Conjunctival malignant lymphoma is a malignant lymphoma originating from the conjunctiva due to monoclonal proliferation of B cells. It arises from conjunctiva-associated lymphoid tissue (CALT) and accounts for 25–30% of ocular adnexal lymphomas. 1)
The majority of these cases correspond to MALT lymphoma (lymphoma of mucosa-associated lymphoid tissue). Conjunctival MALT lymphoma is also called CALT lymphoma and tends to be low-grade, slowly progressive, and localized to the mucosa, which differs greatly in nature and prognosis from other high-grade lymphomas. In contrast, diffuse medium-cell and large-cell lymphomas have many mitotic figures and are likely to be metastases from lymphomas of other organs.
The incidence is rare at 0.2 per 100,000 people, accounting for 1–2% of all non-Hodgkin lymphomas. 1) It is more common after the age of 60, and the incidence of extranodal marginal zone lymphoma and follicular lymphoma showed an increasing trend from 1980 to 2005. 1) Although it is more common in the elderly, cases have been reported as early as 33 months of age. The incidence of ocular adnexal lymphoma in children is extremely rare at 0.12 per million. 1)
Histological subtypes in a series of 1014 cases are: extranodal marginal zone lymphoma 81%, follicular lymphoma (FL) 8%, mantle cell lymphoma (MCL) 3%, diffuse large B-cell lymphoma (DLBCL) 3%, with 98% being B-cell lineage. 1) Most are non-Hodgkin B-cell lymphomas, consistent with the overall trend of ocular lymphomas.
Historically, Arnold and Becker first reported it in 1872, and Isaacson established the concept of mucosa-associated lymphoid tissue (MALT) in 1984. 1) The WHO 2017 classification defines over 80 subtypes. 1)
QHow common is conjunctival malignant lymphoma?
A
The incidence is 0.2 per 100,000 population, accounting for 25–30% of all ocular adnexal lymphomas. 1) It is a rare disease, corresponding to 1–2% of all non-Hodgkin lymphomas. It is more common after the age of 60, and extremely rare in children, with an incidence of 0.12 per million. 1)
QWhat is MALT lymphoma?
A
MALT lymphoma (mucosa-associated lymphoid tissue lymphoma) is a general term for low-grade B-cell lymphomas arising from mucosal tissues such as the gastrointestinal tract, salivary glands, lungs, orbit, and conjunctiva. It originates from lymphoid tissue acquired locally due to chronic inflammation or infection, and is characterized by slow progression and local confinement. Those originating in the conjunctiva are called CALT lymphoma and have a relatively good prognosis.
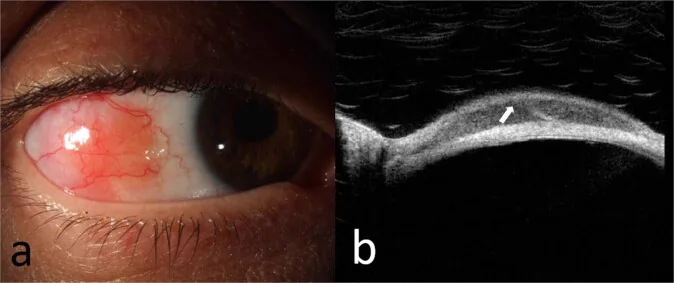
McGrath LA, et al. Conjunctival Lymphoma. Eye (Lond). 2023. Figure 5. PMCID: PMC10049989. License: CC BY.
Slit-lamp photograph (a) of extranodal marginal zone lymphoma of the bulbar conjunctiva, and OCT image (b) of the lesion showing hypo-reflective homogeneous subepithelial infiltration and a hyper-reflective subepithelial band. This corresponds to the conjunctival lesion discussed in the section “2. Main Symptoms and Clinical Findings.”
The main symptom is a conjunctival mass, often with little foreign body sensation. Some cases are diagnosed after long-term treatment as chronic conjunctivitis.
Mass/Protrusion: Perceived as a slowly enlarging conjunctival mass.
Foreign body sensation/mild discomfort: 85% have some symptoms, and 67% are considered mild. 1)
Salmon-pink, translucent, elevated lesions appear on the fornix and bulbar conjunctiva. It is difficult to distinguish them from reactive lymphoid hyperplasia (RLH) based on appearance alone.
The most common site is the conjunctival fornix, and as it progresses, it may spread to the entire conjunctiva. It is also important to evert the upper eyelid conjunctiva for examination. Over 90% appear pink, with typical findings of a base diameter of 15 mm, thickness of 3 mm, and 2–3 lesions per eye. 1) Unilateral involvement accounts for 2/3 of cases (82% for extranodal marginal zone lymphoma), and 62% occur in the superior or inferior conjunctiva. Only 7% reach the limbus. 1) Bilateral involvement can occur, either simultaneously or after an interval of years in the contralateral eye.
Distribution: Commonly occurs in the fornix and bulbar conjunctiva. Mostly unilateral (82%). 1)
Characteristics: Low-grade, slowly progressive. Most common subtype (81%). Good prognosis.
Follicular / Mantle Cell Lymphoma
Follicular lymphoma: Often presents as multinodular lesions. 1)
Mantle cell lymphoma: Large, dark red mass. 1)
Characteristics: Follicular lymphoma is low-grade. Mantle cell lymphoma is often associated with systemic disease.
Diffuse Large B-Cell / T-Cell
Diffuse large B-cell lymphoma: Grayish, rapidly enlarging mass. 1)
T-cell lymphoma: 30% occur at the limbus. Some cases are accompanied by scleritis. 1)
Characteristics: High grade. Urgent management required.
QSalmon-pink mass = lymphoma?
A
A salmon-pink conjunctival mass can also appear similar in reactive lymphoid hyperplasia. Differentiation based on appearance alone is difficult, and biopsy is always necessary for definitive diagnosis. See “Diagnosis and Testing Methods” section for details.
The pathogenesis of conjunctival malignant lymphoma is thought to involve B-cell dysregulation due to chronic antigenic stimulation. Normally, lymphoid tissue is absent in the conjunctiva, but persistent chronic inflammation leads to the acquisition of mucosa-associated lymphoid tissue, from which MALT lymphoma arises.
Infectious agents: Associations with Helicobacter pylori, Chlamydophila psittaci, hepatitis C virus, and HIV have been reported. 1) The association with C. psittaci is more frequently reported in Europe, and the positivity rate varies by region.
Autoimmune diseases: Associations with Sjögren’s syndrome, Hashimoto’s thyroiditis, and IgG4-related disease. 1)
Conjunctival microbiota: Delftia sp. (Gram-negative bacillus) may be involved. 1)
Association with reactive lymphoid hyperplasia: Reactive lymphoid hyperplasia is considered a precursor condition. 1)
Histopathological examination via biopsy is essential for definitive diagnosis. Diagnosis cannot be made based on clinical findings or imaging alone. Malignant lymphoma is monoclonal, whereas reactive lymphoid hyperplasia is polyclonal, and this distinction is key to differentiation.
Biopsy involves partial or complete excision of the tumor for pathological evaluation. A biopsy specimen of at least 250 mg is recommended (necessary for gene rearrangement testing). Since conjunctival lymphoma grows thinly and widely, techniques such as dividing the excision into two sites may be needed to avoid symblepharon.
HE staining + immunohistochemistry: Confirm the lineage and clonality of the lymphocyte population. Use CD10, CD20, CD79a, CD5, etc.
Flow cytometry: Can be performed if sufficient sample is available. Allows rapid determination of tumor cell lineage and differentiation.
Gene rearrangement analysis: Examine the presence of immunoglobulin/T-cell receptor gene rearrangements by Southern blot or PCR. In malignant lymphoma, a monoclonal rearrangement pattern is consistent across all tumor cells, distinguishing it from polyclonal reactive lymphoid hyperplasia.
Once a diagnosis of malignant lymphoma is made, a systemic search for the primary lesion should be performed. It is important to collaborate with a hematologist for staging.
The following are used for systemic evaluation:
FDG-PET/CT: Used for systemic staging. 1)
Bone marrow biopsy: Evaluates the presence of systemic dissemination.
Serum LDH and β2-microglobulin: Used as tumor markers for reference.
Staging is assessed using the Ann Arbor classification (Lugano classification may also be applied for ocular adnexal lymphoma) and directly determines the treatment strategy.
Stage
Definition
Treatment guideline
Stage IE (localized)
Confined to conjunctiva or ocular adnexa
Radiation therapy is first-line
Stage IIE or higher
Involvement of lymph nodes or other organs
Consider systemic chemotherapy
Auxiliary Imaging Tests and Differential Diagnosis
High-resolution optical coherence tomography (HR-OCT): Can be used for supplementary evaluation, but definitive diagnosis is only possible by pathology. 1)
Differential diagnoses: It is necessary to differentiate from reactive lymphoid hyperplasia, IgG4-related eye disease, chronic conjunctivitis, pterygium, pyogenic granuloma, etc. 1)
QCan conjunctival lymphoma be diagnosed without a biopsy?
A
High-resolution optical coherence tomography provides supplementary information, but definitive diagnosis is only possible by histopathological examination of a biopsy. 1) PET/CT is useful for systemic staging but is not used for local diagnosis. Confirmation of monoclonality by gene rearrangement analysis (PCR or Southern blot) provides the basis for definitive diagnosis.
Treatment is performed in collaboration between hematology and ophthalmology. Complete surgical resection is difficult; the disease is highly radiosensitive and also responds well to chemotherapy. The treatment strategy is determined according to the stage (Ann Arbor classification) and histological subtype.
When reactive lymphoid hyperplasia is suspected, observation with 0.05% cyclosporine A eye drops (2-4 times daily) or low-concentration steroid eye drops may be considered first. Regression may be achieved in some cases, but if malignancy is diagnosed, promptly transition to the following treatments.
Treatment of Localized Disease (Ann Arbor Stage IE)
Radiation therapy is the first choice. It is particularly effective for extranodal marginal zone lymphoma (MALT lymphoma). During irradiation, the eye is protected with a lead contact lens. Electron beam irradiation may also be used.
External beam irradiation of 24 Gy in 12 fractions has been reported to achieve a 5-year local control rate of 89-100%. 1) Ultra-low-dose irradiation (4 Gy in 2 fractions) for reducing side effects has achieved a complete response rate of 85% and a 2-year control rate of 75%. 1)
Rituximab monotherapy (375 mg/m² × 4 courses) is also an option. 1) Intralesional rituximab injection (50 mg) is used for recurrent cases or those desiring local treatment, with a reported complete response rate of 73%. 1)
For CD20-positive lymphoma, R-CHOP therapy (rituximab 375 mg/m² + CHOP) is selected. Interferon alpha-2b (1-1.5 MIU subcutaneously three times a week) has been reported to achieve a 5-year progression-free survival rate of 85% in low-grade, localized cases. 1)
In cases positive for Chlamydophila psittaci by PCR, antibiotic therapy with doxycycline 100 mg twice daily has been attempted, with a reported 5-year progression-free survival rate of 55%. 1)
The response data for each treatment method are shown below.
The IELSG-19 trial showed 5-year progression-free survival of 68% vs 51% and response rate of 95% vs 86% for rituximab plus chlorambucil versus chlorambucil alone.1) Cryotherapy has been reported to achieve lesion regression in 98% of 42 cases.1)
For T-cell lymphoblastic lymphoma, hyper-CVAD+HD-MA therapy has been reported to achieve complete response in 91%, 3-year progression-free survival of 66%, and 3-year overall survival of 70%.2)
QHow long is follow-up needed after treatment?
A
Extranodal marginal zone lymphoma has been reported to progress to systemic disease in about 20% of cases even after treatment, and dissemination after more than 10 years is occasionally observed.1) Long-term regular check-ups are necessary for early detection of recurrence and systemic progression. The interval and duration of follow-up should be determined in consultation with the attending physician.
Conjunctival malignant lymphoma originates from conjunctival-associated lymphoid tissue (present at the limbus and fornix). Normally, lymphoid tissue is absent in the conjunctiva, but chronic inflammation, infection, or autoimmune stimulation leads to acquired mucosa-associated lymphoid tissue, in which lymphomagenesis occurs.
Molecular mechanisms of extranodal marginal zone lymphoma (MALT lymphoma)
Analysis of immunoglobulin/T-cell receptor gene rearrangements is useful for determining whether a proliferation is neoplastic (malignant) or reactive (benign). If monoclonal proliferation is confirmed, it is considered malignant; if polyclonal, it is treated as reactive. Even if clinical findings are similar, this molecular biological test is essential for a definitive diagnosis.
Sugawara et al. (2022) reported an extremely rare case of precursor T-cell lymphoblastic lymphoma arising in the conjunctiva. A 61-year-old man presented with a salmon-pink conjunctival mass, which was CD7+, CD10+, TdT+, and CD20−. The 5-year overall survival rate for adult T-cell lymphoblastic lymphoma, which accounts for about 2% of all lymphomas, is poor at 26%. 2)
Comprehensive genetic mutation analysis using next-generation sequencing is advancing the identification of prognostic markers. 1) Expression of BCL-6, MUM1/IRF4, and Ki-67, tumor diameter >30 mm, and Ki-67 >10% are noted as poor prognostic factors. 1)
Treatment Monitoring with High-Resolution Optical Coherence Tomography
The utility of non-invasive treatment effect monitoring using high-resolution optical coherence tomography is being investigated. 1) It may allow tracking of tumor changes without repeated biopsies.
An association between conjunctival microbiota, including Delftia sp. (gram-negative rods), and the development of conjunctival lymphoma has been suggested, and research is progressing as a new pathway of chronic antigen stimulation. 1)
The application of molecular targeted drugs, including BTK inhibitors, to conjunctival lymphoma is being investigated. 1) They are expected as new treatment options for relapsed/refractory cases.
McGrath LA, Ryan DA, Warrier SK, Coupland SE, Glasson WJ. Conjunctival Lymphoma. Eye. 2023;37:837-848.
Sugawara R, Usui Y, Takahashi R, Nagao T, Goto H.. A case of conjunctival precursor T cell lymphoblastic lymphoma presenting with salmon colored conjunctival mass. Am J Ophthalmol Case Rep. 2022;25:101382. doi:10.1016/j.ajoc.2022.101382. PMID:35243143; PMCID:PMC8859792.
Baltă AC, Mihai MA, Ionescu AM, Radu M, Chițac I, Murgoi G, et al. Conjunctival lymphoma: case report. Rom J Ophthalmol. 2025;69(3):440-449. PMID: 41189780.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.