Eyelid papilloma is a benign epithelial tumor in which tumor cells proliferate like leaves on a branch of tumor blood vessels. It is also called squamous cell papilloma or simple papilloma. Human papillomavirus (HPV) is involved in its development, and it can occur in multiple lesions.
Lesions on the eyelid skin are non-ulcerated and may be pedunculated. They grow in a leafy pattern, with a keratinized surface and vascular fibrous tissue. Those near the eyelid margin have less keratinization and appear reddish.
Among benign eyelid tumors by pathological diagnosis, papilloma accounts for 6 out of 64 eyes (9%), making it the fourth most common tumor. HPV may be involved in its development, and some cases show a tendency for multiple lesions. It occurs in both children and adults, and immunocompromised patients have a higher risk of multiple lesions and recurrence 1).
Regarding HPV involvement, studies of conjunctival papilloma have shown that HPV types 6 and 11 are mainly involved as low-risk types 1). HPV types 16 and 18 are high-risk types and have been associated with malignant transformation 2).
Eyelid papillomas are classified into the following two types based on growth pattern.
Pedunculated papilloma: A type that grows from the conjunctival surface via a thin vascular stalk. Most common.
Sessile papilloma: A type that grows with a broad base. Requires differentiation from squamous cell carcinoma.
QIs eyelid papilloma contagious?
A
HPV may be involved in the development, and theoretically, contact transmission is possible. However, the risk of transmission between eyelids through normal daily contact is low. In immunocompromised states (e.g., after organ transplantation, HIV infection), the risk of multiple occurrences and recurrence is reported to be higher. It is recommended to see an ophthalmologist for multiple or rapidly growing lesions on the eyelid.
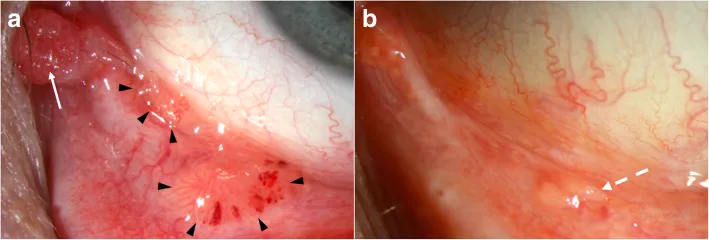
Theotoka D, et al. Update on Diagnosis and Management of Conjunctival Papilloma. Eye Vis (Lond). 2019;6:18. Figure 4. PMCID: PMC6580461. DOI: 10.1186/s40662-019-0142-5. License: CC BY 4.0.
Pedunculated and sessile conjunctival papillomas arising on the eyelid and lacrimal caruncle of a 51-year-old man, with spontaneous intratumoral hemorrhage in the eyelid lesion (arrowhead). Corresponds to the clinical findings of pedunculated and sessile papillomas discussed in the section “2. Main symptoms and clinical findings”.
The clinical findings of eyelid papilloma differ depending on whether it is pedunculated or sessile.
Pedunculated papilloma
Pink cauliflower-like mass: Forms a pink, finely lobulated cauliflower-like mass.
Attachment by a thin vascular stalk: Because it is pedunculated, the area of attachment to the palpebral conjunctival surface is smaller than it appears. It grows in a frond-like pattern, and the surface is composed of keratinized, vascular-rich fibrous tissue. Lesions near the eyelid margin are less keratinized and appear reddish.
Sessile papilloma
Broad-based growth: The base of the tumor is wide and attaches to the palpebral conjunctival surface. Clinically, it may be difficult to distinguish from squamous cell carcinoma.
Rarely, malignant transformation can occur; rapid enlargement, bleeding, or ulceration of the lesion warrants further investigation.
QCan eyelid papilloma become malignant?
A
Rarely, malignant transformation (squamous cell carcinoma) is known to occur. Broad-based growth pattern, rapid enlargement, surface bleeding or ulceration, and the appearance of corkscrew tumor vessels are findings suspicious for malignancy. Pathological examination after excision is essential for definitive diagnosis, and regular follow-up is also important.
The main cause of eyelid papilloma is HPV infection.
HPV types 6 and 11: Low-risk HPV types. They are involved in the majority of conjunctival and eyelid papillomas1). Main cause of benign papillomas.
HPV types 16 and 18: High-risk HPV types. Infection of the ocular surface is less common, but the risk of malignant transformation is high2).
Immunosuppressed state: After organ transplantation, HIV infection, or hematologic malignancies, the risk of multiple or recurrent papillomas is significantly increased2). This is thought to be due to suppressed host immunity against HPV.
Occurrence in children: In children, conjunctival and eyelid papillomas may coexist1). Differences in immune response compared to adults may affect the development and course of papillomas.
Sessile growth → Requires differentiation from squamous cell carcinoma
Histopathological examination of the excised specimen → Essential for definitive diagnosis
Sessile papilloma may resemble giant papillary conjunctivitis in appearance, making accurate clinical diagnosis difficult in some cases 3). A combination of detailed slit-lamp microscopy and histopathological examination is key to diagnosis.
Similar to sessile papilloma; history of allergies or contact lens use
After excision, the specimen must always be submitted for histopathological examination. Particularly for broad-based, rapidly growing lesions, malignancy should be considered.
QIs a biopsy necessary for papilloma?
A
As a rule, excised specimens must always be submitted for histopathological examination. Excisional biopsy provides a definitive diagnosis and helps avoid missing rare malignant components (malignant transformation to squamous cell carcinoma). Especially for lesions with broad-based growth, rapid enlargement, bleeding, or ulceration, malignancy should be strongly suspected, and early excisional biopsy is recommended.
Surgical excision is the first-line treatment for eyelid papilloma. Since simple excision alone tends to result in recurrence, the following steps are standard.
Excise the tumor base attached to the palpebral conjunctival surface and perform cautery hemostasis.
Apply two cycles of cryotherapy (freeze and thaw) to the excision site to prevent recurrence.
Always submit the excised specimen for histopathological examination.
Simple excision alone tends to result in recurrence. Adding cryotherapy can reduce the recurrence rate.
Subconjunctival interferon alpha-2b injection has been reported effective for recurrent and refractory conjunctival papilloma4). It is thought to reduce HPV-related lesions through local antiviral and immunostimulatory effects.
Oral cimetidine (H2 receptor antagonist) has been reported to have therapeutic effects on HPV-related skin lesions via immunomodulatory mechanisms and is sometimes used as an adjuvant therapy3).
The preventive effect of HPV vaccine (quadrivalent vaccine, Gardasil, etc.) against HPV types 6, 11, 16, and 18 is being investigated for the prevention of ocular surface papilloma 5).
QIs recurrence common after surgery?
A
Simple excision alone is known to have a high recurrence rate. To prevent recurrence, it is standard to add two sets of cryotherapy (freeze and thaw) to the excision margins. Patients who are immunocompromised have a particularly high risk of recurrence. For recurrent cases, additional treatments such as subconjunctival interferon alpha-2b injection may be considered.
Eyelid papilloma has a structural characteristic where tumor cells proliferate in a leaf-like pattern, branching from tumor blood vessels. The frond-like growth pattern results from cell proliferation around blood vessels. Histological features include surface keratinization and vascular-rich fibrous tissue.
Pedunculated papilloma results from exophytic growth of conjunctival epithelium, whereas sessile papilloma tends to show endophytic growth. This difference in growth pattern correlates with clinical prognosis (benign vs. malignant potential).
HPV types 6 and 11 are low-risk types involved in the majority of eyelid and conjunctival papillomas 1). The E6 and E7 proteins expressed by these viruses are involved in host cell growth regulation and promote neoplastic proliferation through persistent infection 2).
On the other hand, HPV types 16 and 18 are high-risk types that promote malignant transformation of cells through degradation of p53 by E6 protein and inactivation of Rb protein by E7 protein 2). The involvement of these high-risk HPV types is suspected in the rare malignant transformation of eyelid papilloma to squamous cell carcinoma.
Host cell-mediated immunity plays an important role in controlling HPV infection. In immunocompromised states such as after organ transplantation, HIV infection, or hematologic malignancies, the immune response to HPV is reduced, leading to increased occurrence, recurrence, and enlargement of papillomas 2). Management of eyelid papilloma in immunocompromised patients requires regular ophthalmologic evaluation alongside treatment of the underlying disease.
The possibility of applying HPV vaccines (especially the quadrivalent and 9-valent vaccines) to prevent eyelid and conjunctival papillomas caused by HPV types 6 and 11 is being investigated 5). Vaccines developed for cervical cancer prevention may also be effective in preventing papilloma development in the ophthalmic field, but large-scale clinical trials in ophthalmology have not yet been established.
Cidofovir is an antiviral drug being considered for application to HPV-related lesions. It is not a standard treatment for ocular surface papilloma and remains an investigational option for cases that are difficult to control with existing treatments 6).
Photodynamic therapy has been reported in a small number of cases for refractory papilloma 6). Research on the efficacy of PDT for HPV-related epithelial tumors is still ongoing.
Schechter BA, Rand WJ, Velazquez GE, Williams WD, Starasoler L. Treatment of conjunctival papillomata with topical interferon Alfa-2b. Am J Ophthalmol. 2002;134(2):268-270. doi:10.1016/S0002-9394(02)01514-3.
Yıldız ZÖ, Erdem E. Ocular papilloma and HPV vaccines: a review. Turk J Ophthalmol. 2022;52(3):206-210.
Kaliki S, Arepalli S, Shields CL, et al. Update on diagnosis and management of conjunctival papilloma. Eye Vis (Lond). 2019;6:18. doi:10.1186/s40662-019-0142-5.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.