yellow-white punctate to patchy lesions.
Confluence and enlargement of lesions: Small punctate lesions coalesce and enlarge into large lesions.
Papillitis-like findings: Tumor cell infiltration into the subretinal space around the optic disc may cause papillitis-like findings (rare).
Vascular sheathing: Vascular sheathing resembling retinal vasculitis may also be observed.
At the time of intraocular recurrence, the frequency of keratic precipitates (KP) tends to increase compared to the initial onset, as reported in the literature 2).
QHow is PIOL diagnosed?
A
A definitive diagnosis of PIOL requires a vitreous biopsy performed similarly to vitrectomy. Using the collected vitreous fluid, diagnosis is made by combining cytology, IL-10/IL-6 ratio measurement, PCR for IgH gene rearrangement, and flow cytometry. Cytology alone has a low positivity rate of about 50%, but combinations such as IL-10/IL-6 ratio >1 (sensitivity 89.4%), flow cytometry (sensitivity 88.0%), and PCR (sensitivity 85.1%) are useful 1). If steroids have been used before diagnosis, there is a risk of false negatives, so steroids should be discontinued as much as possible before performing the biopsy.
The mean age at diagnosis is 63 years, with a slight female predominance. The incidence is about 1–2% of uveitis cases at university hospitals. Ocular symptoms are seen in 15–20% of patients with central nervous system lymphoma.
In a case series of 10 patients (17 eyes) from Hong Kong, the median age was 59 years, 70% were female, and 70% had bilateral involvement 1). A retrospective study of 51 cases from Shanghai reported bilateral involvement in 78.4% 2). This indicates that the disease is often bilateral, and even when it presents unilaterally, careful examination and follow-up of the contralateral eye are important.
There is often a delay from onset to definitive diagnosis (average 12–18 months due to masquerade syndrome 3)). Immunodeficiency (e.g., HIV infection) and immunosuppressive states (e.g., post-organ transplant, use of immunosuppressive drugs) are considered risk factors.
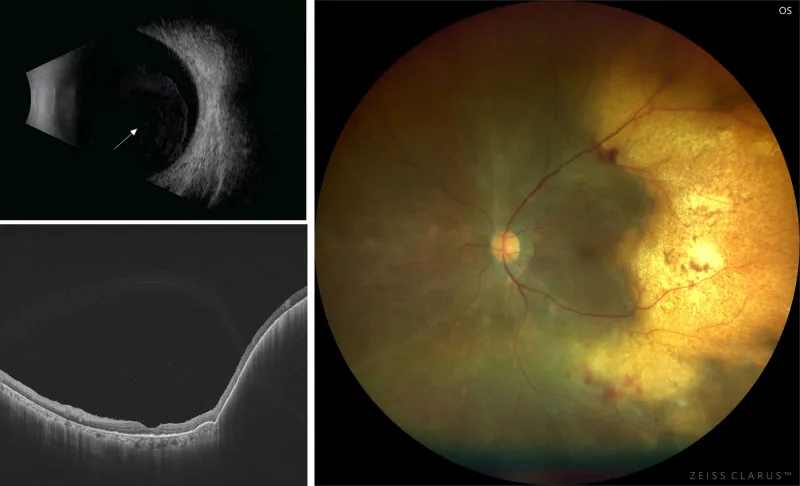
Wang SY, Zhou SW, Gao J, Wang L. Primary vitreoretinal lymphoma: diagnosis, treatment, and prognosis-a review of current knowledge and future directions. Blood Sci. 2025;7(2):e00233. doi:10.1097/BS9.0000000000000233. PMID:40322320. PMCID:PMC12047895. Figure 1. License: CC BY 4.
Multimodal imaging of a 75-year-old woman: B-scan ultrasound (upper left) shows extensive opacity of the posterior vitreous; OCT (lower left) reveals confluent RPE detachment and homogeneous hyperreflective mass under the RPE on the temporal side of the macula; fundus photograph (right) shows a ring-shaped yellow-white elevated lesion with small pigment spots on the temporal side of the macula. This corresponds to the OCT hyperreflective sub-RPE infiltration and yellow-white subretinal lesion discussed in section “4. Diagnosis and examination methods”.
For a definitive diagnosis, a vitreous biopsy similar to vitrectomy is performed. Cytology alone may not confirm the diagnosis; it is essential to combine it with PCR for immunoglobulin gene rearrangement and cytokine measurement.
Detection rate approximately 30% higher than cellular DNA1)
Minimally invasive diagnosis. Also possible with aqueous humor9, 10)
6-item diagnostic framework
Sensitivity 97.5%, specificity 100%8)
High-precision diagnosis using composite indicators
While IL-10 in intraocular fluid is elevated, IL-6, which is elevated in inflammatory diseases, is lower than IL-10, and an IL-10/IL-6 ratio >1 has diagnostic value. However, during recurrence this ratio may decrease (only 43.8% >1), and an absolute IL-10 value ≥50 pg/mL is a more reliable indicator2).
Treatment of PIOL is based on a combination of local ocular therapy and systemic chemotherapy. Because the blood-retinal barrier (BRB) limits intraocular penetration of systemic chemotherapy, local treatment is essential for controlling intraocular disease.
Methotrexate (Methotrexate Injection 200 mg) is injected intravitreally at 400 μg/0.1 mL. The standard protocol is as follows.
Induction phase: Twice a week for 4 weeks
Consolidation phase: Once a week for 8 weeks
Maintenance phase: Once a month for 9 months
In a Hong Kong series, a complete remission rate of 77.8% was reported with a median of 5 injections 1). A low dose of 400 μg/0.05 mL is also used. A large study with 20 years of experience showed a complete remission rate of 97% 6).
Main side effects: Keratopathy (33–100%). Managed with preservative-free eye drops, bandage contact lenses (BCL), and oral folic acid 1).
Local ocular irradiation with a total dose of about 30 Gy is effective. It is indicated for bilateral cases, elderly patients, those intolerant to MTX, or those with difficulty attending clinic visits. However, there are risks of side effects such as radiation retinopathy, optic neuropathy, and cataract, and MTX injection is generally preferred if feasible 4).
Some patients achieve complete remission after diagnostic vitrectomy (Hong Kong series: 75% 1), another report: 19.7% 7)). The mechanism is thought to involve removal of the scaffold for lymphoma cell proliferation and reduction of tumor burden. It is an option for patients intolerant to or refusing MTX.
Systemic chemotherapy (when combined with central nervous system lymphoma)
High-dose MTX therapy: Methotrexate 100–200 mg/kg (5–10 g per dose for adults) intravenous infusion
Leucovorin rescue: Starting the next day, leucovorin injection 5 ampules in 100 mL normal saline, 4-hourly for 4 doses, intravenous infusion for 3 days
Must be administered according to protocol with strict management of fluid intake, urine output, and urine pH
Whole brain irradiation (WBRT) may be added if necessary, but due to the risk of side effects including leukoencephalopathy, the indication should be carefully considered, especially in elderly patients.
Combination of systemic chemotherapy and intravitreal chemotherapy may reduce the risk of intraocular recurrence. A history of no prior intravitreal chemotherapy has been reported as an independent risk factor for intraocular recurrence 2), highlighting the importance of aggressive local ocular treatment.
Most (over 95%) primary intraocular lymphomas correspond to diffuse large B-cell lymphoma (DLBCL). It is a malignant tumor caused by monoclonal proliferation of lymphoid cells, and in contrast to low-grade MALT lymphoma, which is common in the ocular adnexa, it is extremely aggressive.
MYD88 L265P mutation is frequently detected in PVRL/PCNSL. This mutation leads to constitutive activation of Toll-like receptor signaling, persistently activating the NF-κB pathway to maintain tumor cell proliferation and survival 6). BTK (Bruton’s tyrosine kinase) is also located downstream of this pathway and is attracting attention as a therapeutic target.
High expression of VEGF and IL-10 contributes to immune evasion of tumor cells. IL-10 is a cytokine produced by the tumor cells themselves and is involved in the formation of an immunosuppressive environment.
It is thought that tumor cell transformation occurs outside the CNS and then migrates into the immune-privileged eye 3). Because the blood-retinal barrier (BRB) limits the intraocular penetration of systemic chemotherapy, local treatments such as intravitreal injection and ocular radiotherapy are essential for controlling intraocular lesions.
Vitreous cavity (main site of lymphoma cell proliferation)
Retinal pigment epithelium (RPE) (starting point of subretinal infiltration)
Sub-Bruch’s membrane (lesion formation between RPE and Bruch’s membrane)
Vitreous opacities appear band-like or cord-like, showing a unique pattern radiating from the posterior pole to the periphery. Lymphoma cells infiltrating the retina gradually form yellowish-white patchy lesions, which may coalesce and enlarge.
PIOL and PCNSL share many similarities in gene expression profiles, and they are understood to belong to the same disease spectrum 3). This underlies the high frequency of CNS involvement in patients with PIOL.
Detection of MYD88 mutations using cell-free DNA in vitreous humor and aqueous humor is attracting attention. The detection rate is approximately 30% higher than that of cellular DNA 1), and it is effective even in highly diluted samples. Detection in aqueous humor (using ultra-sensitive ddPCR for MYD88 L265P mutation) has been reported 9, 10), and its application is expected in cases where vitreous biopsy is difficult.
A retrospective study of 51 cases suggests that combining systemic chemotherapy with intravitreal chemotherapy may reduce the risk of intraocular recurrence 2). Further prospective studies are needed to determine the optimal dosing schedule.
QWhat is the risk of progression to central nervous system lymphoma?
A
In PIOL, a considerable number of cases eventually develop CNS lesions. 55.6% of isolated PVRL (eye only) developed new CNSL (central nervous system lymphoma), with a median time of 35.1 months 2). In a Hong Kong series, CNS lesions were found in 7 out of 10 cases (70%), and in 57.1%, ocular lesions preceded CNS lesions 1). Therefore, even after intraocular lesions are confirmed, regular CNS evaluation with gadolinium-enhanced head MRI is essential. Although intraocular recurrence has been reported not to directly affect CNS recurrence rate or overall survival 2), prognosis after CNS lesion development remains often poor.
Chee ASH, Mak ACY, Kam KW, et al. Diagnostic challenges and treatment outcomes of primary vitreoretinal lymphoma in Hong Kong. Hong Kong Med J. 2024.
Liu S, Jiang T, Gu J, Zhou X, Chen W, Ping B, Zhou Y, Zhang T, Huang X, Xu G, Chang Q.. Prognosis, Risk Factors, and Clinical Features of Intraocular Recurrence in Primary Vitreoretinal Lymphoma. Ophthalmol Retina. 2024;8(4):317-324. doi:10.1016/j.oret.2023.10.021. PMID:37918656.
Raval V, Binkley E, Aronow ME, Valenzuela J, Peereboom DM, Singh AD.. Primary central nervous system lymphoma - ocular variant: an interdisciplinary review on management. Surv Ophthalmol. 2021;66(6):1009-1020. doi:10.1016/j.survophthal.2021.03.004. PMID:33762182.
Riemens A, Bromberg J, Touitou V, Sobolewska B, Missotten T, Baarsma S, Hoyng C, Cordero-Coma M, Tomkins-Netzer O, Rozalski A, Tugal-Tutkun I, Guex-Crosier Y, Los LI, Bollemeijer JG, Nolan A, Pawade J, Willermain F, Bodaghi B, ten Dam-van Loon N, Dick A, Zierhut M, Lightman S, Mackensen F, Moulin A, Erckens R, Wensing B, le Hoang P, Lokhorst H, Rothova A.. Treatment strategies in primary vitreoretinal lymphoma: a 17-center European collaborative study. JAMA Ophthalmol. 2015;133(2):191-197. doi:10.1001/jamaophthalmol.2014.4755. PMID:25412269.
Ryan S. Huang, Andrew Mihalache, Marko M. Popovic, Miguel Cruz-Pimentel, Bhadra U. Pandya, Rajeev H. Muni, Peter J. Kertes. Diagnostic methods for primary vitreoretinal lymphoma: A systematic review. Survey of Ophthalmology. 2024;69(3):456-464. doi:10.1016/j.survophthal.2023.12.001.
Zohar Habot‐Wilner, Shahar Frenkel, Jacob Pe’er. Efficacy and safety of intravitreal methotrexate for vitreo‐retinal lymphoma – 20 years of experience. Br J Haematol. 2021;194(1):92-100. doi:10.1111/bjh.17451.
Zhang X, Zhang Y, Guan W, Zou D, Zhao C, Gao F, Dai RP, Yu WH, Chen YX, Min HY, Zhang M, Zhang W, Peng X. Development of Diagnostic Recommendations for Vitreoretinal Lymphoma. Ocul Immunol Inflamm. 2024;32(7):1142-1149. doi:10.1080/09273948.2023.2173242. PMID:36758245.
Hiemcke-Jiwa LS, Leguit RJ, Radersma-van Loon JH, et al. Molecular analysis in liquid biopsies for diagnostics of primary vitreoretinal lymphoma: review of current evidence. Surv Ophthalmol. 2019;64(1):10-16.
Demirci H, Rao RC, Bhatt MD, et al. Aqueous humor-derived MYD88 L265P mutation analysis in vitreoretinal lymphoma: A Potential Less Invasive Method for Diagnosis and Treatment Response Assessment. Ophthalmol Retina. 2023;7(2):189-195. doi:10.1016/j.oret.2022.08.005.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.