
Conjunctival Nevus
1. What is Conjunctival Nevus?
Section titled “1. What is Conjunctival Nevus?”Conjunctival nevus is a proliferation of nevus cells (immature pigment cells) in the conjunctival basal cells or subepithelium. It may also occur in the caruncle (the elevated area at the inner canthus involved in tear drainage) or the plica semilunaris.
Conjunctival nevus is the most common benign pigmented tumor of the conjunctiva and is frequently encountered in daily practice. Most occur in early childhood and remain stable after growth. Rarely, they can become malignant, so regular follow-up is important.
Epidemiology and Age Characteristics
Section titled “Epidemiology and Age Characteristics”- Most occur in early childhood (congenital or early childhood)
- Characteristics in childhood: Sparse pigmentation, appearing reddish. Melanin pigment becomes more distinct with age.
- Hormonal changes during puberty may alter color or size.
- Rapid changes after adulthood raise suspicion of malignancy.
- Overall risk of malignant transformation is about 1%1)
Positioning Among Conjunctival Melanocytic Tumors
Section titled “Positioning Among Conjunctival Melanocytic Tumors”Conjunctival nevi constitute the most benign and most common group of melanocytic tumors arising in the conjunctiva. Their relationship with other tumors is as follows:
- Conjunctival nevus: A raised pigmented lesion due to proliferation of nevus cells (this section)
- Conjunctival melanosis (PAM): A patchy pigmentation due to abnormal proliferation of melanocytes, without elevation
- Conjunctival malignant melanoma: Malignant transformation from PAM or nevus, accounting for about 2% of all ocular tumors
Most conjunctival nevi are benign, and if there are no cosmetic concerns or malignant features, observation alone is sufficient. However, if rapid enlargement, color change, increased thickness, or abundant tumor vessels are observed, there is a possibility of malignant transformation, and prompt consultation with a specialist for excisional biopsy should be considered.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”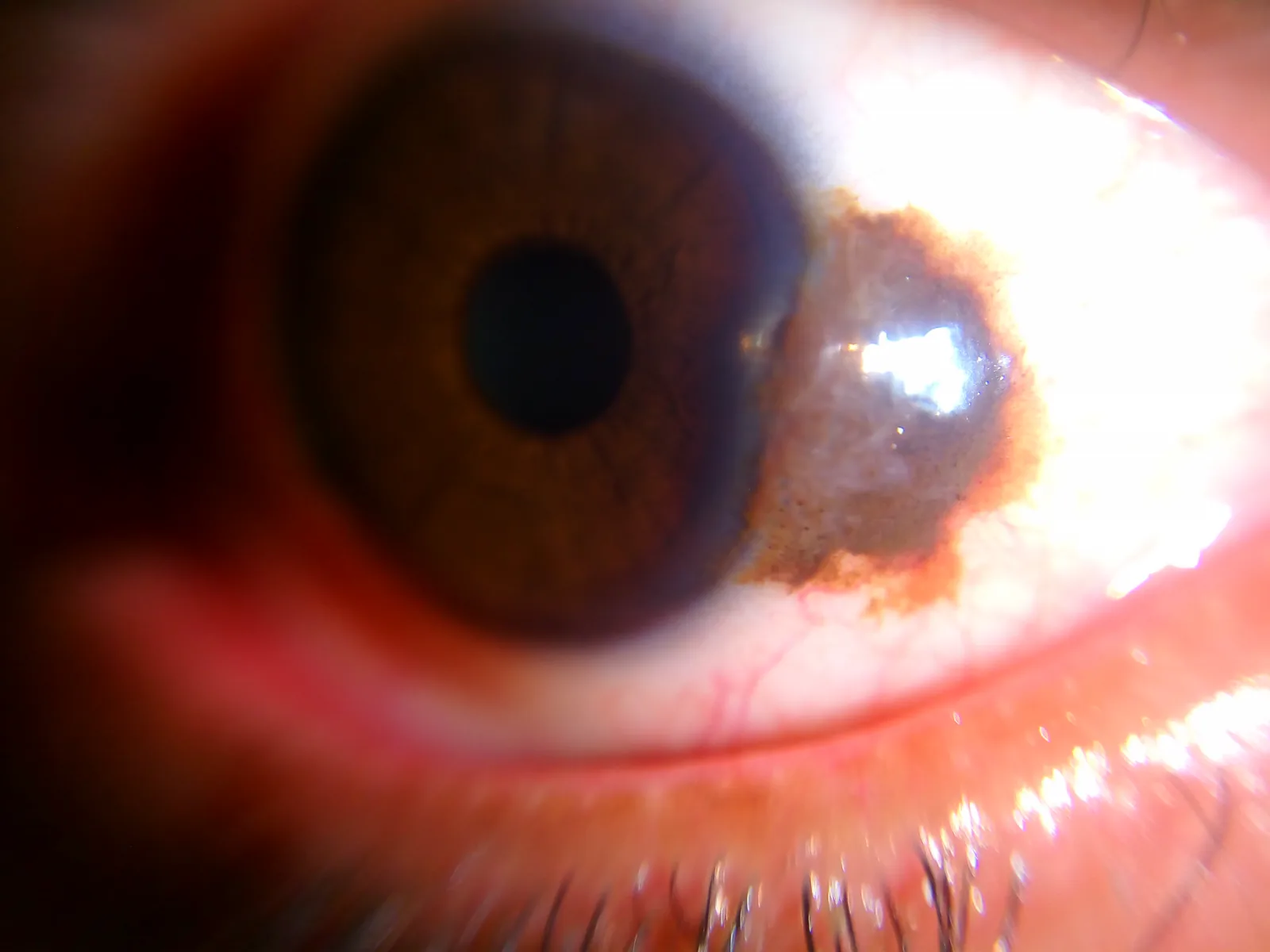
Subjective Symptoms
Section titled “Subjective Symptoms”Most subjective symptoms of conjunctival nevi are cosmetic concerns. Functional impairment is rare.
- Cosmetic concerns (a noticeable black-brown or reddish-brown lesion)
- Some patients present after noticing rapid growth or color change
- May be accompanied by irritation or foreign body sensation
Clinical Findings (Slit-Lamp Evaluation)
Section titled “Clinical Findings (Slit-Lamp Evaluation)”Observation with a slit lamp is essential for evaluating conjunctival nevi.
Findings suggestive of benignity:
- Tapioca-like appearance: Cyst-like findings (epithelial inclusion cysts) within the lesion, appearing like tapioca pearls under slit lamp. This is a key finding characteristic of nevi, and if present, the lesion is highly likely to be a nevus.
- Presence of conjunctival inclusion cysts: Can also be confirmed by ultrasound or anterior segment optical coherence tomography (AS-OCT)
- Bulbar conjunctiva near the corneal limbus: Commonly occurs in the interpalpebral fissure
- Caruncle and plica semilunaris: Lesions confined to these areas are also recognized as nevi
Findings suggestive of malignancy:
- Marked thickness or elevation of the lesion: Malignant melanoma often shows significant elevation
- Diffuse pigmentation: Scattered pigment with unclear borders
- Abundant tumor vessels (feeder vessels): Strongly suggestive of malignant melanoma
- Rapid enlargement: Clear increase in size over a short period
No. Among pigmented conjunctival lesions, benign nevi are the most common, with a malignant transformation risk of only about 1%. The location of the lesion, presence of tapioca-like cysts, age of onset, and pattern of change are important for differentiating benign from malignant. If suspicious changes occur, consultation with a specialist is recommended.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Mechanism of Development
Section titled “Mechanism of Development”Conjunctival nevi arise from the proliferation of nevus cells in the conjunctival basal layer or subepithelium during childhood. The cause is often congenital, and there is no clear association with exogenous risk factors.
- During childhood, nevus cells accumulate in the conjunctiva, forming benign proliferative nests.
- Most become stable after growth and do not regress spontaneously.
- Typically congenital or early childhood onset.
Risk of Malignant Transformation
Section titled “Risk of Malignant Transformation”The mechanism of malignant transformation is not fully understood, but the following points are relevant 1, 2).
- The overall risk of malignant transformation is low, about 1% 1).
- Temporary changes in color or size may occur during hormonal changes such as puberty or pregnancy.
- However, such changes due to hormonal fluctuations do not necessarily indicate malignant transformation.
- Rapid changes after adulthood (especially enlargement over weeks to months) are indicators of malignant transformation
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Clinical Diagnostic Procedure
Section titled “Clinical Diagnostic Procedure”When a dark brown raised lesion is seen on the conjunctiva macroscopically, it is difficult to differentiate between nevus, melanosis, and malignant melanoma based on appearance alone. Definitive diagnosis is made by pathological examination of the excised specimen.
Evaluation points with slit-lamp microscopy:
- Presence of tapioca-like cysts: If present, strongly suggests nevus
- Lesion thickness and elevation: Increased thickness or marked elevation suggests malignancy
- Pigment spread: Ill-defined pigment dispersion suggests malignancy
- Tumor vessels: Abundant tumor vessels suggest malignant melanoma
- Onset and course: Long-standing stable lesions since childhood suggest benignity. Rapid enlargement in adulthood requires caution
Imaging Studies
Section titled “Imaging Studies”- Anterior segment optical coherence tomography (AS-OCT): Allows evaluation of lesion depth, presence of cysts, and Bowman’s membrane
- Ultrasound biomicroscopy (UBM): Measures tumor thickness and checks for scleral invasion
- Ultrasound: Useful for detecting cysts associated with nevus
Differential Diagnosis
Section titled “Differential Diagnosis”| Differential Disease | Key Points for Differentiation |
|---|---|
| Conjunctival Melanosis (PAM) | No elevation, extensive patchy pigmentation, onset after middle age |
| Conjunctival Malignant Melanoma | Rapid growth, marked elevation, abundant tumor vessels, pigment leakage |
| Racial Pigmentation | Bilateral, common in palpebral fissure area, flat without elevation |
| Pigmented Lesion of Caruncle (Acquired) | Localized to caruncle, onset after adulthood |
Immunohistochemical Markers
Section titled “Immunohistochemical Markers”Histopathological examination is essential for definitive diagnosis and differentiation between benign and malignant. In the 5th edition of WHO, melanocyte marker immunohistochemistry has been adopted as a diagnostic criterion.
| Marker | Nevus | Melanoma | Remarks |
|---|---|---|---|
| S100 | + | + | Common melanocytic |
| SOX10 | + | + | Common melanocytic |
| HMB45 | + | + | Common melanocytic |
| Melan-A/MART-1 | + | + | Common melanocytic |
| Ki-67 | Low | 10–15% or higher | Proliferation index |
| p16 | Retained | Lost | Tumor suppressor marker |
| PRAME | − | + | Most useful marker for differentiating benign from malignant |
| bcl2 | − | Moderate to strongly positive | Apoptosis inhibition |
It refers to the finding that intraepithelial cysts formed inside a conjunctival nevus look like tapioca pearls when observed with a slit lamp. Cysts are histologically characteristic structures of nevi, and if this finding is confirmed, it is more likely to be a nevus than a malignant tumor. Since it is a clinically valuable diagnostic finding, it should always be checked during slit-lamp examination.
5. Standard Treatment
Section titled “5. Standard Treatment”Treatment Decision Flow
Section titled “Treatment Decision Flow”The treatment strategy is determined by the presence or absence of cosmetic issues and findings suggestive of malignancy.
- No cosmetic issues, no findings suggestive of malignancy → Regular follow-up including photographic documentation
- Cosmetic issues present or findings suggestive of malignancy present → Excisional biopsy
- Large lesions (when conjunctival scarring or symblepharon is a concern) → Combined with amniotic membrane transplantation
- Pathological examination of the excised specimen is mandatory (to confirm benign or malignant diagnosis)
Follow-up Observation
Section titled “Follow-up Observation”- If there are no cosmetic issues and no findings suggestive of malignancy, follow-up observation is standard.
- Photographic documentation: Take anterior segment photographs at each regular visit to objectively assess changes.
- Visit interval: If there are no clear changes, regular visits every 6 months to 1 year are common.
- Temporary changes in color or size due to hormonal changes during puberty do not necessarily indicate the need for excision.
Excisional Biopsy
Section titled “Excisional Biopsy”- Performed when there are cosmetic concerns or findings suggestive of malignancy (rapid growth, color change, increase in thickness).
- The excised specimen must always be submitted for pathological examination3).
- The principle is to excise with a safe margin.
Amniotic membrane transplantation
Section titled “Amniotic membrane transplantation”Amniotic membrane transplantation is combined when the excision site is large and there is concern about conjunctival scarring or symblepharon.
Effects of amniotic membrane transplantation:
- Anti-inflammatory effect: Reduces postoperative inflammation
- Anti-fibrotic effect: Suppresses postoperative conjunctival scar formation
- Anti-angiogenic effect: Suppresses unwanted new blood vessel formation
- Promotes good epithelialization and is effective in preventing symblepharon2).
When complete excision is performed, the risk of recurrence is low. However, incomplete excision may lead to recurrence. If malignant findings are found on pathological examination of the excised specimen, additional treatment or long-term follow-up is necessary. It is desirable to continue regular follow-up visits after surgery.
6. Pathophysiology and detailed pathogenesis
Section titled “6. Pathophysiology and detailed pathogenesis”Proliferation of nevus cells and histological features
Section titled “Proliferation of nevus cells and histological features”The development of conjunctival nevus is based on abnormal differentiation and proliferation of neural crest-derived pigment cells.
- Nevus cells: Immature pigment cells (melanocytes at an intermediate stage of differentiation from the neural crest)
- Form cell nests (theques) in the conjunctival basal cell layer or subepithelium (subepithelial tissue)
- Most appear in childhood and stop growing and stabilize in adulthood
- Cyst formation: A characteristic histological feature of nevi. Formed by cystic embedding of epithelium, providing the histological basis for the tapioca-like appearance
Mechanism of color change with age
Section titled “Mechanism of color change with age”The reason why nevi in children appear reddish and melanin pigment becomes clearer after growth is that the melanin-producing ability of nevus cells matures with age. In early childhood, even if many nevus cells are present, melanin production is insufficient, so they appear red to light brown. As they grow, melanin synthesis ability increases, and the dark brown color becomes clear.
Continuity with PAM and malignant melanoma
Section titled “Continuity with PAM and malignant melanoma”- PAM (Primary Acquired Melanosis): Patchy pigmentation due to intraepithelial proliferation of melanocytes. PAM with atypia is a precursor lesion of malignant melanoma
- Malignant transformation from nevus: Rare (about 1%), but malignant melanoma can arise directly from a nevus1)
- Origin of conjunctival malignant melanoma: PAM 60–75%, de novo about 19%, nevus 7–20%2)
Histological classification (types of nevi)
Section titled “Histological classification (types of nevi)”Nevi are histologically classified as follows4).
- Junctional nevus: Nevus cells confined to the epithelial basal layer
- Subepithelial nevus: Nevus cells present in the subepithelial tissue
- Compound nevus: Nevus cells present in both the epithelial basal layer and subepithelial tissue
- Blue nevus: Spindle-shaped cells with pigment are present in the deep subepithelium
7. Latest Research and Future Perspectives
Section titled “7. Latest Research and Future Perspectives”Improved Diagnostic Accuracy with Immunohistochemistry Panels
Section titled “Improved Diagnostic Accuracy with Immunohistochemistry Panels”Conjunctival melanocytic proliferative lesions previously classified as “indeterminate” are becoming reclassifiable through combined evaluation of immunohistochemistry panels (PRAME, p16, HMB45, Ki-67, etc.). In particular, PRAME is attracting attention as the most powerful differential marker, being negative in nevi and positive in malignant melanoma5).
Non-invasive Diagnosis with Confocal Microscopy
Section titled “Non-invasive Diagnosis with Confocal Microscopy”Non-invasive real-time evaluation using confocal laser scanning microscopy (CLSM) is being researched. It may allow observation of cellular-level information (nuclear morphology, cell density) in living tissue that cannot be obtained by slit-lamp examination, and is expected to be applied to diagnosis that avoids biopsy.
Benign-Malignant Differentiation by FISH Analysis
Section titled “Benign-Malignant Differentiation by FISH Analysis”Fluorescence in situ hybridization (FISH) analysis can evaluate genomic changes such as RREB1 (6p25), CCND1 (11q13), MYB (6q23), and MYC (8q24), potentially predicting the malignant potential of histologically indeterminate lesions. In FISH analysis of deep penetrating nevus (DPN), all cases were positive for BRAF V600E and all negative for NRAS Q61R, advancing the elucidation of molecular characteristics of nevi5).
8. References
Section titled “8. References”-
Shields CL, Fasiuddin AF, Mashayekhi A, Shields JA.. Conjunctival nevi: clinical features and natural course in 410 consecutive patients. Arch Ophthalmol. 2004;122(2):167-175. doi:10.1001/archopht.122.2.167. PMID:14769591.
-
Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol. 2004;49(1):3-24. doi:10.1016/j.survophthal.2003.10.008.
-
Shields CL, Shields JA, Augsburger JJ. Conjunctival nevi. Int Ophthalmol Clin. 1993;33(3):35-44.
-
Jakobiec FA, Folberg R, Iwamoto T.. Clinicopathologic characteristics of premalignant and malignant melanocytic lesions of the conjunctiva. Ophthalmology. 1989;96(2):147-166. doi:10.1016/s0161-6420(89)32920-4. PMID:2649838.
-
Kenawy N, Lake SL, Coupland SE, Damato BE.. Conjunctival melanoma and melanocytic intra-epithelial neoplasia. Eye (Lond). 2013;27(2):142-152. doi:10.1038/eye.2012.254. PMID:23222568; PMCID:PMC3574254.