Conjunctival malignant melanoma is a malignant tumor originating from melanocytes of the conjunctiva. It is common in Western countries but rare in Japan. It often arises from primary acquired melanosis (PAM).
The global incidence is 0.3–0.8 per million per year, highest in Northern Europe and North America. It has been increasing over the past 50 years. In the United States, approximately 130 new cases per year are estimated, and in Europe about 320 cases 8). The age-adjusted incidence in Asians is low at 0.15 per million per year, and it is most common in Caucasians (91.2%) 1, 8).
The mean age at onset is 55–65 years, and onset under 20 years is extremely rare 1, 4, 5, 6). The 5-year disease-specific survival rate is approximately 82.9%, and 69.3% at 10 years 8).
Conjunctival melanoma is the only mucosal melanoma for which an association with ultraviolet exposure has been suggested, because the bulbar conjunctiva is directly exposed to UV light 4).
QHow rare is conjunctival malignant melanoma?
A
The incidence of conjunctival malignant melanoma is 0.3–0.8 per million per year, making it a rare disease, but it has been increasing over the past 50 years. Asians have a lower risk of developing the disease compared to Caucasians, with a reported incidence of 0.15 per million per year. Pediatric cases account for only 1% of all conjunctival melanomas, and onset under age 20 is extremely rare.
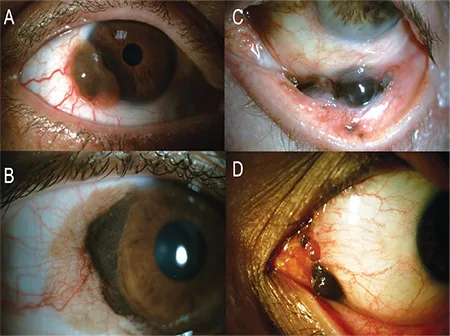
Koç İ, Kiratlı H. Current Management of Conjunctival Melanoma Part 1: Clinical Features, Diagnosis and Histopathology. Turk J Ophthalmol. 2020;50(5):293-303. Figure 1. PMCID: PMC7610047. License: CC BY.
A) Conjunctival melanoma at the limbus with pigmented elevated lesion and abundant feeder vessels; B) Large limbal melanoma arising from diffuse PAM; C) Melanoma localized in the fornix; D) Melanoma involving the caruncle and plica semilunaris. These correspond to the sites and clinical forms of conjunctival malignant melanoma discussed in section “2. Main symptoms and clinical findings.”
Clinically, it appears as a dark brown elevated lesion on the bulbar or palpebral conjunctiva, with abundant blood vessels feeding the tumor.
Pigmented melanoma (70%)
Predilection site: Approximately 90% occur on the bulbar conjunctiva, with 63% localized in the temporal quadrant 4, 6).
Appearance: A raised lesion that is dark brown to brownish. Accompanied by abundant feeding vessels directed toward the tumor.
Relationship with the sclera: Adhesion to the sclera may be observed. The average distance from the tumor to the corneal limbus is 2 mm, and 61% reach the limbus2).
Amelanotic melanoma (30%)
Appearance: A pink to red mass that contains little to no pigment.
Risk of misdiagnosis: Easily misdiagnosed as squamous cell carcinoma or other red conjunctival masses 3).
Prognosis: Hypopigmented and amelanotic types may be associated with a poor prognosis.
Yes. About 30% of conjunctival melanomas are amelanotic, appearing as pink to red masses. Amelanotic melanoma is easily misdiagnosed because it resembles squamous cell carcinoma and other lesions, which can delay diagnosis. Pathological diagnosis by biopsy is essential for suspicious conjunctival masses.
Lymphatic spread is the main route of metastasis. Temporal conjunctival lesions tend to metastasize to the preauricular lymph nodes, while nasal conjunctival lesions tend to metastasize to the submandibular lymph nodes. Distant metastases (hematogenous) occur in the brain, lungs, liver, skin, adrenal glands, etc.6, 1) Lymph node metastases are observed in 15–41% of cases at a median of 2.3 years after diagnosis, and systemic metastases occur in 9–25% at 3 years. Even when lymph node metastasis is not detected, distant hematogenous organ metastasis occurs in 38% of cases6).
QWhat is the most important factor affecting prognosis?
A
Major poor prognostic factors include tumor thickness (especially >2 mm), lesion location (caruncle has the worst prognosis), AJCC stage, nodular morphology, lymphatic invasion, and orbital invasion. Completeness of resection also greatly affects outcomes; approximately 49.3% of incomplete resection cases recur. Sentinel lymph node positivity increases the risk of death.
A biopsy is necessary for a definitive diagnosis. Histopathologically, it consists of proliferation of cells with large nucleus-to-cytoplasm ratios, containing melanin pigment and prominent nucleoli. If melanin pigment is abundant, depigmentation of the pathological specimen is required.
Immunohistochemical staining is essential for definitive diagnosis and differential diagnosis.
Surgical resection of the tumor including surrounding tissue is the mainstay. Intraoperative and postoperative topical administration of MMC or interferon alpha-2b is also effective. If the tumor is extensive with significant subconjunctival invasion, orbital exenteration may be necessary.
Surgical Therapy
Resection margin: Complete tumor resection with a 3–5 mm safety margin 4, 8)
No-touch technique: Avoid direct contact with the tumor using instruments to prevent tumor cell seeding 4, 8)
Dry technique: Resection without using irrigation fluid (BSS)
Corneal invasion: Alcohol corneal epithelial debridement + en bloc resection with a hockey knife 2)
Orbital exenteration: Indicated for extensive or recurrent cases (advanced cases)
To prevent tumor cell seeding (local recurrence or metastasis), this technique involves excising the tumor without directly touching it with instruments and in a dry environment without using irrigation fluid (BSS). The entire tumor is removed en bloc with a 3–5 mm safety margin to reduce the risk of recurrence due to incomplete resection. It fundamentally differs from standard excision by minimizing the seeding of tumor cells onto the conjunctiva.
Conjunctival melanoma is genetically similar to cutaneous melanoma rather than uveal melanoma. The main UV-related driver mutations (C>T transitions) are BRAF, NF1, and RAS. Uveal melanoma markers (BAP1, GNAQ, GNA11, SF3B1) are confirmed negative in conjunctival melanoma1).
TERT promoter mutation (c.-124C>T) affects telomerase reverse transcriptase and has been reported to be associated with metastatic conjunctival melanoma1, 8, 6). It is also detected in moderate to severe atypia of PAM (about 8%), suggesting a nature of melanoma in situ6). It has also been shown to be associated with high tumor mutational burden4). TERT mutations are found in 32–64% of conjunctival melanomas, and their association with prognosis is of interest8).
High PD-L1 expression and the presence of a transcriptional subtype rich in immune-related genes have been confirmed, providing a rationale for the use of immune checkpoint inhibitors. Data on BRAF inhibitors, MEK inhibitors, and PD-L1 inhibitors are promising but currently limited.
Chou et al. (2023) analyzed the molecular profile of a T3c conjunctival melanoma case in a 94-year-old man. They identified an NF1 mutation and a TERT promoter mutation (c.-124C>T, VAF 31.4%), with BRAF, NRAS, and cKIT all negative. The combination of NF1 mutation and NRAS negativity is considered a contributing factor to the relatively favorable course without metastasis1).
PD-1 inhibitors (pembrolizumab, nivolumab) and CTLA-4 inhibitors (ipilimumab) have been tried in metastatic and locally advanced conjunctival melanoma4, 8).
As a representative report, Sagiv et al. (2018) reported that PD-1 inhibition therapy with pembrolizumab or nivolumab was administered to 5 patients, with some achieving complete response8). A Phase 2 trial using the combination of axitinib + nivolumab (for untreated advanced or metastatic mucosal melanoma) is ongoing.
The standard regimen for systemic therapy for metastatic conjunctival melanoma has not yet been established, and careful case-by-case judgment is required.
For BRAF mutation-positive cases, BRAF inhibitor monotherapy (vemurafenib) or combination BRAF/MEK inhibitors (dabrafenib + trametinib, encorafenib + binimetinib) have been attempted 4, 8).
These drugs have been reported to reduce local tumors in some cases, but most reports are single cases or small series, and long-term outcomes are limited. The possibility of synergistic effects by simultaneously targeting the MAPK and AKT pathways is also under investigation 3).
Advances in Diagnostic Techniques and Molecular Classification
The use of immunohistochemical panels (PRAME, p16, HMB-45, Ki-67, Cyclin D1) is enabling reclassification of lesions previously considered “indeterminate” 5). International standardization of the C-MIL (conjunctival melanocytic intraepithelial lesion) classification (WHO 5th edition, 2022) is also progressing.
QCan immunotherapy be used for conjunctival melanoma?
A
Based on genetic similarities with cutaneous melanoma (BRAF, NF1, NRAS mutations, high PD-L1 expression), PD-1 inhibitors (pembrolizumab, nivolumab), CTLA-4 inhibitors, and BRAF inhibitors have been attempted in metastatic and locally advanced cases. However, large-scale clinical trials have not been conducted, and evidence is currently limited; no standard regimen has been established. There is an urgent need to accumulate large-scale data through international multicenter collaborative studies.
Chou LT, Lozeau DF, Boyle NS. A rare case of a long-standing, extensive and invasive conjunctival melanoma without systemic metastasis. Am J Ophthalmol Case Rep. 2023; PMC10121375.
Englisch CN, Berger T, Flockerzi F, et al. Conjunctival melanoma with pronounced central corneal invasion: one-year relapse free follow-up. Am J Ophthalmol Case Rep. 2024; PMC11403272.
Menna F, Tschopp M, Meyer P, et al. A case of conjunctival melanoma presenting as a squamous cell carcinoma. Case Rep Ophthalmol. 2024; PMC11509494.
Okongwu CC, Adewara BA, Olaofe OO, Soremekun AI, Ayodele SO, Abdullahi YO, et al. Malignant melanoma of the conjunctiva metastasizing to the submandibular gland: a case report and review of the literature. BMC Ophthalmol. 2025;25(1):130. doi:10.1186/s12886-025-03949-5. PMID:40082862. PMCID:PMC11905526.
Eder A, Milman T, Mudhar HS, et al. Unusual conjunctival melanocytic proliferations: report of five cases and review of the literature. Surv Ophthalmol. 2024; PMC12208716.
Goemaere J, Lauwers N, de Keizer ROB, et al. Bone metastasis in a case of primary acquired melanosis with atypia resulting from conjunctiva melanoma. Am J Ophthalmol Case Rep. 2023;29:101730. doi:10.1016/j.ajoc.2022.101730. PMID:36561878; PMCID:PMC9763362.
Vishnevskia-Dai V, Davidy T, Zloto O. Amelanotic conjunctival melanoma in a child. Am J Ophthalmol Case Rep. 2023; PMC9792290.
Butt K, Hussain R, Coupland SE, Krishna Y. Conjunctival melanoma: a clinical review and update. Cancers. 2023;15(3):922.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.